Acute intestinal obstruction in children: a comparison of laparoscopic treatment and open surgery
Wei Wu, Kezhe Tan, Lulu Zheng, Weijue Xu, Zhibao Lv, Jiangbin Liu, Jun Sun

TL;DR
This study compares laparoscopic and open surgery for treating intestinal blockages in children, finding that laparoscopic surgery leads to faster recovery with no more complications.
Contribution
The study provides evidence that laparoscopic surgery is effective for pediatric acute small bowel obstruction.
Findings
Laparoscopic surgery resulted in shorter hospital stays compared to open surgery.
Laparoscopic surgery led to shorter postoperative fasting periods and lower hospitalization costs.
Complication rates were similar between laparoscopic and open surgery groups.
Abstract
This study aimed to evaluate the clinical efficacy of laparoscopic surgery for acute small bowel obstruction (SBO) in children. The retrospective study included children with acute SBO who were treated at Shanghai Children's Hospital from June 2014 to December 2023. Patients were categorized into one of the following two groups based on the operative approach they underwent: the laparoscopic surgery group and the open surgery group. Perioperative variables, including operative time, fasting duration, hospital stay, and complication rates, were evaluated. The primary outcome was length of hospital stay. Categorical variables were compared using the χ2 or Fisher's exact test, and continuous variables were analyzed using the t-test or Mann–Whitney U test, depending on the data distribution. A P-value < 0.05 was considered statistically significant. In total, 40 patients underwent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
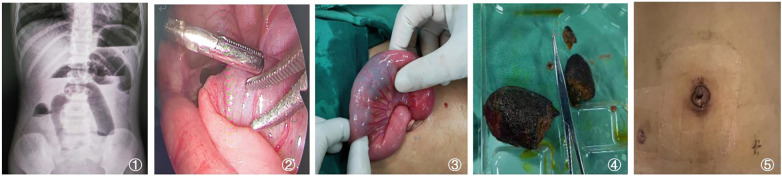 Figure 1
Figure 1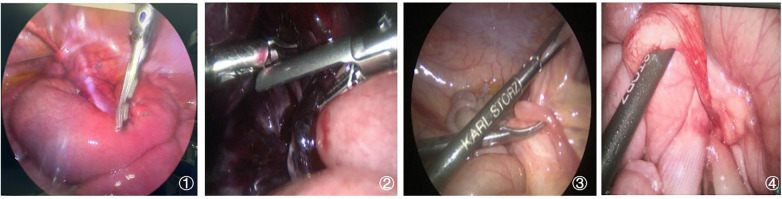 Figure 2
Figure 2| Group (All patients) | Cases ( | Gender ( | Age (months) | Weight (kg) | Symptom-to-surgery interval (h) | History of abdominal surgery ( | ||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Yes | No | |||||
| Laparoscopy | 40 | 20 | 20 | 65.48 ± 37.46 | 18.60 (14.90–20.90) | 48.00 (28.50–99.00) | 11 | 29 |
| Open surgery | 40 | 30 | 10 | 54.30 ± 36.70 | 16.50 (13.20–19.70) | 50.00 (35.50–72.00) | 28 | 12 |
| Statistic | – | 5.333 | 1.349 | −1.839 | −0.197 | 14.459 | ||
| – | 0.021 | 0.181 | 0.066 | 0.844 | 1.430 × 10−4 | |||
| Group (patients excluding conversion) | Cases ( | Length of hospital stay (days) | Hospitalization cost (CNY) | Operative time (min) | Postoperative fasting duration (days) |
|---|---|---|---|---|---|
| Laparoscopic surgery group | 29 | 7.00 (6.50–8.30) | 22,063.50 (18,485.00–24,761.00) | 124.00 ± 26.07 | 4.00 (3.00–5.25) |
| Open surgery group | 40 | 9.50 (9.00–15.70) | 25,433.50 (19,243.00–32,569.00) | 130.47 ± 38.22 | 5.00 (4.00–6.00) |
| Statistic | – | 4.390 | 1.653 | −0.836 | 2.554 |
| – | 1.1 × 10−5 | 0.098 | 0.406 | 0.011 |
| Group (excluding patients with a history of surgery and conversion) | Cases ( | Gender ( | Age (months) | Weight (kg) | Symptom-to-surgery interval (h) | |
|---|---|---|---|---|---|---|
| Male | Female | |||||
| Laparoscopic surgery (excluding converted surgery) | 20 | 10 | 10 | 66.03 ± 39.99 | 21.56 ± 10.48 | 35.00 (26.00–59.25) |
| Open surgery | 12 | 7 | 5 | 53.42 ± 25.69 | 14.97 ± 8.49 | 42.50 (34.13–72.00) |
| Statistic | – | 0.209 | 1.604 | 1.844 | 0.702 | |
| – | 0.647 | 0.337 | 0.075 | 0.501 | ||
| Group (excluding patients with a history of surgery and conversion) | Cases ( | Length of hospital stay (days) | Hospitalization cost (CNY) | Operative time (min) | Postoperative fasting duration (days) |
|---|---|---|---|---|---|
| Laparoscopic group | 20 | 7.00 (6.38–8.00) | 22,025.25 (18,318.75–23,671.25) | 118.68 ± 23.90 | 4.00 (3.00–5.31) |
| Open surgery group | 12 | 13.00 (8.88–16.00) | 25,777.50 (24,781.63–38,690.50) | 132.65 ± 27.89 | 5.50 (4.00–6.00) |
