Coexistence of Adult-Onset Still's Disease and Graves' Disease: Coincidence or Continuum?
Inass Chaari, Ayoub Idrissi, Lahoussaine Abainou, Hamza El Jadi, Azzelarab Meftah, Hicham Baizri

TL;DR
This paper explores the rare coexistence of Adult-Onset Still's Disease and Graves' Disease, suggesting a possible shared immune mechanism.
Contribution
The paper highlights a potential pathophysiological link between two rare autoimmune diseases through a case study and literature review.
Findings
A 22-year-old patient exhibited both AOSD and GD, with overlapping immune dysregulation.
Shared genetic susceptibility and cytokine involvement suggest a possible continuum between the two diseases.
Systematic thyroid screening is recommended for AOSD patients to detect coexisting GD.
Abstract
Adult-onset Still’s disease (AOSD) is a rare systemic autoimmune disorder of unclear etiology, typically characterized by prolonged fever, arthralgia, transient rash, and leukocytosis. Graves’ disease (GD) is a common autoimmune cause of hyperthyroidism in young adults. Although associations between autoimmune conditions have been reported, the coexistence of AOSD and GD remains uncommon. We describe the case of a 22-year-old patient presenting with clinical and biochemical hyperthyroidism, confirmed by thyroid scintigraphy. The clinical picture was further complicated by persistent inflammatory syndrome, marked hyperferritinemia, and hepatosplenomegaly, consistent with AOSD as defined by Yamaguchi’s criteria. The disease course was characterized by recurrent inflammatory flares of both conditions and the development of carbimazole-induced hepatocellular injury, necessitating…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1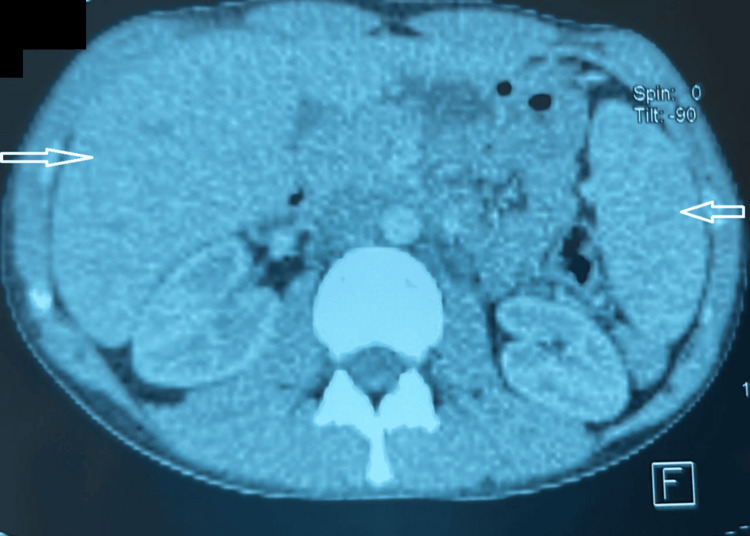 Figure 2
Figure 2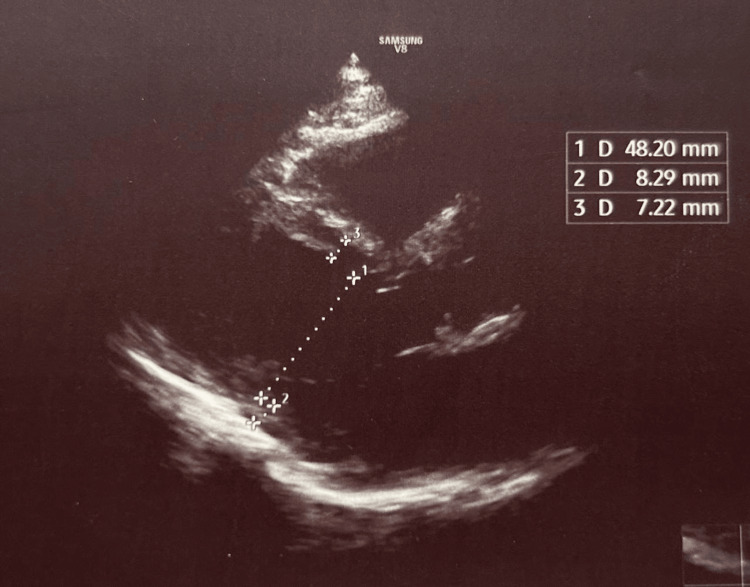 Figure 3
Figure 3| Date | Leukocytes (NR: 4000-11000 /mm³) | Free T4 (pmol/L) (NR: 12-22) | TSH (mU/L) (NR: 0.25-5) | AST (U/L) (NR: <50) | ALT (U/L) (NR: <65) | CRP (mg/L) (NR: <5) | Treatment received |
| February 17, 2024 | 10650 | 309 | 0.008 | 29 | 29.8 | Not available | Carbimazole 40 mg/day |
| March 6, 2024 | 12400 | 40.77 | Not available | 76 | 45 | 66.8 | Treatment discontinued |
| April 9, 2024 | 14300 | 7.32 | Not available | 208.39 | 254.84 | 116.8 | Prednisolone 60 mg/day |
| May 2, 2024 | 8600 | 14.8 | Not available | 67.5 | 120.4 | 14 | |
| June 2, 2024 | 7500 | 19.91 | 3.68 | 21 | 29 | Not available |
| Authors (references) | Country | Year | Patient age | Patient sex | Response to treatment (corticosteroids) |
| Hu et al. [ | China | 2014 | 43 years | Female | Good response |
| Torigoe et al. [ | Japan | 2011 | 50 years | Female | Good response |
| 1995 | 47 years | Female | Good response | ||
| 1996 | 52 years | Female | Good response | ||
| 1996 | 26 years | Female | Good response | ||
| 2001 | 30 years | Female | Good response | ||
| Chen et al. [ | Taiwan | 2010 | 37 years | Female | Good response |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders Research · Otitis Media and Relapsing Polychondritis · Inflammasome and immune disorders
Introduction
Adult-onset Still’s disease (AOSD) is a rare systemic autoimmune disorder of uncertain etiology. Graves’ disease (GD) is an autoimmune thyroid condition and represents the leading cause of hyperthyroidism in young adults.
