Prevalence and associated factors of human haemorrhagic fevers in Senegal: a comprehensive analysis of Hantaan, Crimean-Congo haemorrhagic fever and Rift Valley fever
Maryam Diarra, Safietou Sankhe, Mamadou Aliou Barry, Fatoumata Diene Sarr, Mamadou Korka Kindy Diallo, Joseph Faye, Mame Astou Gassama, Maimouna Mbanne, Ousmane Faye, Cheikh Talla, Robab Katani, Keersten Ricks, Moussa Moise Diagne, Jessica Radzio-Basu, Cheikh Loucoubar

TL;DR
The study found that human exposure to several viral haemorrhagic fevers is common in Senegal, with most cases going undetected by current surveillance systems.
Contribution
This study provides the first serological evidence of human hantavirus exposure in Senegal and highlights significant under-detection of infections.
Findings
Seroprevalence rates were 15.1% for Rift Valley fever virus, 10.8% for Crimean-Congo haemorrhagic fever virus, and 2.2% for Hantaan virus.
Exposure to Rift Valley fever was higher in the transboundary region Matam, while exposure to the other two viruses was higher in Thiès.
Routine surveillance systems detected only a small fraction of infections, indicating widespread under-detection.
Abstract
Viral haemorrhagic fevers such as Rift Valley fever, Crimean-Congo haemorrhagic fever, and hantavirus disease continue to threaten public health in Africa. This study assessed the seroprevalence and associated factors of these infections in Senegal. A cross-sectional survey was conducted from September 2022 to June 2024 among asymptomatic individuals living in close contact with livestock in two regions: Matam, a transboundary area; and Thiès, a non-transboundary area with high livestock density. Participants completed standardized questionnaires, and serum samples were screened for antibodies against Rift Valley fever virus, Crimean-Congo haemorrhagic fever virus, and Hantaan virus using a Luminex-based multiplex immunoassay. Logistic regression models were used to identify independent risk factors. Among 2,019 participants, crude seroprevalence was 15.1 percent (95 percent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1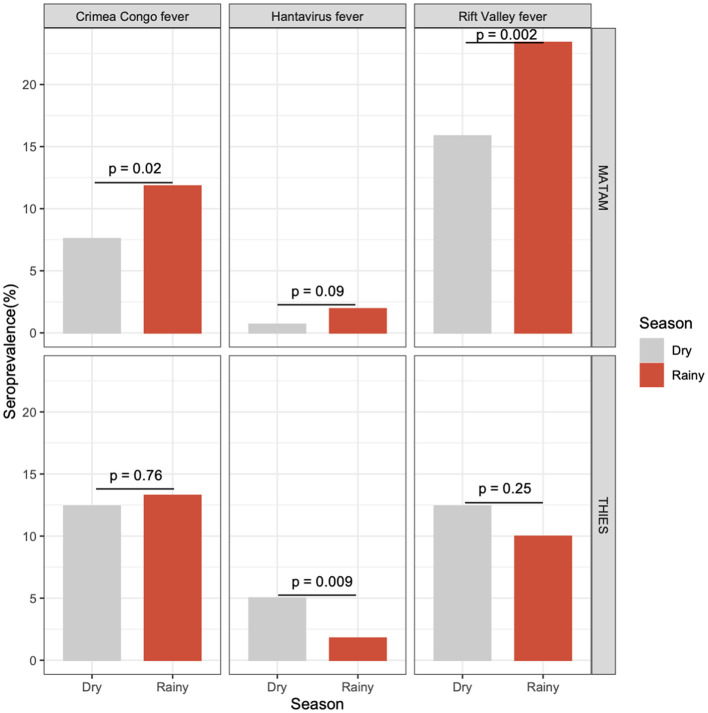 Figure 2
Figure 2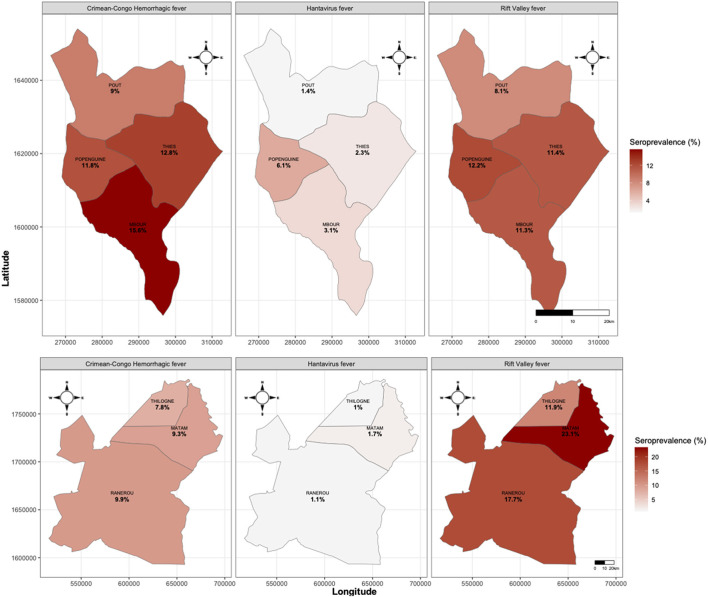 Figure 3
Figure 3|
|
|
|
|
| ||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |||
| Matam | Rainy | Sept 22–Oct 06, 2022 | 251 | 17.62 | 8.20 | 0.00 | 1 | 1 |
| Sept 24–Oct 01, 2023 | 226 | 29.91 | 16.14 | 4.48 | - | - | ||
| Dry | May 22–30, 2023 | 267 | 16.33 | 9.16 | 0.00 | - | - | |
| May 22–June 1, 2024 | 332 | 15.50 | 6.38 | 1.22 | - | - | ||
| Thies | Rainy | Nov 09–20, 2022 | 260 | 14.29 | 15.52 | 2.63 | - | - |
| Sept 17–23, 2023 | 224 | 5.36 | 10.71 | 0.89 | - | - | ||
| Dry | Jun 04–11, 2023 | 254 | 15.35 | 13.39 | 3.94 | - | - | |
| May 27–June 6, 2024 | 205 | 8.82 | 11.27 | 6.37 | - | - | ||
|
| ||||||||
| Total | 11 | 63 | 19 | 19 | ||||
|
|
|
|
|
|
|
| ||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |||||
| Sex | Female | 1,008 (49.9) | 126 | 12.5 | - | - | - | |||
| Male | 1,003 (49.7) | 176 | 17.5 | 1.49 | [1.16; 1.91] | 0.002 | 1.7 | [1.3; 2.21] | <0.001 | |
| Missing | 8 (0.4) | 2 | 25 | |||||||
| Age Group | [0–15] | 372 (18.4) | 38 | 10.2 | - | - | - | |||
| [15–45] | 1,013 (50.2) | 126 | 12.4 | 1.25 | [0.85; 1.83] | 0.257 | 1.32 | [0.89; 1.98] | 0.168 | |
