Construction of a Bayesian network-based risk prediction model for hepatocellular carcinoma in cirrhotic patients
Ni Ma, Jingwei Song, Yuqing Yang

TL;DR
This study builds a Bayesian network model to predict which cirrhosis patients are at higher risk of developing liver cancer, using clinical data and identifying key risk factors.
Contribution
A novel Bayesian network-based risk prediction model combining LASSO regression for cirrhosis progression to hepatocellular carcinoma.
Findings
Female gender is a protective factor against liver cancer progression in cirrhosis patients.
The Bayesian network model outperforms logistic regression in predicting HCC progression.
Elevated total cholesterol and reduced antithrombin III activity are significant risk factors for HCC progression.
Abstract
To investigate clinical data of hospitalised cirrhosis patients, identify risk factors for cirrhosis progression to hepatocellular carcinoma, establish a risk prediction model, and provide scientific basis for early identification of high-risk patients. Hospitalised cirrhosis patients treated at Xinjiang Uygur Autonomous Region People’s Hospital between January 2019 and December 2023 were selected. Their inpatient examination records were retrieved, including medical record summaries alongside results for coagulation function, complete blood count, liver function tests, urinalysis, renal function tests, tumour markers, comprehensive hepatitis panel, comprehensive thyroid function panel, comprehensive biochemical panel, glucose series, and lipid series. Patients diagnosed with hepatic malignancy during subsequent hospitalisations (excluding the initial admission) formed the cancer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
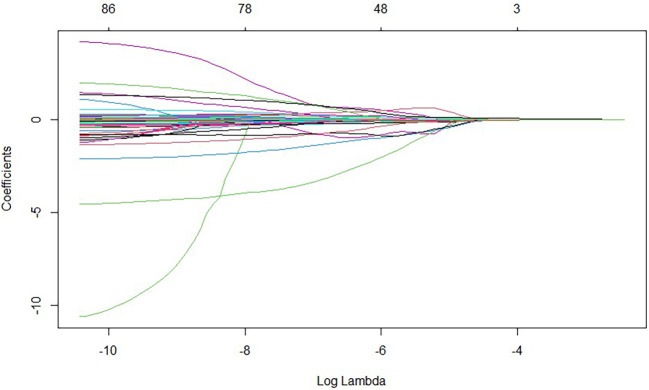 Figure 1
Figure 1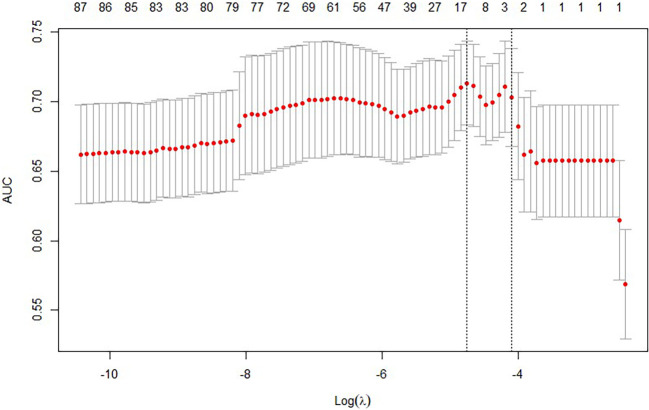 Figure 2
Figure 2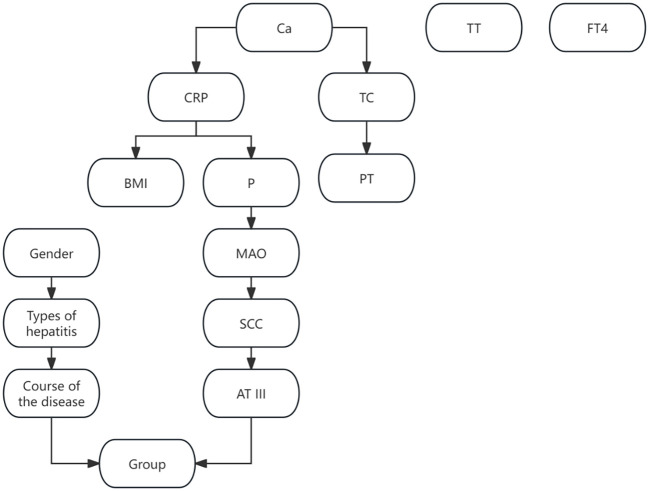 Figure 3
Figure 3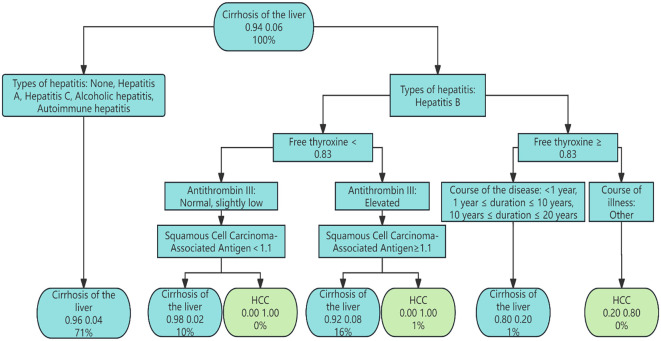 Figure 4
Figure 4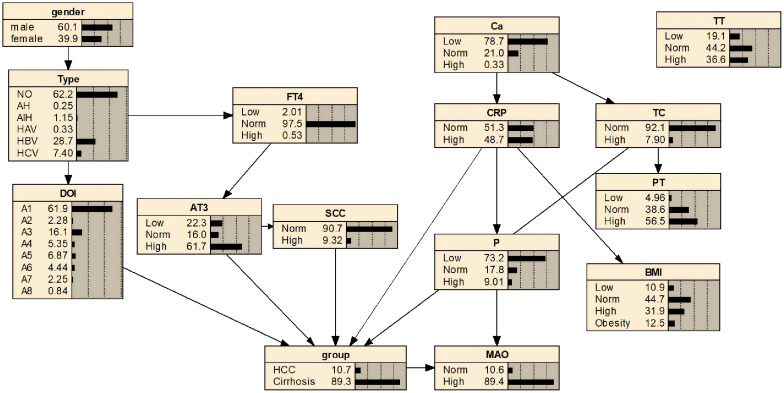 Figure 5
Figure 5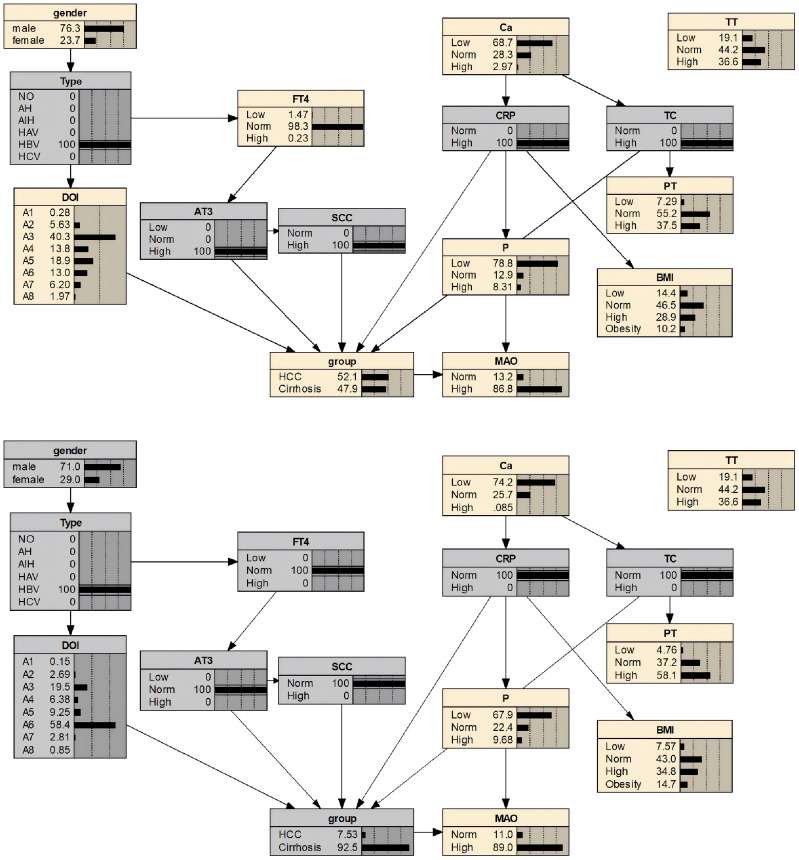 Figure 6
Figure 6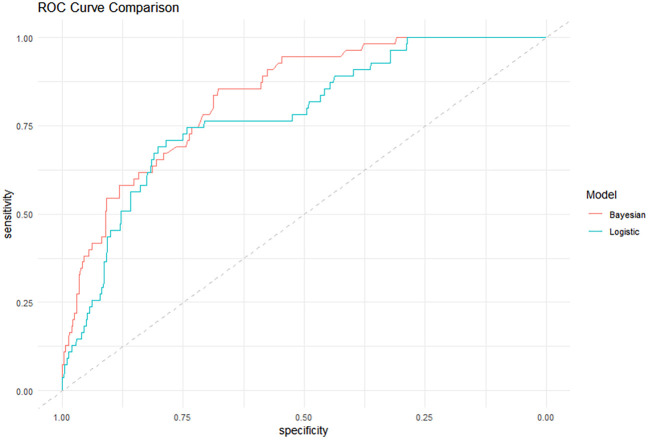 Figure 7
Figure 7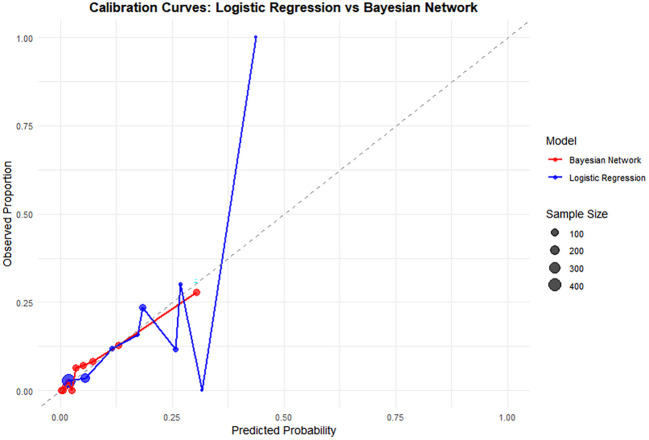 Figure 8
Figure 8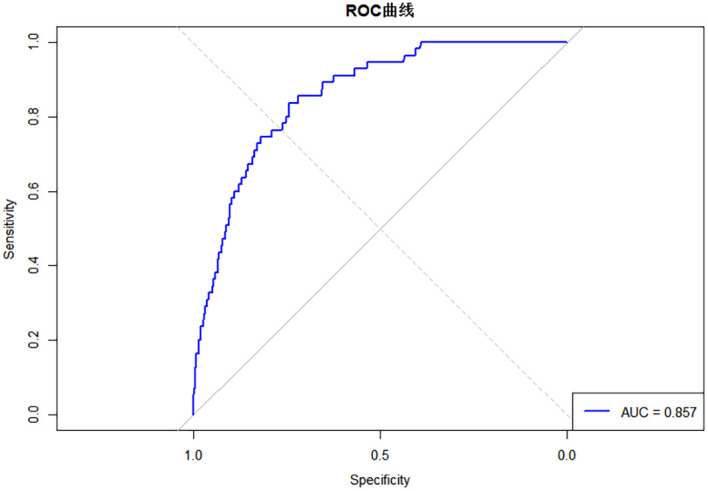 Figure 9
Figure 9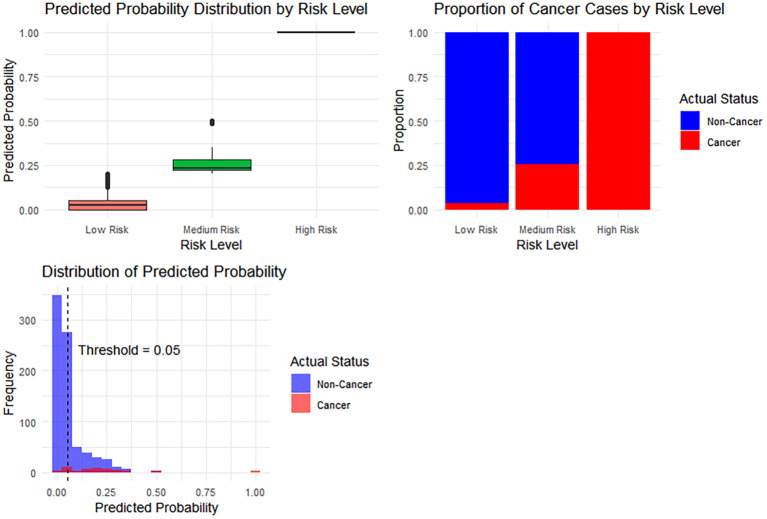 Figure 10
Figure 10| Variable | Levels | Cirrhosis of the liver N(%) | Malignant liver tumour N(%) |
|
|---|---|---|---|---|
| Gender | male | 664 (91.7) | 60 (8.3) | <0.001 |
| female | 464 (96.7) | 16 (3.3) | ||
