Self‐reported changes in adolescent mental health, deliberate self‐harm, substance use, and help‐seeking behavior before and after the COVID‐19 pandemic – A Finnish time‐trend study
Andre Sourander, Xiao Zhang, Omid Dadras, Anne Abio, Kaisa Mishina, Tiia Ståhlberg, Yuko Mori, Sonja Gilbert, Emmi Heinonen, David Gyllenberg

TL;DR
This study shows that adolescent mental health and self-harm behaviors increased significantly in Finland after the COVID-19 pandemic, especially among girls.
Contribution
The study compares mental health trends pre- and post-pandemic using identical survey designs across three time points.
Findings
Females showed significant increases in mental health issues, self-harm, and substance use after the pandemic.
Males experienced smaller increases in mental health problems and decreased alcohol consumption.
Minimal changes were observed between 2014 and 2018, suggesting pandemic-specific effects.
Abstract
Despite the impact that the COVID‐19 pandemic had on adolescents' mental health, there is a lack of studies comparing it pre‐ and postpandemic using consistent designs and measurements. Therefore, this study aimed to analyze changes in adolescent psychopathology, deliberate self‐harm behavior, substance use, and help‐seeking behavior pre‐ and post‐COVID‐19, with an identical study design. The study included three repeated cross‐sectional studies conducted in 2014, 2018, and 2023, including self‐reported data from Finnish secondary school students in grades 7 to 9, aged 13 to 16 (n = 9,024). The survey measured demographic information, mental health using the Strengths and Difficulties Questionnaire (SDQ), deliberate self‐harm behavior, substance use, and help‐seeking behavior. Comparing data in 2023 with 2018, there were significant increases among females in total SDQ score (OR 2.1,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
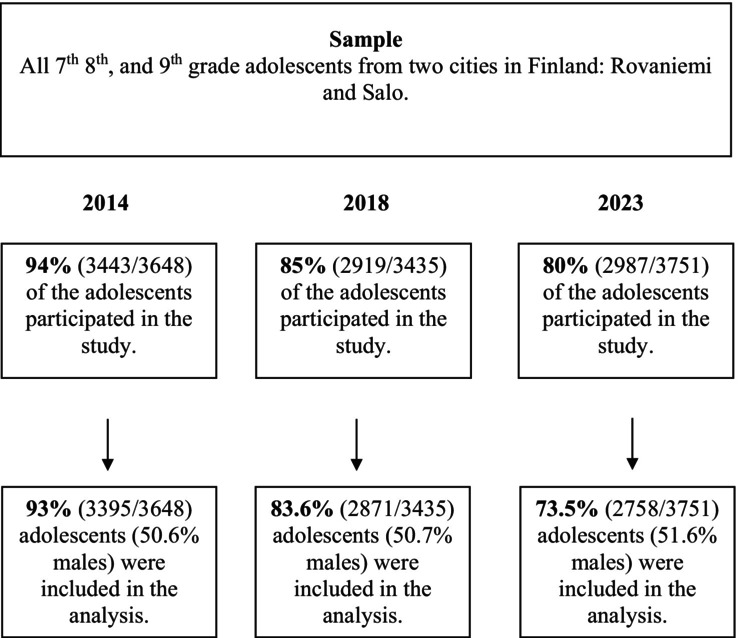 Figure 1
Figure 1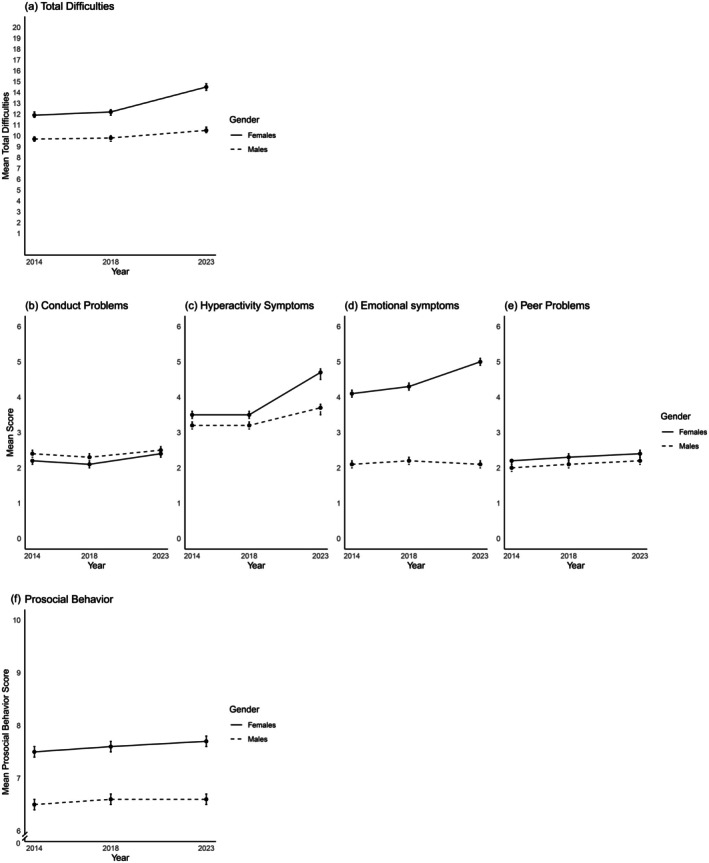 Figure 2
Figure 2| Characteristics | 2014 | 2018 | 2023 |
|
|---|---|---|---|---|
| ( | ( | ( | ||
| Gender (%) | 0.706 | |||
| Females | 1,678 (49.4) | 1,414 (49.3) | 1,335 (48.4) | |
| Males | 1,717 (50.6) | 1,457 (50.7) | 1,423 (51.6) | |
| School grade (%) | 0.708 | |||
| 7th graders | 1,167 (34.4) | 974 (34.0) | 906 (32.9) | |
| 8th graders | 1,128 (33.2) | 937 (32.7) | 914 (33.2) | |
| 9th graders | 1,098 (32.4) | 952 (33.3) | 930 (33.8) | |
| Family structure (%) | 0.114 | |||
| Two biological parents | 2,369 (70.4) | 2,067 (72.7) | 1,928 (70.2) | |
| One biological parent | 936 (27.8) | 719 (25.3) | 772 (28.1) | |
| Other | 58 (1.7) | 57 (2.0) | 48 (1.7) | |
| Parents background (%) |
| |||
| Both parents born in Finland | 3,079 (91.7) | 2,529 (89.1) | 2,355 (86.7) | |
| One parent born in Finland | 173 (5.2) | 189 (6.7) | 212 (7.8) | |