| [45–65] | 457 (22.6) | 102 | 22.3 | 2.53 | [1.69; 3.77] | <0.001 | 2.72 | [1.79; 4.13] | <0.001 | |
| [65–98] | 130 (6.4) | 30 | 23.1 | 2.64 | [1.55; 4.47] | <0.001 | 2.95 | [1.7; 5.09] | <0.001 | |
| Missing | 47 (2.3) | 8 | 17 | |||||||
| Region | Thies | 943 (46.7) | 102 | 10.8 | - | - | - | |||
| Matam | 1,076 (53.3) | 202 | 18.8 | 1.91 | [1.47; 2.46] | <0.001 | 2.21 | [1.68; 2.91] | <0.001 | |
| Year | Year 1 | 1,032 (51.1) | 156 | 15.1 | - | - | - | |||
| Year 2 | 987 (48.9) | 148 | 15 | 0.99 | [0.78; 1.26] | 0.939 | ||||
| Season | Dry | 1,059 (52.5) | 149 | 14.1 | - | - | - | |||
| Rainy | 955 (47.3) | 154 | 16.1 | 1.17 | [0.92; 1.5] | 0.198 | ||||
| Missing | 5 (0.2) | 1 | 20 | |||||||
| Profession | Others | 375 (18.6) | 60 | 16 | - | - | - | |||
| Student–Teachers | 299 (14.8) | 29 | 9.7 | 0.56 | [0.35; 0.9] | 0.017 | ||||
| Breeders | 609 (30.2) | 112 | 18.4 | 1.18 | [0.84; 1.67] | 0.338 | ||||
| Housewives | 503 (24.9) | 69 | 13.7 | 0.83 | [0.57; 1.21] | 0.345 | ||||
| Medical-staff | 76 (3.8) | 7 | 9.2 | 0.53 | [0.23; 1.22] | 0.134 | ||||
| Slaughterhouse-staff | 126 (6.2) | 24 | 19 | 1.24 | [0.73; 2.08] | 0.429 | ||||
| Milk sellers | 31 (1.5) | 3 | 9.7 | 0.56 | [0.17; 1.91] | 0.356 | ||||
| Contact with animal | No | 64 (3.2) | 7 | 10.9 | - | - | - | |||
| Yes | 1,914 (94.8) | 291 | 15.2 | 1.46 | [0.66; 3.23] | 0.351 | ||||
| Missing | 41 ( | 6 | 14.6 | |||||||
| Raw milk consumption | No | 294 (14.6) | 45 | 15.3 | - | - | - | |||
| Yes | 1,688 (83.6) | 254 | 15 | 0.98 | [0.69; 1.38] | 0.909 | ||||
| Missing | 37 (1.8) | 5 | 13.5 | |||||||
| Use protective equipment | No | 1,929 (95.5) | 299 | 15.5 | - | - | - | |||
| Yes | 45 (2.2) | 2 | 4.4 | 0.25 | [0.06; 1.05] | 0.059 | ||||
| Missing | 45 (2.2) | 3 | 6.7 | |||||||
|
|
|
|
|
|
|
| ||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |||||
| Sex | Female | 1,008 (49.9) | 73 | 7.2 | - | - | - | |||
| Male | 1,003 (49.7) | 144 | 14.4 | 2.15 | [1.6; 2.89] | <0.001 | 1.9 | [1.39; 2.61] | <0.001 | |
| Missing | 8 (0.4) | 0 | 0 | |||||||
| Age Group | [0–15] | 372 (18.4) | 21 | 5.6 | - | - | - | |||
| [15–45] | 1,013 (50.2) | 79 | 7.8 | 1.41 | [0.86; 2.32] | 0.172 | 1.4 | [0.84; 2.33] | 0.199 | |
| [45–65] | 457 (22.6) | 78 | 17.1 | 3.44 | [2.08; 5.69] | <0.001 | 3.27 | [1.95; 5.48] | <0.001 | |
| [65–98] | 130 (6.4) | 33 | 25.4 | 5.69 | [3.15; 10.27] | <0.001 | 5.42 | [2.96; 9.93] | <0.001 | |
| Missing | 47 (2.3) | 6 | 12.8 | |||||||
| Region | Matam | 943 (46.7) | 117 | 12.4 | - | - | - | |||
| Thies | 1,076 (53.3) | 100 | 9.3 | 0.72 | [0.55; 0.96] | 0.025 | 0.84 | [0.62; 1.14] | 0.264 | |
| Year | Year 1 | 1,032 (51.1) | 113 | 10.9 | - | - | - | |||
| Year 2 | 987 (48.9) | 104 | 10.5 | 0.96 | [0.72; 1.27] | 0.765 | ||||
| Season | Dry | 1,059 (52.5) | 101 | 9.5 | - | - | - | |||
| Rainy | 955 (47.3) | 115 | 12 | 1.3 | [0.98; 1.72] | 0.07 | ||||
| Missing | 5 (0.2) | 1 | 20 | |||||||
| Profession | Others | 375 (18.6) | 32 | 8.5 | - | - | - | |||
| Student-Teachers | 299 (14.8) | 13 | 4.3 | 0.49 | [0.25; 0.95] | 0.034 | ||||
| Breeders | 609 (30.2) | 106 | 17.4 | 2.26 | [1.49; 3.43] | <0.001 | ||||
| Housewives | 503 (24.9) | 34 | 6.8 | 0.78 | [0.47; 1.28] | 0.325 | ||||
| Medical-staff | 76 (3.8) | 4 | 5.3 | 0.6 | [0.2; 1.74] | 0.342 | ||||
| Slaughterhouse-staff | 126 (6.2) | 22 | 17.5 | 2.27 | [1.26; 4.07] | 0.006 | ||||