| Types of hepatitis | Normal | 728 (96.6) | 26 (3.4) | <0.001 |
| Hepatitis A | 2 (100) | 0 (0) | ||
| Hepatitis B | 301 (86.7) | 46 (13.3) | ||
| Hepatitis C | 84 (95.5) | 4 (4.5) | ||
| Alcoholic hepatitis | 1 (100) | 0 (0) | ||
| Autoimmune hepatitis | 12 (100) | 0 (0) | ||
| Course of the disease | 0 | 728 (96.6) | 26 (3.4) | <0.001 |
| <1 year | 23 (95.8) | 1 (4.2) | ||
| ≥1 year and <10 years | 177 (88.5) | 23 (11.5) | ||
| ≥10 years and <20 years | 57 (90.5) | 6 (9.5) | ||
| ≥20 years and <30 years | 71 (86.6) | 11 (13.4) | ||
| ≥30 years and <40 years | 44 86.3) | 7 (13.7) | ||
| ≥40 years and <50 years | 23 (95.8) | 1 (4.2) | ||
| ≥50 years | 5 (83.3) | 1 (16.7) | ||
| BMI | Normal | 495 (91.7) | 45 (8.3) | 0.037 |
| underweight | 126 (96.9) | 4 (3.1) | ||
| overweight | 363 (94.3) | 22 (5.7) | ||
| obesity | 144 (96.6) | 5 (3.4) | ||
| Total cholesterol | Normal | 1046 (94.1) | 65 (5.9) | 0.040 |
| slightly elevated | 82 (88.2) | 11 (11.8) | ||
| Antithrombin III | Normal | 187 (97.9) | 4 (2.1) | <0.001 |
| below average | 682 (91.4) | 64 (8.6) | ||
| slightly elevated | 259 (97.0) | 8 (3.0) |
| Variable |
|
|
|
|
| |
|---|---|---|---|---|---|---|
| lower limit | upper limit | |||||
| Gender(female) | -0.632 | 4.510 | 0.034 | 0.532 | 0.297 | 0.952 |
| Types of hepatitis | 29.889 | 0.000 | ||||
| Hepatitis A | -17.757 | 0.000 | 0.999 | 0.000 | 0.000 | 0.000 |
| Hepatitis B | 1.406 | 28.891 | 0.000 | 4.080 | 2.443 | 6.814 |
| Hepatitis C | 0.304 | 0.300 | 0.584 | 1.355 | 0.457 | 4.021 |
| Alcoholic hepatitis | -18.326 | 0.000 | 1.000 | 0.000 | 0.000 | 0.000 |
| Autoimmune hepatitis | -17.507 | 0.000 | 0.999 | 0.000 | 0.000 | 0.000 |
| Elevated total cholesterol | 0.836 | 5.289 | 0.021 | 2.308 | 1.132 | 4.707 |
| Antithrombin III | 15.422 | 0.000 | ||||
| Slightly elevated | -0.489 | 0.608 | 0.436 | 0.613 | 0.179 | 2.098 |
| Below average | 1.093 | 7.859 | 0.005 | 2.982 | 1.389 | 6.402 |
| Constant | -3.338 | 34.537 | 0.000 | 0.035 | ||
| Variable | Coefficient |
|
|---|---|---|
| Prothrombin time(PT) | -3.66E-02 | 0.9640603 |
| Thrombin time(TT) | 7.75E-02 | 1.080562 |
| Monoamine oxidase(MAO) | -8.12E-02 | 0.921985 |
| Alkaline phosphatase(ALP) | 9.77E-05 | 1.0000977 |
| Platelet distribution width(PDW) | -1.06E-03 | 0.9989404 |
| C-reactive protein(CRP) | 3.26E-03 | 1.0032662 |
| Creatine kinase isoenzymes(CK-MB) | 2.31E-03 | 1.0023101 |
| Ca | 1.80E-01 | 1.1966451 |
| P | -2.21E-01 | 0.8014812 |
| Total cholesterol(TC) | 3.42E-02 | 1.0347541 |
| Alpha-fetoprotein(AFP) | 2.79E-05 | 1.0000279 |