| Neither parent born in Finland | 106 (3.2) | 121 (4.3) | 148 (5.5) |
| 2014 | 2018 | 2023 | 2023 vs. 2018 | 2023 vs. 2014 | 2018 vs. 2014 | Overall year | |
|---|---|---|---|---|---|---|---|
| % | % | % | OR (98.3% CI) | OR (98.3% CI) | OR (98.3% CI) | ||
| SDQ | |||||||
| Females | 16.9 | 17.0 | 30.6 | 2.1 (1.7–2.7)*** | 2.2 (1.7–2.7)*** | 1.0 (0.8–1.3) |
|
| Males | 8.0 | 9.0 | 11.5 | 1.3 (0.9–1.9) | 1.6 (1.1–2.2)* | 1.2 (0.8–1.7) |
|
| Conduct problems score ≥cut‐off (5) | |||||||
| Females | 8.9 | 8.0 | 13.1 | 1.7 (1.1–2.7)** | 1.4 (1.0–2.2) | 0.8 (0.5–1.3) | 0.008 |
| Males | 12.1 | 10.1 | 13.1 | 1.3 (1.0–1.7) | 1.1 (0.8–1.4) | 0.8 (0.6–1.1) | 0.118 |
| Emotional symptoms score ≥cut‐off (7) | |||||||
| Female | 18.2 | 20.0 | 31.4 | 1.8 (1.5–2.3)*** | 2.1 (1.7–2.6)*** | 1.1 (0.9–1.4) | <.001 |
| Males | 2.3 | 4.3 | 3.2 | 0.8 (0.5–1.4) | 1.5 (0.8–2.8) | 1.9 (1.1–3.4)* | 0.024 |
| Hyperactivity symptoms score ≥cut‐off (6) | |||||||
| Female | 18.1 | 18.2 | 38.1 | 2.8 (2.2–3.6)*** | 2.8 (2.2–3.5)*** | 1.0 (0.8–1.3) | <0.001 |
| Males | 13.0 | 12.8 | 18.5 | 1.5 (1.2–1.9)*** | 1.5 (1.2–1.9)*** | 1.0 (0.8–1.3) | <0.001 |
| Peer problems score ≥cut‐off (4) | |||||||
| Females | 18.9 | 21.4 | 24.8 | 1.2 (1.0–1.6) | 1.4 (1.1–1.8)** | 1.2 (0.9–1.5) | 0.003 |
| Males | 17.4 | 19.7 | 21.6 | 1.1 (0.9–1.4) | 1.3 (1.0–1.6)* | 1.2 (0.9–1.5) | 0.015 |
| Prosocial behavior score ≤cut‐off (5) | |||||||
| Females | 14.7 | 12.2 | 11.7 | 0.9 (0.7–1.3) | 0.8 (0.6–1.0) | 0.8 (0.6–1.1) | 0.091 |
| Males | 30.1 | 28.3 | 29.1 | 1.1 (0.8–1.3) | 1.0 (0.8–1.2) | 0.9 (0.8–1.2) | 0.733 |
| Overall difficulties % | |||||||
| Female | |||||||
| Minor | 34.3 | 39.6 | 38.5 | 1.3 (1.1–1.7)** | 1.8 (1.5–2.2)*** | 1.3 (1.1–1.6)*** |
|
| Definite/Severe | 12.7 | 14.5 | 28.3 | 2.8 (2.0–3.7)*** | 3.6 (2.7–4.9)*** | 1.3 (1.0–1.8) | |
| Males | |||||||
| Minor | 30.9 | 29.5 | 31.6 | 1.2 (0.9–1.6) | 1.2 (0.9–1.5) | 1.0 (0.7–1.3) |
|
| Definite/Severe | 5.3 | 7.5 | 10.7 | 1.5 (1.0–2.1)* | 2.3 (1.6–3.2)*** | 1.5 (1.0–2.2)* | |
| Self‐harm % | |||||||
| Females | |||||||
| Once | 12.1 | 15.2 | 13.3 | 0.9 (0.7–1.2) | 1.2 (0.9–1.5) | 1.3 (1.0–1.7) |
|
| Multiple times | 6.9 | 9.1 | 12.2 | 1.4 (0.9–2.2) | 2.0 (1.3–3.0)*** | 1.4 (0.9–2.1) | |
| Males | |||||||
| Once | 3.2 | 4.3 | 3.8 | 0.8 (0.5–1.3) | 1.2 (0.7–1.9) | 1.4 (0.9–2.3) | 0.151 |
| Multiple times | 1.4 | 2.2 | 1.6 | 0.7 (0.4–1.4) | 1.2 (0.6–2.5) | 1.7 (0.8–3.3) | |
| 2014 | 2018 | 2023 | 2023 vs. 2018 | 2023 vs. 2014 | 2018 vs. 2014 | Overall year | |
|---|---|---|---|---|---|---|---|
| % | % | % | OR (98.3% CI) | OR (98.3% CI) | OR (98.3% CI) | ||
| Alcohol usage % | |||||||
| Females | |||||||
| Once a month or more | 22.4 | 21.0 | 17.5 | 0.7 (0.5–1.0) | 0.7 (0.5–0.9)* | 0.9 (0.7–1.3) | . |
| Once a week or more | 1.4 | 1.3 | 0.9 | 0.7 (0.3–1.8) | 0.6 (0.2–1.4) | 0.8 (0.4–1.8) | |