| Milk sellers | 31 (1.5) | 6 | 19.4 | 2.57 | [0.98; 6.73] | 0.054 | ||||
| Contact with animal | No | 64 (3.2) | 7 | 10.9 | - | - | - | |||
| Yes | 1,914 (94.8) | 206 | 10.8 | 0.98 | [0.44; 2.18] | 0.965 | ||||
| Missing | 41 (2) | 4 | 9.8 | |||||||
| Raw milk consumption | No | 294 (14.6) | 20 | 6.8 | - | - | - | |||
| Yes | 1,688 (83.6) | 190 | 11.3 | 1.74 | [1.08; 2.8] | 0.024 | 1.85 | [1.13; 3.03] | 0.014 | |
| Missing | 37 (1.8) | 7 | 18.9 | |||||||
| Use protective equipment | No | 1,929 (95.5) | 203 | 10.5 | - | - | - | |||
| Yes | 45 (2.2) | 4 | 8.9 | 0.83 | [0.29; 2.34] | 0.724 | ||||
| Missing | 45 (2.2) | 10 | 22.2 | |||||||
|
|
|
|
|
|
|
| ||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |||||
| Sex | Female | 1,008 (49.9) | 19 | 1.9 | - | - | - | |||
| Male | 1,003 (49.7) | 26 | 2.6 | 1.39 | [0.76; 2.52] | 0.286 | ||||
| Missing | 8 (0.4) | 0 | 0 | |||||||
| Age Group | [0–15] | 372 (18.4) | 3 | 0.8 | - | - | - | |||
| [15–45] | 1,013 (50.2) | 24 | 2.4 | 2.98 | [0.89; 9.97] | 0.076 | 4.53 | [1.06; 19.25] | 0.041 | |
| [45–65] | 457 (22.6) | 13 | 2.8 | 3.6 | [1.02; 12.73] | 0.047 | 4.87 | [1.08; 21.92] | 0.039 | |
| [65–98] | 130 (6.4) | 3 | 2.3 | 2.91 | [0.58; 14.58] | 0.195 | 3.88 | [0.64; 23.55] | 0.141 | |
| Missing | 47 (2.3) | 2 | 4.3 | |||||||
| Region | Matam | 1,076 (53.3) | 14 | 1.3 | - | - | - | |||
| Thies | 943 (46.7) | 31 | 3.3 | 2.58 | [1.36; 4.88] | 0.004 | 2.52 | [1.29; 4.89] | 0.007 | |
| Year | Year 1 | 1,032 (51.1) | 16 | 1.6 | - | - | - | |||
| Year 2 | 987 (48.9) | 29 | 2.9 | 1.92 | [1.04; 3.56] | 0.038 | ||||
| Season | Dry | 1,059 (52.5) | 27 | 2.5 | - | - | - | |||
| Rainy | 955 (47.3) | 17 | 1.8 | 0.69 | [0.38; 1.28] | 0.241 | ||||
| Missing | 5 (0.2) | 1 | 20 | |||||||
| Profession | Others | 375 (18.6) | 8 | 2.1 | - | - | - | |||
| Student-Teachers | 299 (14.8) | 3 | 1 | 0.46 | [0.12; 1.77] | 0.261 | ||||
| Breeders | 609 (30.2) | 20 | 3.3 | 1.56 | [0.68; 3.57] | 0.295 | ||||
| Housewives | 503 (24.9) | 8 | 1.6 | 0.74 | [0.28; 1.99] | 0.553 | ||||
| Medical-staff | 76 (3.8) | 0 | 0 | 0 | [0; Inf] | 0.984 | ||||
| Slaughterhouse-staff | 126 (6.2) | 4 | 3.2 | 1.5 | [0.45; 5.08] | 0.511 | ||||
| Milk sellers | 31 (1.5) | 2 | 6.5 | 3.16 | [0.64; 15.59] | 0.157 | ||||
| Contact with animal | No | 64 (3.2) | 1 | 1.6 | - | - | - | |||
| Yes | 1,914 (94.8) | 44 | 2.3 | 1.48 | [0.2; 10.92] | 0.699 | ||||
| Missing | 41 (2) | 0 | 0 | |||||||
| Raw milk consumption | No | 294 (14.6) | 5 | 1.7 | - | - | - | |||
| Yes | 1,688 (83.6) | 39 | 2.3 | 1.37 | [0.53; 3.5] | 0.514 | ||||
| Missing | 37 (1.8) | 1 | 2.7 | |||||||
| Use protective equipment | No | 1,929 (95.5) | 44 | 2.3 | ||||||
| Yes | 45 (2.2) | 0 | 0 | |||||||
| Missing | 45 (2.2) | 1 | 2.2 | |||||||
- —Defense Threat Reduction Agency10.13039/100000774
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Vectors · Viral Infections and Outbreaks Research · Vector-Borne Animal Diseases
Introduction
Emerging and re-emerging zoonotic diseases such as Rift Valley Fever (RVF), Crimean Congo Haemorrhagic Fever (CCHF) and hantaviruses infection (HTN) pose major global health threats. Climatic and environmental changes, human encroachment into wildlife habitats, and intensified livestock movements are disrupting ecosystems, facilitating the spillover of animal pathogens to humans. Globally, up to half of human infectious diseases are zoonotic in origin, many maintained in wild reservoirs (1, 2). Understanding these dynamics is essential to prevent future outbreaks in vulnerable regions such as West Africa.