| Statistic | – | 4.256 | 2.453 | −1.505 | 2.095 |
| – | 2 × 10−6 | 0.013 | 0.143 | 0.040 |
| Group (patients who underwent laparoscopy) | Cases ( | Gender ( | Age (months) | Weight (kg) | Symptom-to-surgery interval (h) | |
|---|---|---|---|---|---|---|
| Male | Female | |||||
| Laparoscopic surgery alone | 29 | 17 | 12 | 72.68 ± 40.23 | 21.83 ± 9.74 | 50.00 (41.50–100.75) |
| Laparoscopy converted to open surgery | 11 | 3 | 8 | 46.52 ± 19.90 | 16.13 ± 3.89 | 48.00 (27.00–90.00) |
| Statistic | – | 3.135 | 2.051 | 2.644 | 1.152 | |
| – | 0.155 | 0.047 | 0.012 | 0.254 | ||
| Group (patients who underwent laparoscopy) | Cases ( | Length of hospital stay (days) | Hospitalization cost (CNY) | Operative time (mins) | Postoperative fasting duration (days) |
|---|---|---|---|---|---|
| Laparoscopic surgery alone | 29 | 7.00 (6.50–8.30) | 22,063.50 (18,485.00–24,761.00) | 124.00 ± 26.07 | 4.00 (3.00–5.25) |
| Laparoscopy converted to open surgery Group | 11 | 9.00 (8.00–10.00) | 29,442.00 (26,425.00–39,739.50) | 161.91 ± 42.12 | 4.00 (4.00–5.00) |
| Statistic | – | 2.117 | 2.773 | −3.442 | 0.626 |
| – | 0.035 | 0.005 | 0.001 | 0.550 |
| Group (foreign body ingestion) | Cases | Gender (male/female) | Known foreign body ingestion [ | Weight (kg) | Age (months) | Surgical approach |
|---|---|---|---|---|---|---|
| Laparoscopic surgery group | 10 | 6/4 | 5 (50%) | 17.30 (14.10–21.40) | 66.59 ± 37.47 | Laparoscopic umbilical enterotomy and foreign body removal |
| Open surgery group | 5 | 3/2 | 3 (60%) | 15.50 (14.20–19.70) | 56.32 ± 37.72 | Exploratory laparotomy and enterotomy for foreign body removal |
| Statistical value | – | – | – | −0.367 | 0.499 | – |
| – | 0.713 | 0.573 | 0.768 | 0.626 | – |
| Group (foreign body ingestion) | Cases | Type of foreign body | Hospital stay (days) | Hospitalization cost (CNY) | Surgery time (min) | Postoperative fasting duration (days) |
|---|---|---|---|---|---|---|
| Laparoscopic surgery group | 10 | Superabsorbent polymer, 3; hairball, 3; jujube seed, 2; tannin bezoar, 2. | 5.5 (5–7.5) | 23,198.50 (18,975.00–25,990.25) | 100.07 ± 65.02 | 4.00 (3.75–5.00) |
| Open surgery group | 5 | Superabsorbent polymer, 1; hairball, 1; jujube seed, 1; magnet, 2. | 6 (5–8.6) | 26,980.50 (18,243.00–36,569.00) | 125.10 ± 140.00 | 5.00 (4.25–6.00) |
| Statistical value | – | – | 0.939 | 0.490 | −0.483 | 1.990 |
| – | 0.437 | 0.371 | 0.679 | 0.637 | 0.047 |
| Group (all patients) | Cases ( | Intraoperative complications | ||||
|---|---|---|---|---|---|---|
| Total | Serosal tears (III) | Muscularis injury (III) | Perforation (III) | Open appendiceal stump (III) | ||
| Laparoscopy | 40 | 9 | 4 | 2 | 2 | 1 |
| Open surgery | 40 | 8 | 4 | 3 | 1 | 0 |
| Statistic | – | 0.075 | – | |||
| – | 1.000 | – | ||||
| Group (all patients) | Postoperative complications | ||||||
|---|---|---|---|---|---|---|---|
| Total | Intestinal obstruction (II) | Wound infection (I) | Pneumonia (II) | Bowel leakage (III) | Short bowel syndrome (II) | Chylous ascites (II) | |
| Laparoscopy | 6 | 3 | 2 | 1 | 0 | 0 | 0 |
| Open surgery | 10 | 5 | 1 | 1 | 1 | 1 | 1 |
| Statistic | 1.250 | – | |||||
| 0.402 | 0.455 | ||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Appendicitis Diagnosis and Management · Abdominal Surgery and Complications
Introduction
1
Acute small bowel obstruction (SBO) is a common pediatric surgical emergency that carries meaningful morbidity and non-trivial mortality when diagnosis or treatment is delayed (1, 2). Compared to adults, children exhibit a broader etiological spectrum, faster clinical deterioration, and earlier electrolyte or acid–base disturbances (1–3). Initial management includes nasogastric decompression, fluid resuscitation, and correction of metabolic derangements; urgent surgery is indicated when bowel strangulation is suspected or when conservative treatment fails.