| Free thyroxine(FT4) | -1.71E-01 | 0.8427542 |
| Squamous Cell Carcinoma-Associated Antigen(SCC) | -6.85E-02 | 0.9337824 |
| Antithrombin III(AT III) | 1.09E-01 | 1.1155666 |
| Model | Brier_Score | AUC | Accuracy | C-index(95%CI) | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| Bayesian Network | 0.052 | 0.857 | 0.940 | 0.833(0.784-0.882) | 0.836 | 0.744 |
| Logistic Regression | 0.056 | 0.780 | 0.934 | 0.785(0.726-0.843) | 0.727 | 0.766 |
| k-fold | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Accuracy | 0.901 | 0.951 | 0.911 | 0.917 | 0.868 | 0.950 | 0.975 | 0.938 | 0.915 | 0.964 | 0.929 |
| Risk stratum | Sample size | Risk proportion |
|---|---|---|
| Low Risk | 318 | 0.036 |
| Intermediate risk | 42 | 0.253 |
| High Risk | 1 | 1.000 |
- —Natural Science Foundation of Xinjiang Uygur Autonomous Region10.13039/100009110
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Liver Disease and Transplantation · Liver Disease Diagnosis and Treatment
Introduction
1
Liver cancer, specifically hepatocellular carcinoma (HCC), is a malignant tumour originating from liver cells, primarily comprising two types: hepatocellular carcinoma and cholangiocarcinoma. It ranks among the most prevalent malignant tumours globally, exhibiting high incidence and mortality rates. According to 2020 estimates, hepatocellular carcinoma ranks sixth among the most common malignant tumours worldwide, third among causes of malignant tumour mortality (1), and second among causes of premature cancer death (2). Hepatocellular carcinoma presents insidiously, with a poor prognosis in advanced stages, a median survival of less than one year, and a five-year survival rate of merely 7% (3, 4). Substantial evidence indicates that cirrhosis constitutes the primary pathological basis for the development of hepatocellular carcinoma (HCC), with over 80% of HCC cases originating from this population (5). Consequently, it has become an international consensus to identify cirrhosis patients as the core target group for primary prevention and early monitoring of HCC. Current clinical practice guidelines recommend regular ultrasound screening for all patients with liver cirrhosis. However, significant heterogeneity exists within this cohort, and the risk of progression to hepatocellular carcinoma (HCC) is not uniform. Therefore, precise risk stratification of cirrhosis patients to identify a truly “extremely high-risk” subgroup and develop individualised enhanced monitoring protocols for them is