Rift Valley fever virus (RVFV) and Crimean-Congo haemorrhagic fever virus (CCHFV) are vector-borne RNA viruses transmitted mainly by mosquitoes (3–5) and ticks (6). Human infection typically occurs through bites or contact with infected animal tissues. Both viruses are endemic in West Africa and are increasingly associated with livestock infections (7, 8). In contrast, hantaviruses are rodent-borne viruses transmitted to humans primarily through the inhalation of aerosolized rodent excreta, and cause haemorrhagic fever with renal syndrome (HFRS) or hantavirus pulmonary syndrome (HPS), both associated with substantial morbidity and mortality (8, 9).
In Senegal, RVF was first reported during the 1987–88 epidemic near the Mauritanian border (10). Since then, RVFV transmission has been documented mainly in ruminants from the northern part of the country and in the Ferlo region. Subsequent outbreaks occurred in 2003 and 2013, with the latter marking the first detection of urban and peri-urban human cases in Dakar and Thiès (11, 12). Between 2020 and 2022, 13 human cases were reported in several regions of the country, including Matam, Saint-Louis, Fatick and Dakar, while a 2021 serosurvey in Matam revealed a human IgG prevalence of 20.8% and livestocks seroprevalence exceeding 60% (13–15).
Senegal has also reported widespread circulation of CCHFV in humans, livestock and ticks across multiple regions (15, 16). Between March and September 2023, eight confirmed human CCHF cases were identified in five regions, followed later that year by an additional eleven cases across seven regions (17, 18).
Serological evidence of human hantavirus exposure has now been reported in Senegal from samples collected between 2019 and 2022, marking the first identification in human samples with approximately 1 percent Hantaan virus (HTNV) IgG (19) alongside prior detection of Seoul orthohantavirus in wild black rats captured in 2012–2013 (20), highlighting the need for strengthened surveillance.
Early detection of zoonotic viruses with epidemic potential remains challenging due to asymptomatic subclinical infections, limited diagnostic capacity, and incomplete understanding of human and environmental risk factors. Despite recurrent outbreaks, few studies have systematically assessed human exposure and associated risk factors for multiple haemorrhagic fever viruses in Senegal. Data remain particularly scarce for transboundary pastoral areas, where close human–animal contact and seasonal livestock movements may facilitate viral spillover.
Accordingly, this study aimed to determine the seroprevalence of Rift Valley fever, Crimean-Congo haemorrhagic fever, and hantavirus infections in high-risk populations and to identify associated factors in both transhumant and sedentary communities of Senegal.
Materials and methods
We conducted a repeated cross-sectional study between September 2022 and June 2024 to assess the seroprevalence of RVF, CCHF, and hantavirus infections in humans across different seasons and epidemiological settings in Senegal.