| Males | |||||||
| Once a month or more | 23.2 | 20.9 | 15.1 | 0.7 (0.5–0.9)*** | 0.6 (0.5–0.7)*** | 0.9 (0.7–1.1) |
|
| Once a week or more | 2.3 | 2.4 | 2.8 | 1.1 (0.6–2.2) | 1.1 (0.6–2.1) | 1.0 (0.5–1.9) | |
| Drunk % | |||||||
| Females | |||||||
| Once a month or more | 16.2 | 14.7 | 12.9 | 0.8 (0.5–1.2) | 0.7 (0.5–1.0) | 0.9 (0.6–1.3) | .222 |
| Once a week or more | 0.7 | 0.6 | 0.5 | 0.8 (0.2–2.6) | 0.7 (0.2–2.1) | 0.9 (0.3–2.6) | |
| Males | |||||||
| Once a month or more | 16.0 | 14.5 | 11.5 | 0.8 (0.6–1.1) | 0.7 (0.5–0.9) | 0.9 (0.6–1.2) | . |
| Once a week or more | 1.4 | 1.2 | 1.8 | 1.5 (0.6–3.3) | 1.2 (0.6–2.5) | 0.8 (0.4–1.8) | |
| Smoke % | |||||||
| Females | |||||||
| Rarely | 10.1 | 10.6 | 11.8 | 1.2 (0.9–1.6) | 1.2 (0.9–1.7) | 1.0 (0.8–1.4) | . |
| Weekly | 3.3 | 2.4 | 5.6 | 2.7 (1.5–4.9)*** | 1.8 (1.1–3.0)* | 0.7 (0.4–1.2) | |
| Daily | 5.7 | 4.7 | 7.0 | 1.5 (0.8–2.7) | 1.1 (0.6–2.1) | 0.8 (0.4–1.4) | |
| Males | |||||||
| Rarely | 12.3 | 10.5 | 10.5 | 0.9 (0.6–1.3) | 0.8 (0.6–1.1) | 0.8 (0.6–1.2) | . |
| Weekly | 4.7 | 3.1 | 4.1 | 1.3 (0.8–2.2) | 0.8 (0.5–1.3) | 0.6 (0.4–1.0) | |
| Daily | 11.5 | 9.0 | 7.5 | 0.9 (0.6–1.5) | 0.6 (0.4–1.0)* | 0.7 (0.4–1.0) | |
| Illegal drugs % | |||||||
| Females | |||||||
| Rarely | 1.8 | 2.1 | 2.4 | 1.2 (0.6–2.3) | 1.2 (0.7–2.3) | 1.0 (0.5–1.9) | .847 |
| Weekly | 0.5 | 1.0 | 1.0 | 1.0 (0.4–2.6) | 1.5 (0.5–4.3) | 1.5 (0.5–4.3) | |
| Daily | 1.1 | 0.8 | 1.1 | 1.2 (0.4–3.9) | 0.8 (0.3–2.2) | 0.7 (0.2–0.9) | |
| Males | |||||||
| Rarely | 2.2 | 2.2 | 2.4 | 1.0 (0.5–2.2) | 1.2 (0.5–2.5) | 1.1 (0.5–2.4) | .098 |
| Weekly | 1.4 | 2.1 | 1.2 | 0.6 (0.3–1.2) | 0.9 (0.4–2.0) | 1.5 (0.8–3.0) | |
| Daily | 1.1 | 0.8 | 1.9 | 2.2 (1.0–5.2) | 1.8 (0.9–3.8) | 0.8 (0.3–2.0) | |
| 2014 | 2018 | 2023 | 2023 vs. 2018 | 2023 vs. 2014 | 2018 vs. 2014 | Overall year | |
|---|---|---|---|---|---|---|---|
| % | % | % | OR (98.3% CI) | OR (98.3% CI) | OR (98.3% CI) |
| |
| Help‐seeking behavior % | |||||||
| Females | |||||||
| Have considered seeking help | 15.8 | 14.5 | 25.2 | 2.2 (1.7–2.9)*** | 2.1 (1.7–2.7)*** | 0.9 (0.7–1.2) |
|
| Have sought help | 16.1 | 18.6 | 22.2 | 1.5 (1.2–2.0)*** | 1.8 (1.4–2.4)*** | 1.2 (0.9–1.6) | |
| Males | |||||||
| Have considered seeking help | 5.4 | 5.9 | 6.5 | 1.0 (0.7–1.5) | 1.2 (0.9–1.8) | 1.2 (0.8–1.7) | .206 |
| Have sought help | 4.0 | 5.8 | 5.0 | 0.9 (0.6–1.4) | 1.3 (0.8–2.1) | 1.4 (0.9–2.3) | |
- —Juho Vainion Säätiö10.13039/501100004037
- —European Research Council10.13039/501100000781
- —NordForsk10.13039/501100004785
- —Academy of Finland10.13039/501100002341
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSuicide and Self-Harm Studies · COVID-19 and Mental Health · Child and Adolescent Psychosocial and Emotional Development
Key Practitioner MessageWhat is currently known?