crucial for optimising HCC prevention and control systems and improving patient outcomes. This study aims to identify risk factors for the progression of liver cirrhosis to hepatocellular carcinoma by analysing diagnostic data from hospitalised cirrhosis patients, and to establish a predictive risk model. This endeavour seeks to provide scientific evidence for the early identification of high-risk individuals for hepatocellular carcinoma among cirrhosis patients.
Research content and methods
2
Research subjects
2.1
Patients hospitalised for liver cirrhosis at the Xinjiang Uygur Autonomous Region People’s Hospital between January 2019 and December 2023 were selected. Exclusion criteria were: ① Patients hospitalised for less than 24 hours; ② Patients with newly diagnosed malignant liver tumours during their first admission; ③ Patients with secondary liver cancer; ④ Patients with concomitant other tumours.
Research content
2.2
An analysis of the general characteristics and examination results of patients with cirrhosis and those who progressed from cirrhosis to hepatocellular carcinoma was conducted. This identified the factors influencing the development of hepatocellular carcinoma in cirrhosis patients and enabled the construction of a risk prediction model for the progression from cirrhosis to hepatocellular carcinoma.
Research methodology
2.3
The hospital information department retrieved medical records for cirrhosis patients using their hospital admission numbers as identifiers. This included the front pages of medical records and test results for coagulation function, complete blood count, liver function tests, urinalysis, renal function tests, tumour markers, comprehensive hepatitis panel, comprehensive thyroid function panel, comprehensive biochemical panel, glucose series, and lipid series. A total of 97 variables were selected, with incomplete or missing data removed from the records.
Patients with liver cirrhosis who were diagnosed with hepatic malignancy during subsequent hospitalisations (excluding the initial admission) constituted the malignancy group, while those without hepatic malignancy served as the control group. The progression of liver cirrhosis to hepatic malignancy was confirmed through clinical presentation, imaging studies, and pathological diagnosis. This study was approved by the hospital’s ethics committee (KY2024052420).
Diagnostic criteria for malignant liver tumours: Guidelines for the Diagnosis and Treatment of Hepatocellular Carcinoma (2019 Edition) (6).