Study sites
Two sites in Senegal were selected to compare transboundary and non-transboundary regions with differing ecological and epidemiological profiles (Figure 1). The Matam region, located in north-eastern Senegal along the borders with Mauritania and Mali, represents a transboundary pastoral ecosystem characterized by arid landscapes and extensive seasonal livestock movements. During the dry season, transhumant herders migrate southward in search of pastures, returning north during the rainy season (21).
Study sites. Map of Senegal indicating selected study regions (in red). Other Senegalese regions are represented in white.
In contrast, the Thiès region, situated in western Senegal, is a non-transboundary area with high human population density and substantial livestock holdings. It has a history of zoonotic outbreaks and is influenced by peri-urban farming practices that promote close contact between animals and humans. Recent studies have detected RVFV in local livestock (12) and CCHFV in both ticks and animals in the area, with human cases occurring within a 5 km radius (22). In addition, bat colonies known to harbor zoonotic viral pathogens are also present in the vicinity (23).
Ethical considerations
Participants at high risk for zoonotic transmission in these regions were identified and invited to participate. All participants consented to participate in the study. For those younger than 15 years of age, a legal representative provided informed consent. The study was approved by the Senegalese National Ethics Committee for Research in Health (reference number N°000242/MSAS/DPRS/CNERS/SP, 07 September 2022).
Sample size calculation
Based on IgG antibodies, a recent study conducted in Senegal in 2021 estimated a human prevalence of 20.8% (24). Based on this, with an absolute error of ±5%, a power of 90%, a sample size of 253 individuals was needed in each study site and each survey. This power and precision were selected to ensure reliable regional comparisons and to detect at least a 5 percent difference in seroprevalence between study sites or survey rounds. Overall, from September 2022 to June 2024, the total sample size targeted for both regions were estimated to be 2,024 individuals.
Data collection and blood sampling
A cross-sectional study of asymptomatic individuals was conducted in Matam, in the north of the country, and Thies, in the west. The aim was to compare the Matam region, which has a transhumant population with significant movement of animals and people, with the Thies region, which has a more stable population but a high livestock density. The target population included individuals living in close contact with livestock, such as livestock farmers, slaughterhouse workers, and butchers.
For each participant, a whole blood sample was collected in a dry Vacutainer tube using standard venipuncture procedures, and a structured risk-exposure questionnaire was completed to capture demographic characteristics, occupational data, animal contact, and travel history. Blood samples were immediately stored at 4 °C and transported to the Institut Pasteur de Dakar for laboratory testing. Field investigation forms were checked for accuracy before data entry and subsequently stored in a centralized electronic MySQL database. The collected information included age, sex, occupation, residence, animal exposure, and travel history.
Laboratory testing
Serum samples were screened for immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies against RVFV, CCHFV, and HTNV using a Luminex-based multiplex magnetic-bead immunoassay (MAGPIX, Luminex Corp). For each viral target, the nucleoprotein antigen was coupled to distinct microsphere sets to capture virus-specific antibodies. This multiplex assay was verified using animal models and known IgG-positive human samples (25, 26), and later validated for RVFV and CCHFV (23). This confirmed its suitability for large-scale surveillance in Senegal, showing good agreement with reference serological methods.
In brief, serum samples were heat-inactivated for 30 min at 37 °C and diluted 1:100 in PBST-SK (phosphate-buffered saline with 0.02 percent Tween 20 and 5 percent skim milk). The magnetic-bead mix was diluted 1:250 in PBST and dispensed into 96-well plates along with diluted samples, positive controls (known IgG/IgM-positive convalescent sera), and negative controls. Plates were incubated for 1 h, washed, and then incubated with anti-human IgG-PE or IgM-PE conjugates diluted 1:100 in PBST-SK. After final washing, 100 μL of PBST was added to each well, and fluorescence was read on the MAGPIX instrument.
Samples were considered positive when the mean fluorescence intensity exceeded 20 times that of the negative control, a threshold established through cross-validation with microneutralization assays on an independent Ghanaian cohort. As previously described, the MAGPIX platform was used here as a fixed-dilution qualitative screening assay for IgG and IgM detection. Because the assay does not include antibody titration curves, it does not allow quantitative interpretation of IgM/IgG ratios or timing of infection. Its intended purpose in this study is the identification of past exposure rather than dating of immune responses.
Data analysis
Crude seroprevalence rates were calculated with the 95% confidence interval (CI). The 95% CI for seroprevalence were estimated using a binomial distribution.
We evaluated potential risk factors for RVF, CCHF and HTN, including region, sex, age group [(under 15], (15–45], (45–65], (65–98] years-old], season of sample collection (dry season, rainy season), occupation (breeders, student and/or teachers, housewives, medical staff, slaughterhouse staff and milk sellers, as well as other non-listed occupations), contact with wild animals, raw milk consumption and the use of protective equipment when handling animals. Fisher's exact test was used to compare the seroprevalence of RVFV (respectively CCHFV, HTNV) between the rainy and dry season.
Statistical analysis was performed for each disease using univariate binary logistic regression models. Significant variables from the univariate analysis were incorporated into the multivariable binary logistic regression analysis to evaluate the statistical significance of the association between the independent and response variables using adjusted odds ratios (AOR), 95% confidence intervals (CI) for AOR and p-values. A backward selection procedure was then applied to identify the variables that remained significant at the 0.05 level in the final model.
All statistical analyses and mapping were carried out using the R statistical language (25) version 4.0.4 within Rstudio (Version 1.2.1335).