Open surgery has long been the standard approach. With advances in optics, energy devices, and pediatric instruments, laparoscopy has been increasingly adopted for acute SBO and has shown promising short-term recovery profiles in selected populations (4–6). Advocates cite superior visualization, lower wound morbidity, and the potential to reduce adhesion burden over time (7). However, skeptics underscore the risk of iatrogenic bowel injury in a distended and friable small intestine and technical constraints in a limited workspace (8). Therefore, the optimal surgical approach for pediatric acute SBO remains controversial (7–10).
Etiology heavily influences operative decision-making. In children, adhesive SBO (ASBO) after prior laparotomy accounts for a substantial proportion of cases, but non-adhesive causes, such as Meckel diverticulum-related internal hernia (2), congenital or acquired bands (2, 11), volvulus (12), and ingested foreign bodies (13), are also common and may influence the feasibility, conversion rate, and outcomes of laparoscopy. These differences, together with the variable thresholds for failure of non-operative management, complicate comparisons between laparoscopic and open surgery across centers.
Against this background, we conducted a retrospective study of 80 children who underwent operative management for acute SBO at a tertiary pediatric center from June 2014 to December 2023. We analyzed perioperative outcomes between laparoscopic and open approaches, aiming to explore the value of laparoscopic techniques in managing pediatric acute SBO, and further discuss etiology, indications, key intraoperative points, reasons for conversion to open surgery, and prevention and management of complications.
Subjects and methods
2
Study subjects
2.1
This study was approved by the Ethics Committee of Shanghai Children's Hospital (2020R041-E01), and informed consent was obtained from the parents or guardians of all the patients. Inclusion criteria included children (aged 0–18 years) with a confirmed diagnosis of acute SBO who exhibited failure of conservative treatment within 24–48 h or presented with clinical signs suggestive of bowel strangulation or perforation, warranting surgical intervention. Exclusion criteria included cases of acute intussusception, incarcerated hernia, neonatal SBO, inflammatory bowel disease, and tumor-induced acute SBO.
All the patients had complete clinical records, and SBO was diagnosed based on the combination of typical clinical manifestations (crampy abdominal pain, vomiting, abdominal distension, and obstipation) and imaging evidence of SBO (dilated small-bowel loops, multiple air–fluid levels, and absence of colonic gas based on an upright and left lateral X-ray). For infants and young children who could not tolerate an upright and left lateral abdominal X-ray, contrast-enhanced abdominal computed tomography was performed, characterized by dilated small bowel loops with air-fluid levels, a clear transition point between dilated proximal and collapsed distal bowel, and a decompressed colon and rectum. In our center, initial medical treatment comprised nasogastric (NG) decompression, intravenous fluids, electrolyte correction, and antibiotics when SBO was suspected. Failure of medical therapy was defined as persistent obstructive symptoms with continuous NG output and no passage of stool after 24–48 h. Abdominal X-rays were obtained every 6–12 h, and surgery was indicated when three consecutive X-rays showed no improvement. Surgery was also indicated when any signs of ischemia or strangulation appeared, including fever, tachycardia, worsening pain, leukocytosis, or rising lactate.
The surgical approach was chosen based on the preferences of both the surgeon and the patients’ families. Eligibility for laparoscopic surgery required normal cardiopulmonary and coagulation function, stable hemodynamics, no severe abdominal distension (defined as marked tympany, a tense abdominal wall, and radiological evidence of extensive gaseous dilation), no history of abdominal surgery within the past 2 months (to avoid a hostile peritoneal environment) (14), and no prior abdominal malignancy.