Diagnostic criteria for cirrhosis: Evidence-based clinical practice guidelines for Liver Cirrhosis (7).
Statistical methods
2.4
Use Excel software to perform preliminary data processing.Univariate analysis and factor analysis were conducted using SPSS 26.0 software. Numerical variables were expressed as mean ± standard deviation, with intergroup comparisons performed using the independent samples t-test. Categorical variables were represented by frequency and proportion, with intergroup comparisons conducted using the chi-square test. Factor analysis employed a binary logistic regression model. The significance level was set at P < 0.05.Handling Missing Values and Outliers: Missing values were detected using the summary function in R. If any missing values were found, the Multiple Imputation method was employed for their imputation. Outliers were detected using boxplots, where values below Q1-1.5 * IQR or above Q3 + 1.5 * IQR were considered outliers. If an outlier resulted from an operational error during data recording, the data were re-verified and corrected. If the outlier was a natural component of the population, the winsorization method was applied to adjust the outlier to the boundary value of the corresponding percentile.Employing the glmnet package within R software for LASSO regression variable selection, cross-validation was utilised to identify the optimal λ. Model λ screening primarily encompasses lambda.min and lambda.1se; this study employed lambda.min to select variables most strongly associated with the outcome.Bayesian network modelling was conducted using the bnleam package within R software. Divide the data into training and test sets in a 7:3 ratio. First, use the training set data with the hc function to train the network, obtaining a preliminary network architecture. The bn.fit_MLE function was then used to learn the network parameters. The cpquery function facilitated Bayesian network inference and the calculation of conditional probability distribution tables. Subsequently, nodes and directed links may be added to the Bayesian network model based on existing research findings and decision tree models, employing the set.arc function for this purpose. Finally, Netica software was used to construct the Bayesian network model. The built-in node inference function of Netica was employed to calculate the probability of outcome changes caused by the cumulative effects of various factors. Additionally, sensitivity analysis was conducted using the “grain”package in R to analyse the probability of the outcome under specific single-factor conditions.Model Evaluation: The “ggplot2” package in R was used to plot calibration curves. By comparing the Bayesian network model with the logistic regression model, the predictive performance of the Bayesian network model was assessed through a comprehensive comparison of several evaluation metrics, including Brier Score, AUC, Accuracy, C-index (95% CI), Sensitivity, and Specificity. k−fold cross-validation was employed to evaluate the accuracy rate of the model.Model Prediction Threshold and Risk Stratification Strategy: The trained Bayesian network model was applied to the test set to compute risk probabilities. After evaluating the model’s performance, the ROC curve and AUC were calculated. The optimal threshold was determined from the ROC curve by maximizing the Youden index. Based on the predicted probabilities and actual classifications, two thresholds were defined: Threshold 1 (the upper limit for low risk—the threshold at which specificity reaches 90%) and Threshold 2 (the lower limit for high risk—the threshold at which sensitivity reaches 90%). The curve was then segmented into three parts corresponding to low, intermediate, and high risk. Finally, the relationships between risk strata and predicted probabilities, risk strata and actual cancer status, as well as a histogram of predicted probability distribution, were plotted.
Result
3
General overview
3.1
A total of 1,204 individuals were included in this study, comprising 1,128 patients with liver cirrhosis, with no missing values identified. Among them, 76 patients with liver cirrhosis developed hepatic malignancy. There were 724 males and 480 females. The proportion of males progressing to liver malignancy (8.3%) was higher than that of females (3.3%). Patients with cirrhosis and hepatitis B showed the highest incidence of liver malignancy progression (13.3%). Patients with a disease duration of ≥50 years had a higher incidence of liver malignancy progression than those with other durations. Patients with normal BMI exhibited the highest incidence of liver malignancy (8.3%); cirrhosis patients with elevated total cholesterol levels demonstrated a higher incidence of liver malignancy (11.8%); cirrhosis patients with reduced antithrombin III activity showed a higher incidence of liver malignancy (8.6%) (P < 0.05), as shown in Table 1.
Risk factor analysis
3.2
The results of the multivariable logistic regression model indicate that being female is a protective factor against the progression of liver cirrhosis to hepatocellular carcinoma (OR = 0.532, OR 95% CI = 0.297-0.952); Hepatitis B, elevated total cholesterol, and reduced antithrombin III activity were identified as risk factors for the progression of cirrhosis to malignant liver tumours (OR = 4.080, OR 95% CI = 2.443–6.814, OR = 2.308, OR 95% CI = 1.132–4.707, OR = 2.982, OR 95% CI = 1.389–6.402) (P < 0.05), as shown in Table 2.
LASSO regression model
3.3
The 97 collected laboratory test results were incorporated into the LASSO model. After 100 rounds of cross-validation, the minimum average error lambda value was determined as lambda.min=0.008638309. This lambda value was then applied to the LASSO model, ultimately identifying 14 variables most significantly associated with the progression from liver cirrhosis to malignant liver tumours. These variables are: monoamine oxidase, alkaline phosphatase, platelet distribution width, C-reactive protein, creatine kinase isoenzymes, total calcium, phosphorus, total cholesterol, alpha-fetoprotein, free thyroxine, squamous cell carcinoma-associated antigen, and antithrombin III activity. See Figures 1, 2, and Table 3.
Variable selection in the LASSO-based predictive model 1.
Variable selection in the LASSO-based predictive model 2.