Syndromic sentinel surveillance network in senegal (4S network)
To complement serological findings, data from the national 4S (Syndromic Sentinel Surveillance) system were reviewed to identify confirmed human cases of RVF and CCHF reported during the study period. The 4S network, coordinated by the Senegalese Ministry of Health and the Institut Pasteur de Dakar since 2011, monitors epidemic-prone diseases through a network of sentinel health facilities across the country (24, 26).
Results
Between 2022 and 2024, eight seroprevalence surveys were conducted. Four surveys were carried out at each site: two during the rainy season and two during the dry season (Table 1). A total of 38 sites (16 in Matam and 22 in Thies) provided 2,019 participants during this time period: 1,076 from Matam and 948 from Thies.
Among the viral haemorrhagic fevers investigated, RVF was the most prevalent, followed by CCHF and HTN. The estimated crude seroprevalence was 15.06% (95%CI = 13.52–16.69) for RVF, 10.75% (95%CI = 9.43–12.18) for CCHF and 2.23% (95%CI = 1.63–2.97) for HTN.
For RVF, seroprevalence was significantly higher in Matam (19.27%) than in Thies (11.17%) (Fisher's exact test p-value < 0.001). For CCHF, seroprevalence was significantly higher in Thies (12.8%) than in Matam (9.55%) (Fisher's exact test p-value = 0.025). For HTN, seroprevalence was significantly higher in Thies (3.41%) than in Matam (1.34%) (Fisher's exact test p-value = 0.002) (Table 1). Co-infections between different viruses were also observed in the tested samples: 11 samples tested positive for RVFV, CCHFV and HNTV; 63 samples tested positive for FVRV and CCHFV; 19 samples tested positive for RVFV and HNTV; and 19 samples tested positive for CCHFV and HNTV (Table 1).
Regionally, we observed that in Matam, seroprevalence was significantly higher during the rainy season than the dry season for RVF (p = 0.002) and CCHF (p = 0.02). However, in Thies, the differences in seroprevalence observed between the dry and rainy seasons were not statistically significant for RVF or CCHF. For HTN, seroprevalence was significantly higher in the dry season than in the rainy season in Thies (Figure 2).
Seroprevalence comparison between rainy and dry season. Haemorrhagic fever viruses (HFVs) are represented in column. The first line panel represent seroprevalence for each HFVs in Matam. The second line panel represent seroprevalence for each HFVs in Thies. Gray bars represent the dry season and red one the rainy season.
Regarding the distribution of seroprevalence by health district, RVF was the most widespread, being present in all surveyed districts. The highest seroprevalences were recorded in the Matam district (23.38%), followed by the Ranerou district (17.7%), the Popenguine district (12.2%) and the Thilogne health district (11.9%). The highest CCHF seroprevalence was found in the Mbour health district (15.6%), followed by the Thies health district (12.8%), the Popenguine health district (11.8%). For HTN, the highest seroprevalence values were particularly observed in Popenguine (6.1%), Mbour (3.1%) and Thies health districts (Figure 3).
Spatial distribution of Haemorrhagic fever viruses seroprevalence at district level.
For RVF, factors significantly associated with infection included gender, age group and region. During the entire study period, the odds of being infected by RVFV were higher among participants over 45 years old compared with those under 15 years old (AOR = 2.72, 95% CI = 1.79–4.13, p <0.001 for 45–64 years old and AOR = 2.95, 95% CI = 1.7–5.09, p <0.001 for over 65 years old). RVFV infection was 1.7 times higher in men than in women (AOR = 1.7, 95% CI = 1.3–2.21, p <0.001). Participants living in Matam region were 2.21 times more likely to be infected with RVFV than those living in Thies region (AOR = 2.21, 95% CI = 1.68–2.91, p <0.001) (Table 2).
Analysis of CCHFV exposure showed significant associations with gender, age group, consumption of raw milk and certain occupations. Compared with women, men were 1.9 times more likely to be infected by CCHFV (AOR = 1.9, 95% CI = 1.39–2.61, p <0.001). Compared with participants younger than 15 years old, the odds of being infected by CCHFV were significantly higher among participants aged 45–64 years old (AOR = 3.27, 95% CI = 1.95–5.48, p <0.001) and those aged 65 years or older (AOR = 5.42, 95% CI = 2.96–9.93, p <0.001). Participants who reported consuming raw milk also had higher odds of infection (AOR = 1.85, 95% CI = 1.13–3.03, p <0.014). Occupational exposure further influenced risk, with significantly higher odds among slaughterhouse staff (OR = 2.27, 95% CI = 1.26–4.07, p = 0.006) and livestock breeders (OR = 2.26, 95% CI = 1.49–3.43, p <0.001) (Table 3).
In the case of hantaviruses, infection risk was primarily associated with age and region. Compared with participants under 15 years old, the odds of HNTV infection were higher among individuals aged 15–44 years (AOR = 34.53, 95% CI = 1.06–19.25, p = 0.041) and 45–64 years (AOR = 4.87, 95% CI = 1.08–21.92, p = 0.039). Participants living in the Thies region were 2.52 times more likely to be infected with HTNV than those living in the Matam region (AOR = 2.52, 95% CI = 1.29–4.89, p = 0.007) (Table 4).
