Contralateral Axillary Metastasis With Synchronous Ipsilateral Axillary Metastasis From Occult Breast Cancer: A Case Report With a Review of the Literature
William Swee Keong Khoo, Rasika Hendahewa

TL;DR
This case report describes a rare instance of breast cancer with metastasis to both axillary lymph nodes from an undetectable primary tumor.
Contribution
The novelty lies in presenting a rare combination of contralateral and ipsilateral axillary metastasis from occult breast cancer in one patient.
Findings
A 67-year-old woman presented with left axillary metastasis from occult breast cancer.
She also had synchronous contralateral axillary metastasis, highlighting the complexity of this rare condition.
The case emphasizes the need for tailored therapeutic approaches based on current guidelines.
Abstract
Occult breast cancer (OBC) is a rare presentation of breast cancer, characterised by evidence of metastasis to axillary lymph nodes without a clear radiological lesion in the breast. Contralateral axillary metastasis (CAM) in breast cancer is another rare presentation, with various differentials. This case report presents a 67-year-old female with left axillary metastasis from an OBC with synchronous CAM. This case highlights the complexities of both rare presentations in a single patient and discusses the pertinent therapeutic recommendations from current literature and guidelines.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1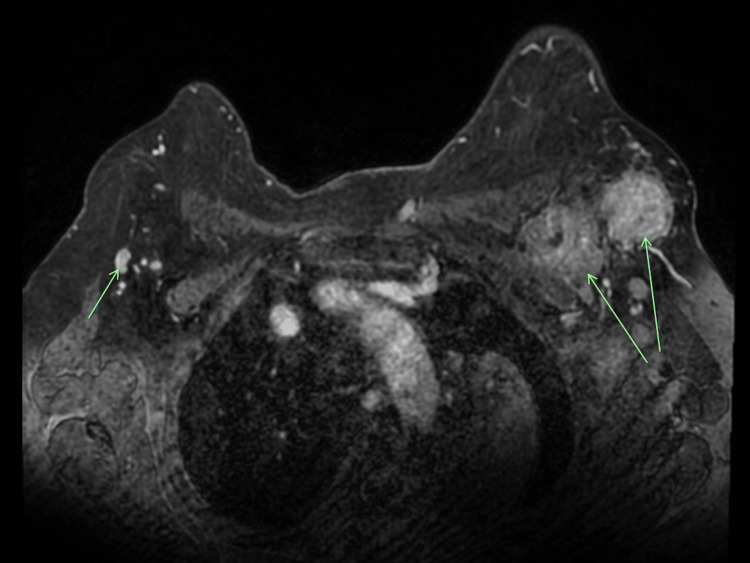 Figure 2
Figure 2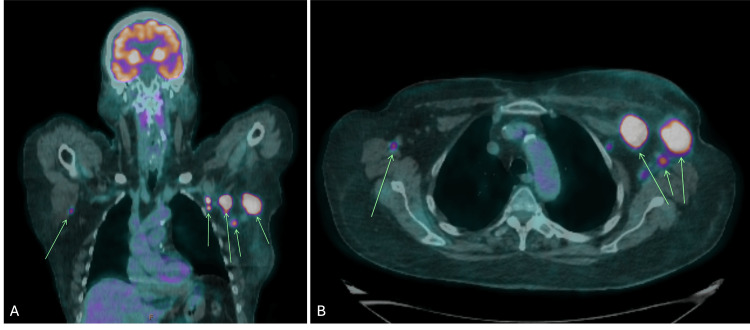 Figure 3
Figure 3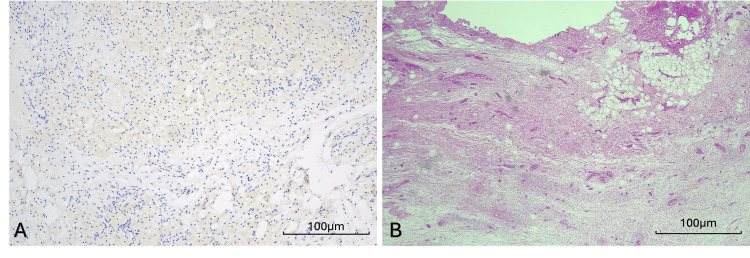 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Breast Lesions and Carcinomas · Breast Cancer Treatment Studies
Introduction
Occult breast cancer (OBC) is a rare presentation of breast cancer, characterised by breast carcinoma that has metastasised to the axillary lymph nodes, with the absence of radiological disease in the breast [1-3]. Contralateral axillary metastasis (CAM) in breast cancer is another rare occurrence, with differentials including contralateral metastasis from the primary breast cancer, metastasis from a separate ipsilateral primary breast cancer, or metastasis from another primary cancer of extramammary origin [4].