Surgical methods
2.2
Laparoscopic surgery
2.2.1
Positioning and trocar placement
2.2.1.1
The patient was placed in a supine position with their waist elevated. The operating table was adjusted as needed during the procedure. The first trocar was inserted using the Hasson technique. For patients with a history of abdominal surgery, the trocar was placed away from previous surgical sites. If dilated bowel loops were palpable, the trocar was placed away from these areas, with the umbilicus serving as the primary choice. Pneumoperitoneum was established, and the abdominal cavity was explored to determine the positions of the other two trocars.
Identifying the site of the obstruction
2.2.1.2
Using atraumatic bowel forceps, the cecum was first located, and the terminal ileum was traced proximally in segments until the transition point between the narrowed and dilated segments was identified.
Releasing the obstruction
2.2.1.3
Adhesions were dissected using an ultrasonic scalpel or Ligasure for bands, and adhesions between bowel loops or between the bowel and abdominal wall were separated with scissors. In cases of Meckel's diverticulum-associated internal hernia, the obstructing band was severed under laparoscopy to release the obstruction. The affected bowel was then extracted through an enlarged umbilical incision for further management.
Traditional open surgery
2.2.2
For infants and children, a transverse abdominal incision was made, whereas adolescents (post-puberty) underwent a midline incision. The small intestine was gently delivered out of the incision, and the transition point between the dilated and narrowed segments was located and released. In cases of necrotic bowel, bowel resection with anastomosis or enterostomy was performed. The abdominal wall was closed in layers.
Observation indicators
2.3
The collected data included general patient information, operative time (from skin incision to final skin closure), postoperative time to regular diet, length of postoperative hospital stay (discharge criteria: regular diet resumed, no complaints of discomfort, regular diet and bowel movements, and no wound abnormalities), incidence of complications, and medical expenses. The criteria for resuming oral intake included the passage of flatus or stool; absence of digestive clinical symptoms such as abdominal pain, vomiting, or distension; recovery of bowel sounds; and tolerance to the gradual reintroduction of fluids.
The length of hospital stay was set as the primary outcome of the study. Other parameters were set as secondary outcomes. Moreover, intraoperative and postoperative complications were assessed using the Clavien–Dindo Classification (15). Briefly, Grade I complications referred to those that did not require pharmacological intervention, such as wound infections. Grade II included complications requiring pharmacological treatment (e.g., antibiotics), including intestinal obstruction, pneumonia, short bowel syndrome, and chylous ascites. Grade III referred to complications requiring surgical intervention, including all intraoperative complications and postoperative bowel leakage.
Statistical analysis
2.4
Statistical analysis was performed using SPSS 17.0 software. Categorical variables were compared using the chi-square test (0 cells with expected count less than 5) or Fisher's exact test (≥ one cell with expected count less than 5). We used the Shapiro–Wilk method to assess the normality of the data. A P-value > 0.05 indicated a normal distribution, while P < 0.05 indicated a non-normal distribution. Normally distributed continuous variables are expressed as mean ± standard deviation (SD) and were analyzed using an independent sample t-test; non-normally distributed variables are presented as median (P25–P75) and were analyzed with the non-parametric Mann–Whitney U test. A P-value < 0.05 was considered statistically significant.
Results
3
General characteristics of the two groups
3.1
In total, 80 children were enrolled (50 boys and 30 girls, with an average age of 59.9 ± 37.8 months, ranging from 1 month to 13 years) and were treated either with laparoscopic surgery (n = 40) or open surgery (n = 40). Among the 80 patients, 39 had a history of abdominal surgery, including bowel resection and anastomosis (n = 17), appendectomy (n = 8), Ladd procedures (n = 8), surgery for Hirschsprung disease (n = 2), and one each for urachal cystectomy, duodenal diaphragm surgery, internal hernia repair after enterostomy, and post-intussusception surgery. The remaining 41 patients had no surgical history. They presented with Meckel's diverticulum-associated internal hernia (n = 9), congenital or acquired band adhesion (n = 6), gastrointestinal foreign body (n = 15; hair, multiple magnets, jujube pits, etc.), volvulus (n = 4), conservative management of appendicitis (n = 3), mesenteric defect hernia (n = 2), small bowel stricture after ischemia-reperfusion injury (n = 1), and idiopathic small bowel stricture (n = 1).
There was a significant skew towards male patients in the open surgery group (P = 0.021). However, no statistically significant differences were observed between the two groups in terms of age (P = 0.181), weight (P = 0.066), or time from symptom onset to surgery (P = 0.844) (Table 1). A history of abdominal surgery was present in 11/40 cases in the laparoscopic group and 28/40 cases in the open surgery group, which was statistically significantly different (P = 1.430 × 10^−4^).