Construction of Bayesian network models
3.4
Based on variables selected via LASSO regression and combined with risk factor analysis results, an initial Bayesian network disease prediction model comprising 15 nodes and 12 directed edges was constructed. The conditional probabilities for each node are shown in Figure 3. By constructing a decision tree model, relationships among some variables were identified (see Figure 4). Integrating this with the Bayesian network model from Figure 3, the set.arc function was employed to add edges, yielding a Bayesian network model comprising 15 nodes and 17 directed edges (see Figure 5). Figure 5 demonstrates that variables including gender, hepatitis type, disease duration, free thyroxine, antithrombin III activity, squamous cell carcinoma-associated antigen, C-reactive protein, monoamine oxidase, and total calcium establish connections with the progression of liver cirrhosis to malignant liver tumours through complex network relationships. Disease duration, antithrombin III activity, squamous cell carcinoma-associated antigen, C-reactive protein, and total cholesterol are directly associated with the occurrence of hepatic malignancy; gender, free thyroxine, hepatitis type, and total calcium exert an indirect influence on the development of hepatic malignancy.
Bayesian network model.
Decision tree model.
Bayesian network risk prediction model for hepatocellular carcinoma in patients with liver cirrhosis.
Model inference
3.5
Sensitivity analysis revealed the probability of progression from liver cirrhosis to hepatocellular carcinoma under specific conditions: when AT3 levels were normal, the probability was 0.0749 (7.5%); when AT3 was low, it was 0.0709 (7.1%); and when AT3 was high, the probability increased to 0.0850 (8.5%). Regarding TC levels, the probability was 0.0763 (7.6%) when TC was normal, but rose significantly to 0.1309 (13.1%) when TC was elevated. The Netica node cumulative inference results showed that for a cirrhosis patient with hepatitis B, whose antithrombin III activity was at a low level and squamous cell carcinoma antigen, total cholesterol, and C-reactive protein were at high levels, the probability of progressing to hepatic malignancy was 52.1%. However, if antithrombin III activity, squamous cell carcinoma antigen, total cholesterol, and C-reactive protein were maintained at normal levels, the probability of developing hepatic malignancy would decrease to 7.5%, as shown in Figure 6.
Bayesian network prediction model inference for hepatocellular carcinoma development in patients with liver cirrhosis.
Model evaluation
3.6
The results showed that the performance of the Bayesian network model (AUC = 0.857, Brier Score = 0.052, Accuracy = 0.940, C-index (95% CI)=0.833(0.784–0.882), Sensitivity = 0.836, Specificity = 0.744) was superior to that of the logistic regression model (AUC = 0.780, Brier Score = 0.056, Accuracy = 0.934, C-index (95% CI) = 0.785 (0.726–0.843), Sensitivity = 0.727, Specificity = 0.766), as detailed in Table 4 and Figure 7. The calibration curve results indicated that the predicted points of the Bayesian network model were evenly distributed around the diagonal line, suggesting good predictive performance (see Figure 8). Ten-fold cross-validation was performed, and the results showed that in nine out of the ten validation runs, the accuracy exceeded 0.9, with an average accuracy of 0.93 (see Table 5).
Comparison of the area under the ROC curve between the two models.
Comparison of the calibration curves between the two models.
Model prediction threshold and risk stratification strategy for the Bayesian network model
3.7
Based on the predicted values, the ROC curve of the Bayesian network model was established (see Figure 9). The area under the curve (AUC) was 0.857. After balancing sensitivity and specificity, the optimal threshold was determined by maximizing the Youden index (0.052). A predicted probability > 0.052 indicates progression from liver cirrhosis to hepatic malignancy. Based on the ROC curve, threshold 1 was set at 0.2 and threshold 2 at 0.8 to establish a risk stratification system: low risk (predicted probability < 0.2), intermediate risk (0.2 ≤ predicted probability ≤ 0.8), and high risk (predicted probability > 0.8). Accordingly, 318 patients were classified as low risk, 42 as intermediate risk, and 1 as high risk (see Table 6). Monitoring frequency recommendations are as follows: low-risk patients: annual routine check-ups; intermediate-risk patients: regular monitoring every 6 months; high-risk patients: close monitoring every 3 months, with consideration for further diagnostic procedures. The relationships between risk strata and predicted probabilities, risk strata and actual cancer status, and the predicted probability distribution are shown in Figure 10.
ROC curve of the Bayesian network model.
The relationship between risk strata and predicted probabilities, the relationship between risk strata and actual cancer status, and the predicted probability distribution.
Discussion
4
Hepatocellular carcinoma exhibits high mortality rates and poor prognosis, constituting a major disease affecting human health and quality of life. In China, over 80% of hepatocellular carcinoma cases develop from cirrhosis. Consequently, close monitoring of cirrhosis patients to prevent progression to hepatocellular carcinoma is paramount. This study enrolled 1,204 cirrhosis patients, among whom 76 progressed to hepatocellular carcinoma. Male cirrhosis patients exhibited a higher probability of developing hepatocellular carcinoma than female patients, a finding consistent with the gender incidence ratio observed in China, South Korea, and Japan (8). This may be related to the fact that men engage in unhealthy lifestyle habits such as smoking and excessive alcohol consumption more frequently than women (9, 10). A single-centre cohort study in the United States indicates that men are diagnosed with liver cancer at a later stage than women, presenting with larger tumours and a greater number of lesions. This may be attributed to men undergoing routine screening for liver cancer less frequently. Consequently, it is recommended that male patients with hepatitis, cirrhosis, and even those in good health undergo regular health check-ups to facilitate early detection and diagnosis of liver cancer. Prompt treatment is essential to enhance therapeutic outcomes. At the same time, men should place greater emphasis on lifestyle and dietary habits, refraining from smoking and excessive drinking, adopting a healthy diet, engaging in regular exercise, and enhancing their physical fitness.