- Adolescents' mental health has shown a notable decline after the COVID‐19 pandemic.
What has been shown?
- This repeated cross‐sectional study revealed increased psychopathology, deliberate self‐harm, and help‐seeking behavior, with minimal changes in substance use in the Finnish context.
What is the significance of this for clinical practice?
- The increased difficulties call for gender‐sensitive interventions and accessible services to address rising help‐seeking behavior.
Introduction
Several systematic reviews have demonstrated significant increases in adolescent mental health problems, particularly anxiety, depression, and deliberate self‐harm behavior following the COVID‐19 pandemic (Bower et al., 2023; Kauhanen et al., 2023; Orban et al., 2024; Sayed et al., 2024). These issues not only compromise individual well‐being but also carry significant societal implications, including increased healthcare costs and reduced productivity. Pandemic‐related factors, including fear of infection, concerns for loved ones, restrictions on social and physical activities due to lockdowns, isolation, family conflicts, and excessive exposure to media, are widely considered key contributors (Cheng, Wang, Wang, Zou, & Qu, 2023; Keyes & Platt, 2024; Panchal et al., 2021; Peng et al., 2023; Wiguna et al., 2024).
A recent review indicates increased internalizing problems among adolescents throughout the 21st century, attributed to earlier puberty onset, hormonal changes, increased use of digital devices, the COVID‐19 pandemic, and worsening macro‐economic conditions, such as economic instability and inequality (Keyes & Platt, 2024). There is also an expansion of adolescents reporting internalizing and several other problems over time, which needs to be considered when interpreting research findings (Haslam, 2016). Accurate assessment of time‐trend changes in adolescent mental health requires repeated population‐based cross‐sectional surveys with consistent sampling, regions, and methodologies (Collishaw, 2015). Many studies comparing prepandemic and early pandemic mental health face methodological inconsistencies, small samples, or a narrow focus on internalizing problems (e.g., Hafstad, Sætren, Wentzel‐Larsen, & Augusti, 2022; Ravens‐Sieberer et al., 2023).
Few population‐based studies have employed repeated cross‐sectional surveys with consistent methodologies to evaluate mental health changes before and after the pandemic, particularly in later phases (Kauhanen et al., 2023; Orban et al., 2024). A Norwegian study using nationwide school surveys from 2014 to 2022 observed increased adolescent cannabis and illicit drug use (Myhr, Vesterbekkmo, Samarawickrema, & Sund, 2024). An Icelandic study reported increases in depression and worsened mental well‐being from 2018 to 2022 (Thorisdottir et al., 2023). In Finland, a nationwide survey investigated generalized anxiety, depression, loneliness, social anxiety, and well‐being, reporting an increase in generalized anxiety, depression, and loneliness from 2019 to 2023, social anxiety from 2015 to 2023, along with a decline in overall well‐being from 2017 to 2023 (Kiviruusu et al., 2024). Another study from the Health Behavior in School‐aged Children examined Finnish adolescents between 2018 and 2022, identifying deterioration in mental health with increases in loneliness and psychosomatic complaints (Gustafsson et al., 2023). A German study spanning 2009 to 2022 examined subjective health and life satisfaction (Reiß et al., 2024). These studies compared multiple time points before and after the pandemic but focused primarily on internalizing problems, lacking consistent assessment of externalizing problems, substance use, and help‐seeking behavior. These gaps underscore the need for comprehensive studies using consistent methodologies to address these areas.
This study utilized three population‐based cross‐sectional samples from before the COVID‐19 pandemic (2014 and 2018) and after the peak of the pandemic (2023), each using identical designs, methods, and target populations to enable a consistent comparison. The study aimed to compare pre‐ and post‐COVID‐19 data to examine changes in adolescent internalizing and externalizing problems, deliberate self‐harm behavior, substance use, and help‐seeking behavior. We hypothesized that the prevalence of adolescent mental health problems and service utilization would be increased after the COVID‐19 pandemic.
Materials and methods
Participants and study procedure
This RoSa time‐trend study in Finland included three repeated cross‐sectional surveys conducted in spring 2014, 2018, and 2023, capturing data from both before and after the COVID‐19 pandemic. Participants were adolescents from Rovaniemi in Finnish Lapland (population ~ 60,000) and Salo in southern Finland (population ~ 52,000). Data collection was carried out in all secondary schools in these cities, excluding schools and classes for children with special needs.