Taken together, these results reveal widespread past exposure to RVFV, CCHFV, and hantaviruses in high-risk populations, despite the near absence of confirmed human cases through routine surveillance. Over the same period, the 4S network identified only one Rift Valley fever case and one Crimean-Congo haemorrhagic fever case in Matam, and none in Thiès (Table 1), suggesting that active transmission may be far more widespread and cryptic than indicated by routine case reporting.
Discussion
This study provides a comprehensive overview of the circulation and exposure patterns of three major viral haemorrhagic fevers, RVF, CCHF, and hantavirus infection, across contrasting ecological settings in Senegal. The results reveal sustained and widespread exposure to these pathogens, with distinct regional and seasonal trends that underline their endemic presence and the ongoing risk of spillover to humans. Our findings revealed higher prevalence rates of RVF and CCHF in Matam than those reported by Sankhe and colleagues (27) in the same region. This discrepancy may be attributed to differences in sampling strategies. Our study targeted high-risk populations, whereas Sankhe and colleagues selected households at random.
The high prevalence rates observed in this study indicate historical exposure to VHFs in both regions, confirming that RVF and CCHF remain endemic in Senegal. Beyond the well-studied health districts of Matam and Thilogne, this work provides new insight into virus circulation in Ranerou Ferlo, a zone marked by intense cross-border pastoral mobility between Senegal and Mauritania. In Mauritania where RVF is endemic, eight epidemics have been documented since 1987 (28), with human cases and associated deaths also reported in Nouakchott (29, 30).
For RVF specifically, seroprevalence in humans was significantly higher in Matam than in Thiès (Table 2). This difference likely reflects contrasting population dynamics and animal movement patterns: Matam functions as a transhumance corridor with extensive seasonal migration of livestock and herders, whereas Thiès hosts a more sedentary population. Such movements have long been associated with increased exposure risk, as pastoralists and their herds frequently encounter infected vectors in endemic areas. Indeed, previous studies have shown that migrating herds exhibit higher RVF antibodies levels than sedentary ones (31).
Gender, age, and occupation were consistent determinants of exposure. Men were about twice as likely as women to be seropositive for RVFV and CCHFV, consistent with their greater involvement in livestock handling, herding, and slaughter activities (Tables 2, 3). Similarly, seroprevalence increased with age, indicating cumulative exposure over time to infected vectors or animals. These trends align with previous studies in West and East Africa that have linked occupational and behavioral patterns to zoonotic virus transmission.
The higher CCHFV seroprevalence in Thiès may be linked to ecological conditions favorable to tick vectors. The presence of the Bandia Reserve, which hosts abundant wildlife–livestock interfaces and high tick densities (11), could maintain a natural transmission cycle independent of livestock movement. In Bandia, Senegal, a study conducted from 1986 to 1988 found a prevalence of anti-CCHF IgG of 3.2% in the human population (32). Similar hotspots have been described in semi-arid zones of Africa, where mixed ecosystems sustain long-term virus circulation (33).
The results of our study showed a statistically significant association between CCFHV infection and the consumption of raw or unpasteurised milk. These results should be interpreted with caution, as transmission of the virus through milk is not certain. Indeed, Studies conducted in Turkey have not detected any CCHFV RNA in milk samples from domestic animals (34). However, unpasteurised milk has been suggested as a possible route of exposure to CCHFV, particularly in regions where the virus circulates in livestock (35). Furthermore, documents and guidelines relating to risk assessment specifically advise against the use of unpasteurised milk in regions where the CCHFV is present, as a precautionary measure (36, 37).
The significant increase in RVF and CCHF seroprevalence observed in Matam during the rainy season may be explained by the higher abundance of mosquito vectors during this period. This point is consistent with a study conducted in Tanzania, which reported the highest RVF seroprevalence during the rainy season (38). Peaks in mosquito activity have also been shown to coincide with months of heavy rainfall (39). Furthermore, the elevated RVF and CCHF seroprevalence rates in Matam could be attributed to the seasonal increase in livestock density, as transhumant herders migrate northward during the rainy season (20).
Although no confirmed clinical cases of Hantavirus have been reported in Senegal, our study confirms human exposure to hantaviruses, consistent with recent serological evidence from Sankhe et al. (19), who also identified IgG reactivity to HTNV using the same validated Luminex multiplex assay. In the present study, average IgG seroprevalence reached 3.41% in the Thies region and 1.3% in the Matam, suggesting low but measurable exposure in both regions. These results extend earlier observations of Seoul orthohantavirus detected in Rattus rattus, indicating that multiple hantavirus lineages, both urban and sylvatic, may circulate in Senegal. Environmental conditions in the Thiès region, particularly around Popenguine and the Bandia Reserve, where extensive rodent diversity has been documented (over 1,200 individuals captured between 1975 and 2012), may facilitate such maintenance cycles and sporadic zoonotic spillover to humans (40). It is important to note that the MAGPIX assay, as implemented in this study, is a fixed-dilution qualitative platform not used to infer the timing of infection. Our conclusions focus on the geographical distribution and magnitude of hantavirus exposure rather than on the age of immune responses. This approach aligns with global hantavirus sero-epidemiology practices, in which IgG detection alone is considered sufficient for documenting population-level exposure (41).