Intraoperative findings in both groups
3.2
In the laparoscopic group (n = 40), five patients were found to have intestinal necrosis or perforation intraoperatively. Moreover, nine underwent intestinal resection and anastomosis or intestinal repair, and 24 underwent adhesiolysis, band excision, or detorsion. Laparoscopic procedures were completed successfully in 29 cases (72.5%), while 11 (27.5%) required conversion to open surgery. The primary reasons for conversion included limited operating space or poor exposure (n = 3), extensive adhesions between bowel loops or with the abdominal wall (n = 4), large areas of small bowel necrosis (n = 1), iatrogenic perforation (n = 1), and multiple magnet-induced perforations (n = 2). Following conversion, five patients underwent adhesiolysis and band excision, five patients required intestinal resection with anastomosis, and one patient underwent adhesiolysis plus intestinal repair. All the patients recovered and were discharged without significant complications.
In the open surgery group (n = 40), intraoperative findings revealed eight cases of intestinal necrosis or perforation. Thirteen cases underwent intestinal resection with anastomosis or intestinal repair, two required intestinal stoma formation, and the remaining cases received adhesiolysis, band excision, detorsion, or reduction of internal hernia.
Comparison of the main outcomes between the two groups
3.3
Length of hospital stay was the primary outcome in this analysis. The laparoscopic group had a significantly shorter hospital stay compared to the open surgery group (median, 7.00 days vs. 9.50 days; P = 1.1 × 10^−5^). Secondary outcomes included postoperative fasting duration, hospitalization cost, and operative time. Postoperative fasting duration was also significantly shorter in the laparoscopic group (median, 4.00 vs. 5.00 days; P = 0.011). Although the median hospitalization cost was lower in the laparoscopic group (22,063.5 vs. 25,433.5 CNY), the difference was not statistically significant (P = 0.098). Operative time was slightly shorter in the laparoscopic group (124.00 ± 26.07 vs. 130.47 ± 38.22 min), but this difference was also not significant (P = 0.406). These results were summarized in Table 2.
Subgroup analysis of the patients without prior abdominal surgery
3.4
To minimize the impact of surgical history on postoperative recovery, a subgroup analysis was conducted among the patients who had no prior abdominal surgery. As shown in Table 3, there were no statistically significant differences in gender (P = 0.647), age (P = 0.337), weight (P = 0.075), or symptom-to-surgery interval (P = 0.501) between the laparoscopic and open surgery groups.
However, as presented in Table 4, the laparoscopic group had a significantly shorter hospital stay (median, 7.00 vs. 13.00 days; P = 2 × 10^−6^), lower hospitalization cost (median, 22,025.25 vs. 25,777.50 CNY; P = 0.013), and shorter postoperative fasting duration (median, 4.00 vs. 5.50 days; P = 0.040) compared to the open surgery group. Operative time did not differ significantly (P = 0.143).
Subgroup analysis of laparoscopic surgery and conversion to open surgery
3.5
To assess the impact of intraoperative conversion on outcomes, we further analyzed the patients in the laparoscopic group based on whether conversion to open surgery was required. As summarized in Table 5, the patients in the conversion group had significantly lower body weight (P = 0.012) and were younger (P = 0.047) than those who underwent laparoscopic surgery alone. Other baseline characteristics were comparable.
As shown in Table 6, the conversion group had a prolonged hospital stay (median, 9.00 vs. 7.00 days; P = 0.035). In addition, the conversion group had significantly higher hospitalization costs (P = 0.005) and operative times (P = 0.001). However, postoperative fasting duration did not differ significantly between the groups (P = 0.550).
Surgical outcomes for gastrointestinal foreign bodies
3.6
Among the 15 children who underwent surgery for gastrointestinal foreign body removal, 10 received laparoscopic-assisted treatment and five underwent open surgery. As shown in Table 7, there were no statistically significant differences between the two groups in baseline characteristics, including sex distribution (P = 0.713), age (P = 0.626), weight (P = 0.768), or history of known foreign body ingestion (P = 0.573).
As shown in Table 8, postoperative fasting duration was significantly shorter in the laparoscopic group than in the open surgery group (median, 4.00 vs. 5.00 days; P = 0.047). Other perioperative outcomes, including length of hospital stay (P = 0.371), hospitalization cost (P = 0.679), and operative time (P = 0.637), did not differ significantly between the groups.