The study collected data from 7th to 9th graders in Finnish secondary schools, aged 13 to 16 years. All students present on the survey day were invited to participate, completing questionnaires during class and sealing their responses in envelopes. Absent students were given the opportunity to participate later. Across all 3 years, a total of 9,283 questionnaires were collected. We performed an initial screening to remove questionnaires with inappropriate responses (11 (0.3%) in 2014, 13 (0.4%) in 2018, and 42 (1.4%) in 2023), such as uniform response patterns, logically inconsistent or invalid answers, or a large amount of missing data. Additionally, students under 13, over 16, or with missing age or sex information were excluded, resulting in a final sample of 9,024 students for analysis (Figure 1). For all other variables, listwise deletion was applied given the minimal amount of missing data.
Flowchart of respondent inclusion
This study has been approved by the Ethics Committee of the University of Turku in all 3 years, 2014, 2018, and 2023. Participation was entirely voluntary. Parental consent was obtained by informing parents about the study in advance, giving them the option to decline their adolescent's participation. The study followed the ethical standards from the 1964 Declaration of Helsinki and its later amendments.
Measures
In demographic section, we asked about their age, gender, city, school grade, family structure, and parental background. Family structure was categorized as living with two biological parents, one biological parent, or other. Parental background was based on country of birth and categorized as both parents born in Finland, one parent born in Finland, or neither parent born in Finland.
Mental health was assessed using the Strengths and Difficulties Questionnaire (SDQ) and one question about deliberate self‐harm behavior. The SDQ, translated and back‐translated from English to Finnish (Koskelainen, Sourander, & Vauras, 2001), includes 25 items across five scales: emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behavior (Goodman, 1997; Goodman & Scott, 1999). Responses ranged from 0 (not true) to 2 (certainly true), with subscale scores ranging from 0 to 10, with higher scores indicating greater difficulties, except for prosocial behavior. Five items were phrased positively and scored in reverse. The total difficulties score, calculated by summing the scores from the first four subscales, ranged from 0 to 40. Additionally, perceived difficulties in emotions, concentration, behavior, or getting along with other people were asked, with the option of ‘No’ and ‘Yes (Minor, definite, or severe difficulties)’. Deliberate self‐harm behavior was assessed with one question, ‘Have you intentionally harmed yourself by cutting or burning your skin in the past 6 months?’ with response options of ‘no’, ‘once’, or ‘multiple times’.
Substance use was assessed through questions on alcohol consumption, drunkenness, smoking/nicotine use, and illegal drug use. Participants reported alcohol use and drunkenness frequency with options: ‘not at all’, ‘once a month or more often’, and ‘once a week or more often’. Smoking/nicotine use frequencies were categorized as: ‘not at all’, ‘not often’, ‘every week’, and ‘every day’. Illegal drug use was measured with options: ‘never’, ‘once’, ‘2–4 times’, and ‘5 or more times’.
Help‐seeking behavior was assessed by asking: ‘Within the past six months, have you at any point felt a need for outside help (someone outside your immediate family) with your problems, feelings, behavior, or emotional trouble?’ with three options: ‘No, I have not felt the need’, ‘I have considered getting outside help’, and ‘I have sought outside help’. Those selecting ‘I have sought outside help’ could specify the source, such as friends, relatives, or teachers.
Statistical method
For background characteristics, frequencies and percentages were calculated for each year, and Pearson's Chi‐square test was used to compare the distributions. The outcomes were analyzed in two ways. First, categorical analyses used the SDQ total difficulties and subscores categorized by the 90th percentile based on the 2014 total sample (10th percentile for prosocial), as suggested by previous studies on both Finnish and broader European samples (Goodman, 1997; Koskelainen et al., 2001; Sourander, Helstelä, & Helenius, 1999). Mixed effects logistic regression with school‐wise random intercepts compared the likelihood of scores above these thresholds across years. Mixed effects multinomial logistic regression was used for overall difficulties, deliberate self‐harm behavior, and substance use, with ‘None’, ‘No’, and ‘Not at all’ as reference categories. For self‐perceived difficulties, the options ‘Definite’ and ‘Severe’ were combined. Second, SDQ subscales and total difficulties were analyzed as continuous variables using mixed effects linear regression. Mixed effects logistic regression was used to analyze the interaction effect of year and sex on the categorical outcomes. Significant interactions of sex were found for some outcomes; thus, the analyses were performed separately for females and males.
For all outcomes, odds ratios and mean differences were calculated for pairwise comparisons between the three time points: 2014 versus 2018, 2018 versus 2023, and 2014 versus 2023. To minimize the risk of false positive results due to multiple comparisons, the Bonferroni correction was applied by dividing the significance level of 0.05 by 3, resulting in a significance threshold of 0.0167 and 98.33% confidence intervals. A Type III test provided overall p‐values to determine if outcomes differed significantly across years, with p‐values <.05 considered significant. All results were adjusted for city, grade, family structure, and parents' background.
All statistical analyses were carried out with SAS software, version 9.4 for Windows. The full analysis code is openly available (Appendix S1).