This case presents a 67-year-old female with left axillary metastasis from an OBC with synchronous CAM. Her treatment included neoadjuvant chemotherapy (NACT), bilateral mastectomy with bilateral axillary lymph node dissection (ALND), and adjuvant radiotherapy. This case highlights the complexities of both rare presentations in a single patient and discusses the pertinent therapeutic recommendations from current literature and guidelines.
Case presentation
A 67-year-old woman was referred to the General Surgery Breast Clinic with a five-week history of left axillary swelling. The patient had a history of hypertension, a benign breast lumpectomy five years ago, and a hysterectomy at 34 years of age. She has no known family history of breast or ovarian cancer, is an ex-smoker of 20 pack-years, and drinks alcohol regularly. Her gynaecological history includes menarche at the age of 15 years, no previous contraception use, and she has never breastfed. A bedside examination revealed palpable left axillary lymphadenopathy, with no palpable breast lumps bilaterally.
An initial workup with breast ultrasound and mammogram revealed suspicious pathological lymphadenopathy in the bilateral axillae (Figure 1). However, no obvious changes were identified on the mammogram, aside from mild dermal thickening of the left breast, which was benign on punch biopsy of the left breast skin. A fine-needle aspirate (FNA) of the largest left axillary lymph node revealed pleomorphic lobular carcinoma with changes consistent with metastatic breast carcinoma, which was estrogen receptor (ER) negative, progesterone receptor (PR) negative, and human epidermal growth factor receptor 2 (HER2) positive.
(A) Right breast MLO view and (B) Left breast MLO viewMammogram demonstrating bilateral axillary lymphadenopathy suspicious for metastasis as indicated by arrows.MLO, median lateral oblique
Subsequent investigations with a breast magnetic resonance imaging (MRI) revealed evidence of bilateral lymphadenopathy, with no clear breast lesions identified (Figure 2). Whole-body positron emission tomography-computed tomography (PET-CT) revealed intense abnormal fluorodeoxyglucose (FDG) uptake, consistent with metastatic lymphadenopathy in the left axilla and clavipectoral region, with a small FDG-avid focus in the right axilla, suspicious for contralateral axillary lymph node metastasis (Figure 3). Additionally, FNA biopsy of the right axillary lymph node demonstrated metastatic pleomorphic lobular carcinoma, which was ER and PR negative, but HER2 positive.
Axial view of MRIAxial view of MRI, demonstrating bilateral axillary lymphadenopathy (indicated with arrows), without evidence of pathological lesions in either breast.MRI, magnetic resonance imaging
(A) Coronal view and (B) Axial viewPET scan demonstrating intense abnormal FDG uptake, consistent with metastatic left axillary lymphadenopathy, with a focus of FDG avidity in the right axilla, suspicious for contralateral axillary lymph node metastasis (as indicated by arrows).PET, positron emission tomography; FDG, fluorodeoxyglucose
After discussion of the patient’s case in the Breast Surgery Multidisciplinary Team (MDT) meeting, the decision was made for NACT with carboplatin/doxetaxel and Herceptin. A follow-up staging CT and bilateral breast and axilla ultrasound scan (USS), three months post-initial workup, demonstrated a favourable treatment response of the bilateral axillary lymphadenopathy, without further evidence of progression of metastatic disease. A core biopsy of a newly identified left breast lump at 3 o’clock, 3 cm from the nipple, was conducted but demonstrated benign breast parenchyma. Unfortunately, NACT was ceased prematurely after three cycles due to toxicity.
A decision was made for a bilateral mastectomy with bilateral ALND. Histopathological results revealed no residual malignancy in the bilateral breasts, no residual carcinoma in 27 lymph nodes in the right axilla (one node with treatment-related changes), and no residual carcinoma in nine lymph nodes in the left axilla (two nodes with treatment-related changes) (Figure 4).
(A) Cytokeratin AE1/AE3 staining and (B) H&E stainingHistopathological slides of interest demonstrate the tumour bed from the left axilla, with evidence of treatment-related changes, but no residual tumour.Scale bar represents 100 µm; magnification 20×, for figures (A) and (B).H&E, haematoxylin and eosin
The patient was subsequently referred for adjuvant radiation to the left supraclavicular and clavipectoral nodes. However, prior to commencement of radiation therapy, the patient developed a progressive three-week history of worsening balance, headaches, and nausea. A CT brain demonstrated a new 38 mm left cerebellar lesion, consistent with leptomeningeal disease. This was deemed unresectable, and, after further discussions with the Community Palliative Care Team, the patient and her family subsequently decided to transition to comfort care, and she subsequently passed away.