Intraoperative complications
3.7
The overall intraoperative complications are summarized in Table 9. In the laparoscopic group, nine of 40 patients (22.5%) experienced intraoperative complications, including four cases of serosal tears, two cases of muscularis injury (repaired laparoscopically), two cases of intestinal perforation (one repaired directly laparoscopically, one converted to open repair), and one case of open appendiceal stump, managed with a figure-eight suture and ligation at the appendiceal base. In the open surgery group, eight of 40 patients (20.0%) experienced intraoperative complications, including four cases of serosal tears, three cases of muscularis injury (repaired), and one case of intestinal perforation (repaired intraoperatively). The difference in intraoperative complication rates between the laparoscopic and open surgery groups was not statistically significant (P = 1.000).
Postoperative complications
3.8
The overall postoperative complications are summarized in Table 10. In the laparoscopic group, six patients (15.0%) experienced postoperative complications, including three cases of intestinal obstruction (all resolved with conservative management), two cases of umbilical wound infection (healed after wound care), and one case of pulmonary disease (improved with anti-infective and nebulization treatments). In the open surgery group, 10 patients (25.0%) experienced postoperative complications, including five cases of intestinal obstruction (three resolved conservatively and two required reoperation), one case of small bowel leakage (underwent proximal enterostomy on postoperative day 6), one case of short bowel syndrome (improved with gastroenterology treatment), one case of wound infection, one case of chylous ascites, and one case of pneumonia (all improved with conservative management). Although the postoperative complication rate was lower in the laparoscopic group, the difference was not statistically significant (P = 0.402). Similarly, the distribution of specific complications such as intestinal obstruction, wound infection, pneumonia, and bowel leakage did not differ significantly between the groups (P = 0.455); however, we observed a slightly higher Clavien–Dindo grade in the open surgery group.
Discussion
4
Acute SBO is a common pediatric surgical emergency. If conservative treatment fails or bowel strangulation is suspected, emergency surgery is required. The traditional approach is open surgery, which has disadvantages, including significant trauma, slow postoperative recovery, intense pain, and increased risk of recurrent ASBO. As laparoscopic techniques have advanced, their application in acute SBO has increased, yielding favorable outcomes (4, 16). However, the role of laparoscopy in managing acute SBO, especially in pediatric cases, remains controversial (9, 10, 17). Pediatric cases of acute and chronic bowel obstruction due to foreign bodies are not uncommon, with many requiring emergency surgeries. While previous studies have predominantly described open procedures, reports of laparoscopic approaches are becoming more frequent, especially in large pediatric centers, where laparoscopy is gaining traction as a mainstream option for foreign body-induced obstruction (13, 18, 19). We reviewed recent trends in surgical approaches to determine the optimal management strategies for this type of obstruction.
Etiology of pediatric acute SBO
4.1
In adults, acute SBO is primarily caused by ASBO (approximately 75%) and tumors (16, 20). In children, however, the causes are more diverse (Figures 1, 2). Our 5-year review of pediatric acute SBO cases at the center (excluding intussusception, incarcerated hernias, inflammatory bowel disease, and congenital digestive tract abnormalities) identified 80 cases. Among them, 39 cases (48.7%) had a history of abdominal surgery, consistent with previous pediatric reports (17, 21). These 39 children with ASBO mainly developed the condition after bowel resection and anastomosis, appendectomy, or intestinal malrotation. Similar distributions were reported in previous series (8, 17, 21). However, some reports included cases such as fundoplication or gastrostomy tube placement, which were not present in our cohort, likely reflecting differences in patient selection and surgical practices across centers (17). Approximately 50% of the children without ASBO had obstructions that were mainly caused by Meckel's diverticulum hernia, constriction bands, gastrointestinal foreign bodies, volvulus, and appendicitis, and this distribution was also generally consistent with previous studies (8, 21).
(1) Abdominal X-ray showing complete intestinal obstruction. (2) Intraoperative view showing the transition zone between dilated and non-dilated small bowel. (3) Exteriorization of the affected bowel segment containing the gastrointestinal foreign body through the umbilical incision. (4) Identification of foreign body as tannic acid fecalith. (5) Appearance of postoperative abdominal wound at 1 week. SBO, small bowel obstruction. A few panels were adapted from Dong et al. (13), under CC BY 4.0.
(1) Gastrointestinal foreign body (hair) causing an SBO. (2) Postoperative secondary adhesion causing an acute SBO following choledochal cyst surgery. (3) Congenital adhesion leading to an acute SBO. (4) Acute strangulated SBO caused by a hernia in a Meckel's diverticulum. SBO, small bowel obstruction. A few panels were adapted from Dong et al. (13), under CC BY 4.0.
Indications for laparoscopic surgery and key intraoperative points
4.2
Our indications for laparoscopic surgery were largely consistent with those reported in previous studies, which emphasized normal cardiopulmonary function, stable hemodynamics, the absence of severe abdominal distension, no history of abdominal surgery within the previous 2 months, and no history of abdominal malignancy, consistent with previous reports (12, 14, 22).