Results
Participants sociodemographic
Significant changes were observed in city distribution and parental background between 2014 and 2023. The sample from Rovaniemi comprised 52.4% of the responses in 2014, 47.1% in 2018, and 51.1% in 2023 (p < .001). The percentage of participants with both parents born in Finland decreased significantly across the years (p < .001). No significant differences were observed in gender, school grade, or family structure (Table 1).
Changes in mental health
Significant sex interactions were found for SDQ total scores and all subscales, so results are presented separately for females and males (Table S1).
Table 2 shows results comparing 2023 to 2018. Females showed significant increases in SDQ total scores (OR 2.2, 98.33% CI 1.7–2.7), conduct problems (OR 1.7, 98.33% CI 1.1–2.7), emotional symptoms (OR 1.8, 98.33% CI 1.5–2.3), and hyperactivity (OR 2.8, 98.33% CI 2.2–3.6). Males showed a significant increase only in hyperactivity (OR 2.5, 98.33% CI 1.2–1.9). Females also reported a notable rise in ‘definite/severe’ perceived difficulties from 14.5% in 2018 to 28.3% in 2023 (OR 2.8, 98.33% CI 2.0–3.7), while in males, it increased from 7.5% to 10.7% (OR 1.5, 98.33% CI 1.0–2.1). No significant change was found in peer problems, prosocial behavior, or deliberate self‐harm behaviors for either sex during this period.
When comparing 2023–2014, similar trends were observed among females for total SDQ scores, emotional symptoms, and hyperactivity (all p < .001). Males showed an increase in SDQ total scores (OR 1.6, 98.33% CI 1.1–2.2) and hyperactivity (OR 1.5, 98.33% CI 1.2–1.9). In the pre‐COVID period (2014–2018), only minor increases were observed in emotional symptoms among males and in perceived minor difficulties for both sexes (Table 2). These patterns are further illustrated in Figure 2A–F, which describe changes in mean SDQ total and subscale scores separated by sex. Table S2 provides detailed changes in psychopathology by comparing mean values across different time points. The findings align with the categorical analysis, showing significant increases in psychopathological problems post‐COVID, with minimal changes between the two pre‐COVID assessments.
(A) The trend of SDQ total mean score by gender across survey years. (B–E) The trend of SDQ subscale scores by gender across survey years. (F) The trend of SDQ prosocial behavior mean score by gender across survey years
Changes in deliberate self‐harm behavior
Deliberate self‐harm among females increased significantly only from 2014 to 2023, with the percentage of those reporting multiple self‐injury episodes rising from 6.9% to 12.2% (OR 2.0, 98.33% CI 1.3–3.0). Males showed no significant changes in deliberate self‐harm across the years (Table 2).
Changes in substance use
Comparing 2018 to 2023, weekly smoking/nicotine use increased significantly among females (OR 2.7, 98.33% CI 1.5–4.9), while male alcohol use decreased (OR 0.7, 98.33% CI 0.5–0.9). No other significant changes in substance use were observed between 2014 and 2023 (Table 3).
Changes in help‐seeking behavior
Among females, help‐seeking behavior increased significantly, with 22.2% having sought help and 25.2% considering by 2023 (sought help: OR 1.5, 98.33% CI 1.2–2.0; considered help: OR 2.2, 98.33% CI 1.7–2.9, compared to 2018). By contrast, no significant changes in help‐seeking were observed among males across years (Table 4).
Discussion
The current study reveals significant increases in mental health problems among Finnish adolescents before and after the COVID‐19 pandemic, particularly among females. Compared to prepandemic data from 2018, female adolescents in 2023 showed heightened rates of emotional symptoms, hyperactivity, conduct problems, and overall difficulties, while male adolescents demonstrated increases primarily in hyperactivity symptoms. Additionally, the frequency of deliberate self‐harm among females rose from 2014 to 2023. Substance use trends remained relatively stable, with an increase in weekly smoking among females as the only exception. These findings underscore a concerning postpandemic deterioration in adolescent mental health, especially among females, emphasizing the need for targeted mental health interventions and support.
This study offers several important contributions to the field by using repeated cross‐sectional surveys with the same design to comprehensively assess Finnish adolescent mental health before (2014, 2018) and after the pandemic (2023). Unlike studies focused solely on internalizing problems, this research takes a comprehensive approach, examining externalizing problems, deliberate self‐harm, substance use, and help‐seeking behavior. Multiple prepandemic reference points help isolate pandemic‐related changes, and the population‐based sample enhances the reliability and generalizability of the findings within the Finnish context.
Similar to our findings, previous studies have reported increases in internalizing disorders (Kiviruusu et al., 2024; Madigan, Racine, et al., 2023), eating disorders (Hartman‐Munick et al., 2022; Kiviruusu et al., 2024), and emergency visits for attempted suicide and self‐harm (Kiviruusu et al., 2024; Madigan, Korczak, et al., 2023) among adolescents after the onset of the COVID‐19 pandemic. Adolescents' sensitivity to global threats like the pandemic, climate crisis, and armed conflicts may contribute to these issues. Climate anxiety and worries, widely reported among adolescents, correlate with general anxiety and depression (Hickman et al., 2021; Lass‐Hennemann et al., 2024; Leonhardt, Granrud, Bonsaksen, & Lien, 2022; Sciberras & Fernando, 2022; Wu et al., 2023; Wullenkord, Tröger, Hamann, Loy, & Reese, 2021). Additionally, given Finland's proximity to Russia, the perceived threat of war may have been particularly impactful on Finnish adolescents (The Advisory Board for Defence Information [ABDI], 2024).