Discussion
Breast cancer is the most common cause of malignancy and the second leading cause of cancer-related death in women globally [5,6]. Screening for breast cancer includes the early detection of breast cancer, with mammography as the gold-standard imaging modality [6]. In Australia, screening mammography is recommended for all women aged 50 to 74, biennially [7]. While most breast lesions can be identified clinically or via imaging, very rarely, an OBC may occur.
OBC is a rare presentation of breast cancer, characterised by breast carcinoma that has metastasised to the axillary lymph nodes, with the absence of radiological disease in the breast [1,2]. Most commonly, patients with OBC present with new axillary lymphadenopathy as their initial presentation [2]. Apart from the conventional imaging modalities of an ultrasound and a mammogram, a breast MRI is often recommended to improve the detection of occult primary breast cancer [1]. In addition, breast MRI is also useful to assess the extent of disease, evaluate response to neoadjuvant treatment, and assess lymph nodes and occult primary tumours [8].
Historically, the surgical management of the breast in OBC was a mastectomy, while ALND remains the mainstay of surgical management of the axilla [3]. The current guidelines by the National Comprehensive Cancer Network (NCCN) for OBC recommend mastectomy with ALND, or ALND and whole-breast radiotherapy; however, treatment of the ipsilateral breast remains contentious due to the various prognoses in clinical practice [2]. Interestingly, a recent meta-analysis conducted by Wang et al. in 2023, involving 3,476 patients across 13 studies, demonstrated the role of NACT in the treatment of OBC, improving patient survival [2]. In addition, the evolving role of NACT may also allow for de-escalation of axillary surgery - though further long-term research is required to support this hypothesis [3].
CAM in breast cancer is another rare occurrence, with differentials including a contralateral metastasis from the primary breast cancer, metastasis from a separate primary ipsilateral breast cancer, or metastasis from another primary cancer of extramammary origin [4]. Given the presence of metastatic breast cancer to the contralateral axilla, CAM is regarded as a stage IV disease, with the classification of M1 [9].
However, the occurrence of CAM could be due to differences in the usual lymphatic drainage pathway - thus suggesting that CAM could be classified as a variable presentation of locoregional, rather than systemic, disease [4,10]. Treatment options for CAM favour chemoradiotherapy, while contralateral mastectomy is not routinely recommended, except in specific scenarios, such as CAM with different pathological features from the primary malignancy [4].
Conclusions
In conclusion, OBC and CAM are both rare and complex presentations of breast cancer. This case highlights the complexities and diagnostic dilemmas of OBC and CAM. It is important for clinicians to have a high index of suspicion when there is evidence of metastatic breast cancer, regardless of a clear primary breast malignancy. While an ALND remains the mainstay of surgical management of the axilla for OBC, there are yet to be consensus guidelines on the management of the breast. CAM is a rare presentation in breast cancer, with controversy surrounding its classification as a locoregional rather than systemic disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Occult breast cancer: where are we at?Breast Ofri A Moore K 2112155420203313048710.1016/j.breast.2020.10.012PMC 7599122 · doi ↗ · pubmed ↗
- 2Best treatment options for occult breast cancer: a meta-analysis Front Oncol Wang R Yang HX Chen J Huang JJ Lv Q 10512321320233725192710.3389/fonc.2023.1051232 PMC 10213692 · doi ↗ · pubmed ↗
- 3De-escalation of surgery for occult breast cancer with axillary metastasis Surgery Holt AC Haji F Mc Closkey S Baker JL 41041217420233716040810.1016/j.surg.2023.03.020 · doi ↗ · pubmed ↗
- 4Contralateral axillary lymph node metastasis of breast cancer: retrospective analysis and literature review Front Oncol Zhang L Wang XZ Li C Yu Q Liu Z Yu ZY 8693971220223549401910.3389/fonc.2022.869397 PMC 9047860 · doi ↗ · pubmed ↗
- 5Cancer statistics, 2024 CA Cancer J Clin Siegel RL Giaquinto AN Jemal A 12497420243823076610.3322/caac.21820 · doi ↗ · pubmed ↗
- 6Global guidelines for breast cancer screening: a systematic review Breast Ren W Chen M Qiao Y Zhao F 85996420223563634210.1016/j.breast.2022.04.003PMC 9142711 · doi ↗ · pubmed ↗
- 7Breast Screen Australia monitoring report 2024 10 2025 2024 https://www.aihw.gov.au/reports/cancer-screening/breastscreen-australia-monitoring-report-2024/report-editions
- 8Breast MRI: clinical indications, recommendations, and future applications in breast cancer diagnosis Curr Oncol Rep Wekking D Porcu M De Silva P Saba L Scartozzi M Solinas C 2572672520233674949310.1007/s 11912-023-01372-x · doi ↗ · pubmed ↗