Placing the first trocar is crucial, and we recommend using the Hasson technique. In children with a previous laparotomy, place the trocar away from scars. If the abdomen palpates with significantly dilated loops, the trocar should be placed away from the dilated bowel. The umbilicus is the first and default site in most cases. If adhesions are extensive, the gap between the abdominal wall and the bowel can be gently separated using the laparoscope, and the second trocar can be placed under direct visualization. We prefer placing the second trocar in the left abdomen and maintaining an inter-port distance of at least 4–5 cm. The approach is consistent with previous routines (23).
After entry, we quickly assess the entire cavity. If the obstruction site is obvious, it is directly managed; otherwise, exploration proceeds from the cecum proximally along the ileum until the transition zone is located. The proximal bowel is often thickened, edematous, and fragile, increasing the risk of perforation. Gentle handling with atraumatic forceps and traction away from the edematous segment are essential. The use of ultrasonic scalpels or Ligasure is recommended for dividing adhesions and sealing small mesenteric vessels. Adhesions between bowel loops or between the bowel and the abdominal wall are often difficult to delineate and require careful identification. Dissecting scissors can be used to separate adhesions, allowing for a combination of sharp and blunt dissection to be performed carefully. Minor bleeding is usually controlled without electrocoagulation, and complete resection of the proximal bowel is unnecessary unless specific issues are found. This detailed technique aligns with previous reports advocating atraumatic dissection with careful instrument handling to minimize bowel injury (24) and stressing the importance of identifying the transition zone early so that extensive proximal bowel resection is often unnecessary (25).
Reasons for conversion to open surgery
4.3
In this study, 11 patients in the laparoscopic group required conversion to open surgery. Three conversions (approximately 27.3%) resulted from limited space or poor exposure, primarily due to dilated bowel loops obscuring the surgical field. Initial attempts at bowel decompression by puncture were ineffective due to the high residual content after the obstruction, which made decompression inadequate. The puncture needle also often slipped out and risked contaminating the abdominal cavity. Proper positioning, sufficient muscle relaxation, and the use of atraumatic bowel forceps, with the cooperation of an anesthesiologist, provided better exposure. Extensive and dense adhesions between bowel loops or between the bowel and the abdominal wall were another common reason for conversion (approximately 72.7%), requiring advanced laparoscopic skill and experience. Our review of all 80 acute SBO surgeries revealed that only nine cases (11.3%) had extensive adhesions, while 51 cases (63.7%) had single-site adhesions, findings consistent with previous reports (23). These data suggest that most pediatric acute SBO cases can be safely managed with standard laparoscopic techniques. With growing surgical proficiency, the conversion rate is expected to decline progressively.
Additionally, foreign body ingestion is a common cause of acute SBO, and the ingestion history is often unclear. Our study demonstrated that foreign bodies were unexpectedly found in seven out of 15 cases (46.7%). Ten children (10/15, 66.7%) underwent laparoscopically assisted surgery with an extended umbilical incision, which allowed successful foreign body removal without conversion to open surgery, a slightly higher laparoscopic rate than previously reported (approximately 60%) (13). The laparoscopic group showed significantly shorter postoperative fasting time and hospital stay compared with the open group, along with shorter operation times and faster recovery. Gastrografin challenge is a useful diagnostic tool for gastrointestinal obstruction. When the cause or site of the obstruction was uncertain, it helped assess both the severity and location. In both laparoscopic and open procedures, most obstructions occurred in the terminal ileum, likely because the foreign body could not pass through the ileocecal valve (26).
Prevention and management of common complications
4.4
The most common intraoperative complications in both laparoscopic and open adhesiolysis procedures are injury to the serosal and muscular layers of the bowel (27). The bowel's course and boundaries are unclear when bowel loops are tightly adherent in SBO. Based on our experience and previous studies (16, 27–32), dissection should begin at relatively clear anatomical landmarks, progressing from more straightforward to more challenging areas. Additionally, it is crucial to separate the adhesions while observing from multiple angles to prevent accidentally stripping the seromuscular layer of the bowel (16, 27, 30). A serosal injury does not require intervention, but any muscular layer injury should be repaired with absorbable sutures (31). If bowel perforation occurs during laparoscopic surgery, healthy bowel around the perforation site should be sutured with absorbable sutures. If the bowel injury is extensive, the perforation can be sealed laparoscopically, with a slight enlargement of the umbilical incision for exteriorization and repair of the injured bowel (32).