Consistent with our findings, emotional problems were discovered among females. A Finnish study reported increases in anxiety, depression, eating disorder symptoms, and suicidal behavior during and after the pandemic, while males showed no such increases (Kiviruusu et al., 2024). The gender difference highlights a critical area of concern that the pandemic's role in exacerbating pre‐existing gender disparities in mental health is consistent with prepandemic findings of greater internalizing symptoms among females (Deng et al., 2023; Kauhanen et al., 2023; Keyes & Platt, 2024). One contributing factor may be the heightened sensitivity of girls to some potential negative effects of social media exposure compared with boys (Keles, McCrae, & Grealish, 2020; Kelly, Zilanawala, Booker, & Sacker, 2018; Twenge, 2020). Some studies also suggested that females are more prone to climate anxiety (Heeren, Mouguiama‐Daouda, & Contreras, 2022; Wullenkord et al., 2021).
We also observed a rise in hyperactivity symptoms among both female and male adolescents, with a particularly sharp increase in females. This indicates growing trends of restlessness, impulsivity, and poor concentration, worsening after COVID‐19. These findings align with a Finnish population study reporting an 18.6% increase in ADHD diagnoses, especially among females aged 12–30 from 2019 to 2022 (Auro, Holopainen, Perola, Havulinna, & Raevuori, 2024). Changes in school, social, and learning environments during the pandemic may have contributed to this trend (Auro et al., 2024). While our study focused on hyperactivity, which differs from ADHD, the documented co‐occurrence of hyperactivity and anxiety may explain the parallel increase in emotional problems and hyperactivity symptoms (Jarrett & Ollendick, 2008).
It is concerning to note that deliberate self‐harm was already prevalent among adolescents before the pandemic, and this trend has only worsened. Deliberate self‐harm is common in the general adolescent population, particularly among females (Kiviruusu et al., 2024; Madigan, Korczak, et al., 2023; Monto, McRee, & Deryck, 2018). The higher prevalence among females aligns with results from the United States (Monto et al., 2018). Our findings align with global trends, showing 12‐month self‐harm rates of approximately 19.5% across high‐income and low‐ to middle‐income countries. Increases in adolescent hospitalizations for self‐harm injuries have been reported globally, including in Australia, Canada, the United States, and Europe, pre‐ and during COVID‐19 (Corrigan et al., 2022; Hiscock et al., 2022; Ougrin et al., 2022; Petruzzelli et al., 2022; Shankar et al., 2022; Steeg et al., 2021; Zhang, Davis, Finkelstein, & Rosenfield, 2022). The rise in deliberate self‐harm among females in this study may relate to increased psychopathology, while this study specifically examines general deliberate self‐harm behavior without considering underlying reasons, such as suicidal intentions. Furthermore, in this survey, we used a single item to assess deliberate self‐harm behavior, which may result in lower prevalence estimates compared to using a checklist (Aspeqvist, Andersson, Korhonen, Dahlström, & Zetterqvist, 2024). The item specifically referred to cutting or burning and may have excluded other common forms of self‐injurious behavior – such as self‐hitting, head‐banging, biting, or scratching oneself to cause pain – potentially leading to an underestimation of the overall prevalence of self‐harm.
Regarding substance use, our study found a relatively stable trend before and after the COVID‐19 pandemic, with decreases in alcohol use and drunkenness decreasing among females and males, aligning with findings from other Western countries. A systematic review of over 20 countries reported declines in adolescent substance use during the pandemic, including alcohol, cannabis, tobacco, and vaping (Layman et al., 2022), likely due to public health restrictions limiting access and socialization. However, while the trend of nicotine use among Finnish adolescents has previously been decreasing or stable (Mishina, Heinonen, Lempinen, & Sourander, 2024; Ollila & Ruokolainen, 2023), our findings suggest a reversal in this trend. The increase may be partly due to the rising popularity of new nicotine products, such as vaping and nicotine pouches. Finnish data have also reported increases in vaping since 2021, especially among adolescent females, and the use of nicotine pouches has reached the same level as the use of snus (Ollila & Ruokolainen, 2023). Considering the rising popularity of these new, alternative tobacco products, it is crucial to monitor this trend closely in the future (Speciale, Rao, Yang, & Nugent, 2023).
After the pandemic, there was a significant increase in females seeking mental health support, with nearly half actively considering or seeking help. The use of child and adolescent psychiatric services decreased early in the pandemic (Revet et al., 2022; Wan Mohd Yunus et al., 2022), but gradually increased later (Kalmin et al., 2023). Generally, women are more likely than men to seek help, and this difference may have been further accentuated by the pandemic (Westberg, Nyholm, Nygren, & Svedberg, 2022). Moreover, this study revealed a significant increase in emotional and conduct problems among females after the pandemic, potentially leading to increased help‐seeking behaviors.