It is essential to emphasize that during the two-year period of data collection, the 4S sentinel surveillance detected one case of RVF and one case of CCHF. This weak detection via the 4S system indicates that surveillance only scratches the surface compared to the serological prevalence rates observed in our study. This lack of detection can be explained by the fact that clinical cases are reported by healthcare facilities. However, in rural and pastoral contexts, access to healthcare remains limited, and mild or uncomplicated cases often go unreported. This underscores the importance of community-based surveillance systems capable of detecting weak epidemiological signals and providing early alerts to public health authorities.
The need to reinforce surveillance is underscored by the ongoing RVF outbreak currently affecting Senegal (42). This situation highlights the urgency of strengthening national surveillance systems through an integrated One Health approach that systematically links entomological, veterinary, and human (including community-level) monitoring. Expanding this framework to include livestock serosurveillance, wildlife and mosquito vector data from Matam and Thiès would provide valuable insight into transmission dynamics and ecological risk factors for CCHF, RVF and hantavirus infections. Incorporating predictive modeling and climate-based early warning tools will also be essential to anticipate outbreaks, guide vaccination or vector-control strategies, and mitigate future epidemic impacts across Senegal and the wider subregion.
Conclusions
This study demonstrates widespread IgG reactivity to RVF, CCHF and hantaviruses in Senegal, confirming their endemic circulation and under-recognized public-health relevance. High RVF and CCHF seroprevalence were observed in Matam and Thiès, particularly among individuals in frequent contact with livestock and animal products. Elevated RVF rates in Matam likely reflect seasonal pastoral movements, whereas higher CCHF exposure in Thiès may relate to tick-rich environments such as the Bandia Reserve. Infection risk was shaped by gender, age, occupation and behaviors such as the consumption of raw milk. Men, older adults, and those engaged in herding or slaughter activities showed greater exposure, reflecting cumulative and occupational risks at the human–animal interface. Evidence of hantavirus antibodies further suggests low-level but persistent circulation maintained by rodent reservoirs in peri-urban and sylvatic habitats. Our results suggest that routine surveillance is missing the vast majority of infections. These viruses circulate endemically within exposed populations, often in an asymptomatic or subclinical state, or manifesting with mild symptoms. This under-detection by the current monitoring system poses a significant challenge to the implementation of effective control strategies in endemic regions. These findings highlight the need to reinforce One Health surveillance by integrating human, animal, and entomological data with behavioral risk monitoring. Strengthened diagnostics, community-based surveillance, and predictive modeling are essential to anticipate and mitigate future zoonotic outbreaks in Senegal and the wider region.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prasad N Murdoch DR Reyburn H Crump JA. Etiology of severe febrile illness in low- and middle-income countries: a systematic review. P Lo S ONE. (2015) 10:e 0127962. doi: 10.1371/journal.pone.012796226126200 PMC 4488327 · doi ↗ · pubmed ↗
- 2Chauhan RP Dessie ZG Noreddin A El Zowalaty ME. Systematic review of important viral diseases in africa in light of the ‘one health' concept. Pathogens. (2020) 9:301. doi: 10.3390/pathogens 904030132325980 PMC 7238228 · doi ↗ · pubmed ↗
- 3Biteye B Fall AG Seck MT Ciss M Diop M Gimonneau G. Host-feeding patterns of Aedes (Aedimorphus) vexans arabiensis, a Rift Valley Fever virus vector in the Ferlo pastoral ecosystem of Senegal. P Lo S ONE. (2019) 14:e 0215194. doi: 10.1371/journal.pone.021519431584948 PMC 6777780 · doi ↗ · pubmed ↗
- 4Diallo M Lochouarn L Ba K Sall AA Mondo M Girault L . First isolation of the Rift Valley fever virus from Culex poicilipes (Diptera: Culicidae) in nature. Am J Trop Med Hyg. (2000) 62:702–4. doi: 10.4269/ajtmh.2000.62.70211304058 · doi ↗ · pubmed ↗
- 5Fontenille D Traore-Lamizana M Diallo M Thonnon J Digoutte JP Zeller HG. New vectors of Rift Valley Fever in West Africa. Emerg Infect Dis J - CDC. (1998) 4:289–93. doi: 10.3201/eid 0402.9802189621201 PMC 2640145 · doi ↗ · pubmed ↗
- 6ErgönülÖ. Crimean-Congo haemorrhagic fever. Lancet Infect Dis. (2006) 6:203–14. doi: 10.1016/S 1473-3099(06)70435-216554245 PMC 7185836 · doi ↗ · pubmed ↗
- 7Subudhi S Dakouo M Sloan A Stein DR Grolla A Jones S . Seroprevalence of Rift Valley Fever virus antibodies in cattle in Mali, 2005–2014. Am J Trop Med Hyg. (2018) 98:872–4. doi: 10.4269/ajtmh.17-084129363462 PMC 5930922 · doi ↗ · pubmed ↗
- 8Spengler JR BergeronÉ Rollin PE. Seroepidemiological studies of Crimean-Congo hemorrhagic fever virus in domestic and wild animals. P Lo S Neglected Tropical Diseases. (2016) 10:e 0004210. doi: 10.1371/journal.pntd.000421026741652 PMC 4704823 · doi ↗ · pubmed ↗