This study found that patients with cirrhosis complicated by hepatitis B virus infection exhibited a higher risk of developing hepatocellular carcinoma compared to other patients. Furthermore, multivariate analysis revealed that the presence of hepatitis B virus infection constitutes a risk factor for the progression of cirrhosis to hepatocellular carcinoma. In China, the incidence of hepatitis B-related hepatocellular carcinoma remains persistently high, with studies predicting an increasing trend in this incidence over the forthcoming period (11, 12). Since the formulation of the Guidelines for the Prevention and Treatment of Chronic Hepatitis B in 2005, the prevalence of hepatitis B in China has shown a marked downward trend (13). Nevertheless, China remains one of the countries bearing the heaviest global burden of hepatitis B virus infection (14), posing an extremely serious threat to the lives and property of its people. Consequently, the prevention and control of hepatitis B cannot be delayed. Regular testing for hepatitis B antibodies and timely vaccination with the hepatitis B vaccine are effective methods for preventing infection with the hepatitis B virus. Rejecting drugs, avoiding the sharing of syringes, and maintaining healthy lifestyle and dietary habits to boost immunity can all effectively prevent hepatitis B infection.
Among hepatitis patients, the longer the duration of illness, the greater the likelihood of developing hepatocellular carcinoma. This finding is consistent with the results of a Chinese age-time cohort study on hepatocellular carcinoma (10). Rocio I.R. Macias et al. (15) propose that with increasing age and disease duration, factors such as genomic instability, telomere attrition, epigenetic alterations, impaired protein homeostasis, and mitochondrial dysfunction collectively promote the development of hepatocellular carcinoma. The liver possesses remarkable regenerative potential; however, over time, the accumulation of risk factors can lead to irreversible damage to liver function. Consequently, early detection, diagnosis, and treatment are essential measures for reducing the incidence of liver cancer. National and societal bodies should establish comprehensive liver cancer surveillance systems to promptly identify high-risk populations. Communities and hospitals must undertake public education responsibilities, providing health awareness campaigns to inform the public about the dangers of liver cancer and the necessity of timely diagnosis and treatment.
The relationship between serum cholesterol and the risk of hepatocellular carcinoma remains controversial. Findings from studies by Cai X et al. indicate a negative correlation between serum cholesterol levels and the incidence of hepatocellular carcinoma (16, 17), whereas other research suggests that elevated cholesterol levels may contribute to the development of this malignancy (18–20). Takuma Tsuchida et al. (21) observed in mouse studies that a high-cholesterol diet readily induces non-alcoholic fatty liver disease, subsequently leading to hepatocellular carcinoma. Further research indicates that dietary cholesterol drives hepatocellular carcinoma development by inducing alterations in the gut microbiota and metabolites of mice (19). This study found that patients with elevated cholesterol levels also exhibited a higher incidence of liver cancer. Analysis of influencing factors similarly indicated that elevated cholesterol constitutes a risk factor for the progression of cirrhosis to liver cancer, potentially linked to these patients’ high-cholesterol diets. Patients with cirrhosis require adequate nutrition to control disease progression, yet excessive cholesterol intake proves counterproductive. Given that high-fat, high-cholesterol foods constitute a significant proportion of the Xinjiang diet, promoting balanced nutrition and increasing physical activity are essential strategies for preventing the occurrence of liver cancer.
Antithrombin III, synthesised by the liver, vascular endothelial cells and megakaryocytes, is a protease inhibitor in plasma with anticoagulant properties. It can inhibit hepatitis viruses and reduce the likelihood of developing cirrhosis and hepatocellular carcinoma by modulating multiple host cell signalling factors associated with these conditions (22). It may also regulate the development of hepatocellular carcinoma by inhibiting thrombin (22), and can prevent the metastasis of cancer cells (23). This study has identified reduced antithrombin III activity as a risk factor for the progression of liver cirrhosis to hepatocellular carcinoma. This may be attributed to the more severe hepatic damage in cirrhotic patients, which diminishes their capacity to produce antithrombin III. Consequently, plasma antithrombin III levels decline, impairing the body’s ability to inhibit hepatocellular carcinoma development. Consequently, close monitoring of coagulation function is essential in daily life for cirrhosis patients. Regular medical examinations and adherence to prescribed medication are crucial for restoring antithrombin III activity. Concurrently, appropriate supplementation with iron- and folate-rich foods—such as animal blood, liver, and egg yolks—is advised to correct anaemia.
Bayesian networks can illustrate the relationship between various influencing factors and the progression of cirrhosis to hepatocellular carcinoma. The model indicates that, apart from phosphorus levels, BMI, thrombin time, and prothrombin time, other factors are associated with the development of hepatocellular carcinoma through direct or indirect pathways. Gender influences the type and duration of hepatitis, thereby contributing to HCC development. A 2019 study on the demographic characteristics of hepatitis B virus infection in China indicated that males are more susceptible to viral hepatitis than females (24). Patients with hepatitis B virus infection typically experience more severe disease and greater treatment challenges; the likelihood of developing HCC increases with disease progression.
This study further revealed that hepatitis type can influence free thyroxine levels, thereby affecting antithrombin III activity and ultimately contributing to hepatocellular carcinoma. Research indicates that nearly half of patients with viral hepatitis undergoing interferon therapy develop thyroid disorders, presenting as hypothyroidism (25). Prolonged hypothyroidism increases the risk of hepatocellular carcinoma (26), potentially through hypothyroidism-induced coagulation disorders leading to haemorrhage (27).