There are several limitations to our study. First, the findings based on the Finnish sample may not be generalizable to other countries, but the populations of Rovaniemi and Salo were highly comparable with Finland's general population in terms of demographics (StatFin, 2023). Second, the study relies solely on self‐reports, which, though valuable for assessing adolescent mental health, could be strengthened by including input from parents or teachers. Third, the overall response rate is high, but it has slightly declined from 2014 to 2023. Nonparticipants may have had greater difficulties, potentially leading to an underestimation of problems in our sample (Kearney, 2008). However, since the study was conducted using similar methods each time, it is likely that absenteeism occurred similarly each year. Fourth, this study applied listwise deletion to handle missing data, which may introduce bias. However, given the very low proportion of missing data in our study, the impact on the results is likely minimal.
Conclusion
This study provides valuable insights into adolescent mental health by analyzing the impact of COVID‐19 through three repeated cross‐sectional surveys. By examining internalizing and externalizing problems, deliberate self‐harm, substance use, and help‐seeking behavior, it offers a more integrated perspective. Our findings reveal a concerning trend of increased emotional symptoms and deliberate self‐harm among females, as well as a rise in hyperactivity among both genders. The findings highlight a decline in adolescent well‐being after the COVID‐19 pandemic, suggesting a prolonged trend and the need for continued attention to adolescent mental health, as well as the implementation of effective interventions, particularly for females.
Future research should continue monitoring these trends. The future RoSa study data collection using the same questionnaire and methodology is planned for 2026 and 2029. Additionally, it is important to explore the underlying mechanisms contributing to these mental health trends. Future research can address this issue through approaches such as qualitative research and longitudinal studies, which provide deeper insights into adolescents' experiences and the long‐term factors influencing their well‐being.
Conflict of interests
The authors declare no competing interests.
Funding
The European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program (grant agreement No. 101020767; ERC Advanced, Andre Sourander); the Research Council of Finland (decision number: 345546); the Juho Vainio Foundation; the Academy of Finland Special funding for research on the COVID‐19 epidemic and the mitigation of its effects (decision number: 335690); and Nordforsk (Welfare among Children and Young People in the Post‐Pandemic Nordics, decision number 156858).
Ethics
The Ethics Committee of the University of Turku approved the study (2014, 2018, and 2023). The study followed the ethical standards from the 1964 Declaration of Helsinki and its later amendments. Parental consent was obtained by informing parents about the study in advance, giving them the option to decline their adolescent's participation.
Supporting information
Appendix S1. SAS codes.
Table S1. Descriptive statistics and changes in SDQ total and subscales across three time points (2014, 2018, and 2023). Mixed linear regression results are adjusted for city, grade, family structure, and parental background.
Table S2. Interaction effects of year and sex on adolescent mental health, self‐harm, substance use, and help‐seeking behaviors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aspeqvist, E. , Andersson, H. , Korhonen, L. , Dahlström, Ö. , & Zetterqvist, M. (2024). Measurement and stratification of nonsuicidal self‐injury in adolescents. BMC Psychiatry, 24, 107.38326791 10.1186/s 12888-024-05535-3PMC 10848387 · doi ↗ · pubmed ↗
- 2Auro, K. , Holopainen, I. , Perola, M. , Havulinna, A.S. , & Raevuori, A. (2024). Attention‐deficit/hyperactivity disorder diagnoses in Finland during the COVID‐19 pandemic. JAMA Network Open, 7, e 2418204.38935377 10.1001/jamanetworkopen.2024.18204 PMC 11211961 · doi ↗ · pubmed ↗
- 3Bower, M. , Smout, S. , Donohoe‐Bales, A. , O'Dean, S. , Teesson, L. , Boyle, J. , … & Teesson, M. (2023). A hidden pandemic? An umbrella review of global evidence on mental health in the time of COVID‐19. Frontiers in Psychiatry, 14, 1–19.10.3389/fpsyt.2023.1107560 PMC 1003237736970258 · doi ↗ · pubmed ↗
- 4Cheng, H. , Wang, D. , Wang, L. , Zou, H. , & Qu, Y. (2023). Global prevalence of self‐harm during the COVID‐19 pandemic: A systematic review and meta‐analysis. BMC Psychology, 11, 1–15.37147683 10.1186/s 40359-023-01181-8PMC 10160734 · doi ↗ · pubmed ↗
- 5Collishaw, S. (2015). Annual Research Review: Secular trends in child and adolescent mental health. Journal of Child Psychology and Psychiatry, 56, 370–393. 10.1111/jcpp.12372 25496340 · doi ↗ · pubmed ↗
- 6Corrigan, C. , Duke, G. , Millar, J. , Paul, E. , Butt, W. , Gordon, M. , … & Oberender, F. (2022). Admissions of children and adolescents with deliberate self‐harm to intensive care during the SARS‐Co V‐2 outbreak in Australia. JAMA Network Open, 5, e 2211692.35544133 10.1001/jamanetworkopen.2022.11692 PMC 9096595 · doi ↗ · pubmed ↗
- 7Deng, J. , Zhou, F. , Hou, W. , Heybati, K. , Lohit, S. , Abbas, U. , … & Heybati, S. (2023). Prevalence of mental health symptoms in children and adolescents during the COVID‐19 pandemic: A meta‐analysis. Annals of the New York Academy of Sciences, 1520, 53–73.36537131 10.1111/nyas.14947 PMC 9880764 · doi ↗ · pubmed ↗
- 8Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 38, 581–586.9255702 10.1111/j.1469-7610.1997.tb 01545.x · doi ↗ · pubmed ↗