The most common postoperative complication is recurrent bowel obstruction, which can usually be relieved with conservative treatment (16). In this study, the incidence of postoperative recurrent bowel obstruction was 7.5% (3/40) in the laparoscopic group, which was slightly lower than that in the open surgery group (12.5%, 5/40), though the difference was not statistically significant. However, relevant studies suggest that the incidence of bowel obstruction after laparoscopic surgery is lower than after open surgery (4, 33).
Limitation
4.5
This study had several limitations. First, the results of the study could have been influenced by different types of biases. For example, there may have been selection bias in the choice between laparoscopic and open surgery, as it was determined by the surgeon's judgment and family preference rather than uniform clinical criteria, which may have influenced the comparability between groups (34). Moreover, there may have been confounding bias, as a significantly higher proportion of patients in the open surgery group had a history of prior abdominal surgery, which may have confounded the observed differences in outcomes and limited the generalizability of the findings (35). Furthermore, other potential confounders, such as variability in surgeon experience (e.g., assessment of abdominal distension), differences in institutional protocols, and the presence of patient comorbidities, may have influenced perioperative outcomes. Second, as a retrospective study, the analysis was based on existing medical records, which may be subject to incomplete or inconsistent documentation, thereby introducing information bias (29). Third, after excluding patients with a history of prior abdominal surgery and those who required conversion to open surgery, the remaining sample size was reduced to n = 32, which may have limited the statistical power of the subgroup analyses. Fourth, this was a single-center study, and institutional practices and surgeon expertise may not be representative of broader clinical settings, thereby limiting the external validity of the results. Finally, long-term follow-up data were not available, precluding evaluation of important outcomes such as recurrence of obstruction, adhesion formation, and long-term quality of life.
Conclusion
5
Laparoscopy appears to be a safe and effective option for pediatric acute SBO in appropriately selected patients. It may offer benefits in recovery time and hospital stay without increasing complication rates. However, these findings are limited by this study’s retrospective design and selection criteria.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wassmer CH Revol R Uhe I Chevallay M Toso C Gervaz P A new clinical severity score for the management of acute small bowel obstruction in predicting bowel ischemia: a cohort study. Int J Surg. (2023) 109(6):1620–8. 10.1097/JS 9.000000000000017137026805 PMC 10389338 · doi ↗ · pubmed ↗
- 2Subramanian A Swaminathan C Siby J Singh A Gulab A. Laparoscopic management of acute small bowel obstruction: a retrospective study at a Tertiary Center in the United Kingdom. Cureus. (2024) 16(10):e 71089. 10.7759/cureus.7108939386931 PMC 11463905 · doi ↗ · pubmed ↗
- 3Adejumo AA Alegbejo-Olarinoye MI Akims SM Akanbi OO. Acute small-bowel obstruction: an appraisal of common etiology and management at the Federal Medical Centre, Keffi, North-Central Nigeria. Ann Afr Med. (2024) 23(3):313–6. 10.4103/aam.aam_111_2339034552 PMC 11364338 · doi ↗ · pubmed ↗
- 4Yamada T Okabayashi K Hasegawa H Tsuruta M Yoo JH Seishima R Meta-analysis of the risk of small bowel obstruction following open or laparoscopic colorectal surgery. Br J Surg. (2016) 103(5):493–503. 10.1002/bjs.1010526898718 · doi ↗ · pubmed ↗
- 5Behman R Nathens AB Byrne JP Mason S Look Hong N Karanicolas PJ. Laparoscopic surgery for adhesive small bowel obstruction is associated with a higher risk of bowel injury: a population-based analysis of 8584 patients. Ann Surg. (2017) 266(3):489–98. 10.1097/SLA.000000000000236928657949 · doi ↗ · pubmed ↗
- 6Sallinen V Di Saverio S Haukijarvi E Juusela R Wikstrom H Koivukangas V Laparoscopic versus open adhesiolysis for adhesive small bowel obstruction (lasso): an international, multicentre, randomised, open-label trial. Lancet Gastroenterol Hepatol. (2019) 4(4):278–86. 10.1016/S 2468-1253(19)30016-030765264 · doi ↗ · pubmed ↗
- 7Gutt CN Oniu T Schemmer P Mehrabi A Buchler MW. Fewer adhesions induced by laparoscopic surgery? Surg Endosc. (2004) 18(6):898–906. 10.1007/s 00464-003-9233-315108105 · doi ↗ · pubmed ↗
- 8Aguayo P Fraser JD Ilyas S St Peter SD Holcomb GW 3rd Ostlie DJ. Laparoscopic management of small bowel obstruction in children. J Laparoendosc Adv Surg Tech A. (2011) 21(1):85–8. 10.1089/Lap.2010.016521214380 · doi ↗ · pubmed ↗