Squamous cell carcinoma antigen is a serine protease inhibitor present in normal squamous epithelium. It correlates with the invasion, metastasis, recurrence, and prognosis of squamous cell malignancies, serving as a crucial tumour marker reflecting the biological characteristics of squamous cell carcinoma. Research indicates elevated SCC-related antigen levels in the serum of hepatocellular carcinoma patients, whereas non-hepatocellular carcinoma patients exhibit lower serum SCC-related antigen concentrations (28). The Bayesian network model indicates a pathway from antithrombin III to SCC-A. However, no direct evidence currently exists demonstrating that antithrombin III activity directly influences SCC-A. This discrepancy may explain the elevated SCC-A levels observed in patients with abnormal antithrombin III activity in the present study.
Research indicates (29) that alterations in calcium ion concentration may influence the production and secretion of C-reactive protein. Under normal circumstances, hypocalcaemia (low blood calcium levels) may be associated with elevated C-reactive protein levels. This occurs because hypocalcaemia can stimulate the release of certain cytokines, thereby promoting C-reactive protein production. C-reactive protein is a non-specific inflammatory marker serving as an indicator of sensitivity and specificity in predicting tumour development (30). Existing research has identified an association between C-reactive protein and the occurrence of hepatocellular carcinoma, with higher C-reactive protein levels correlating with increased risk of liver cancer (31, 32). This aligns with the pathway demonstrated in this study’s model, wherein serum total calcium influences C-reactive protein, which in turn affects hepatocellular carcinoma development.
This study examined 1,204 patients with liver cirrhosis admitted to our hospital between 2019 and 2023, identifying 76 cases where cirrhosis progressed to hepatocellular carcinoma. Multivariate analysis revealed that hepatitis B infection, elevated total cholesterol levels, and reduced antithrombin III activity constitute risk factors for the development of malignant liver tumours in cirrhotic patients. Using the LASSO regression model for variable selection, fourteen variables most significantly associated with the progression from cirrhosis to malignant liver tumours were identified. These selected variables were incorporated into a Bayesian network. Combining literature evidence and decision tree model results, a risk prediction model for the progression from cirrhosis to hepatocellular carcinoma was constructed. In summary, gender, hepatitis type, disease duration, total calcium, C-reactive protein, total cholesterol, antithrombin III activity, free thyroxine, and carcinoembryonic antigen are closely associated with the progression of liver cirrhosis to hepatocellular carcinoma. This study has certain limitations. Firstly, the data utilised in this investigation was sourced from a single centre, namely the Xinjiang Uygur Autonomous Region People’s Hospital. Consequently, the distribution of study subjects may lack representativeness. Future research should involve collaboration with multiple hospitals across the region to enhance the representativeness of the study population. Secondly, all variables included in this study were extracted from patients’ hospital admission records and inpatient examination results, without considering variables such as lifestyle habits or dietary patterns. This may introduce bias into the model results. Questionnaire surveys or similar methods should be incorporated to broaden the scope of variables covered. Finally, the progression from cirrhosis to hepatocellular carcinoma is a protracted process. This study’s five-year observation period yielded a relatively small number of patients who developed hepatocellular carcinoma, potentially reducing the model’s accuracy. Consequently, subsequent research should combine retrospective and prospective studies to extend the observation period and minimise research error.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 2Rumgay H Arnold M Ferlay J Lesi O Cabasag CJ Vignat J . Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. (2022) 77:1598–606. doi: 10.1016/j.jhep.2022.08.021, PMID: 36208844 PMC 9670241 · doi ↗ · pubmed ↗
- 3Zhang X Guan L Tian H Zeng Z Chen J Huang D . Risk factors and prevention of viral hepatitis-related hepatocellular carcinoma. Front Oncol. (2021) :686962. doi: 10.3389/fonc.2021.686962, PMID: 34568017 PMC 8458967 · doi ↗ · pubmed ↗
- 4Sayiner M Golabi P Younossi ZM . Disease burden of hepatocellular carcinoma: A global perspective. Dig Dis Sci. (2019) 64:910–7. doi: 10.1007/s 10620-019-05537-2, PMID: 30835028 · doi ↗ · pubmed ↗
- 5Perisetti A Goyal H Yendala R Thandassery RB Giorgakis E . Non-cirrhotic hepatocellular carcinoma in chronic viral hepatitis: Current insights and advancements. World J Gastroenterol. (2021) 27:3466–82. doi: 10.3748/wjg.v 27.i 24.3466, PMID: 34239263 PMC 8240056 · doi ↗ · pubmed ↗
- 6Zhou J Sun H Wang Z Cong W Wang J Zeng M . Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. (2020) 9:682–720. doi: 10.1159/000509424, PMID: 33442540 PMC 7768108 · doi ↗ · pubmed ↗
- 7Yoshiji H Nagoshi S Akahane T Asaoka Y Ueno Y Ogawa K . Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J Gastroenterol. (2021) 56:593–619. doi: 10.1007/s 00535-021-01788-x, PMID: 34231046 PMC 8280040 · doi ↗ · pubmed ↗
- 8Dee EC Laversanne M Bhoo-Pathy N Ho FDV Feliciano EJG Eala MAB . Cancer incidence and mortality estimates in 2022 in southeast Asia: a comparative analysis. Lancet Oncol. 26:516–28. doi: 10.1016/S 1470-2045(25)00017-8, PMID: 40024257 · doi ↗ · pubmed ↗