An association between autoimmune thyroid disorders and rheumatoid arthritis has previously been documented [1]. Since AOSD is regarded as a clinical variant of rheumatoid arthritis [2], it may also coexist with autoimmune hyperthyroidism in some patients, as well as with myasthenia gravis, systemic lupus erythematosus [3], and Sjögren’s syndrome [4].
We report a case of AOSD occurring concomitantly with GD, suggesting that auto-inflammatory processes may act as a potential trigger for recurrent thyroid dysfunction. Beyond the rarity of this coexistence, our observation underlines the importance of systematic thyroid function screening in patients with AOSD [5,6].
Case presentation
We report the case of a 22-year-old male with no significant past medical history who presented with a three-month history of polyarthralgia associated with unquantified weight loss and recurrent fever. There was no cutaneous rash or odynophagia. Cervical examination revealed a diffusely enlarged thyroid gland of elastic consistency, without palpable nodules or cervical lymphadenopathy. Notably, clinical assessment did not demonstrate exophthalmos.
Biological investigations supported the diagnosis of GD, with suppressed thyroid-stimulating hormone (TSH) less than 0.008 mU/L (reference: 0.25-5), markedly elevated free T4 at 309 pmol/L (≈15× upper normal limit; reference: 10.6-19.4), and negative anti-TSH receptor antibodies at 1.10 UI/L (reference: <1.17). Thyroid scintigraphy revealed diffuse, homogeneous, and markedly increased uptake throughout an enlarged thyroid gland (Figure 1). Cervical ultrasonography confirmed a diffuse, hypervascular goiter without nodular lesions, consistent with GD.
Acquisition of a static anterior image centered on the cervical region, 20 minutes after injection of 5 mCi of 99 mTThyroid scintigraphy demonstrating an enlarged gland with diffuse, homogeneous, and markedly increased tracer uptake, consistent with Graves’ disease.
The patient was started on carbimazole at 40 mg/day. After six weeks of therapy, he developed signs of drug-induced hepatotoxicity, with cytolysis evidenced by aspartate aminotransferase (AST) at 208.3 U/L (≈4.6× normal) and alanine aminotransferase (ALT) at 254.8 U/L (≈5.6× normal), as well as cholestasis with alkaline phosphatase (ALP) at 628.1 U/L (≈5× normal) and gamma-glutamyl transferase (GGT) at 667.2 U/L (≈14.8× normal). In light of these abnormalities, carbimazole was discontinued. Viral hepatitis serologies were negative (Table 1).
Given the presence of persistent fever, laboratory testing revealed markedly elevated C-reactive protein at 116.8 mg/L, leukocytosis of 14,300/mm³, increased erythrocyte sedimentation rate, and elevated lactate dehydrogenase at 640 U/L. An etiological workup was undertaken: urine culture was sterile, blood cultures obtained during febrile spikes were negative, the Quantiferon test excluded latent tuberculosis infection, and serum protein electrophoresis confirmed an inflammatory profile.
In the context of suspected AOSD, alternative diagnoses were systematically ruled out. Rheumatoid factor, anti-cyclic citrullinated peptide antibodies, and antinuclear/cytoplasmic antibodies all tested negative.
Imaging investigations showed homogeneous hepatosplenomegaly on thoraco-abdominal computed tomography (CT) scan (Figure 2), while transthoracic echocardiography was unremarkable (Figure 3).
Thoracoabdominal CT showing homogeneous hepatosplenomegalyAxial contrast-enhanced abdominal CT demonstrating homogeneous enlargement of the liver and spleen (arrows).CT, Computed tomography
Transthoracic echocardiography showing normal cardiac morphology and functionParasternal long-axis transthoracic echocardiographic view showing normal cardiac chamber dimensions and wall thickness. Linear measurements are indicated.
In the absence of evidence for infectious or malignant disease, and given the constellation of clinical and biological findings, the diagnosis of AOSD was considered according to the Yamaguchi criteria [7]. Supporting this, serum ferritin was >1200 ng/mL, with glycosylated ferritin reduced to 13%.
The patient was started on corticosteroid therapy with prednisolone 60 mg/day, resulting in a favorable initial clinical and biological response.
The subsequent evolution of the patient was marked by alternating flares and remissions of both conditions. Due to recurrent hepatocellular injury, definitive management of GD with radioiodine therapy was proposed. The patient subsequently received 20 mCi of radioactive iodine.
Discussion
The coexistence of AOSD and GD has been previously documented. In Japan, Torigoe et al. (2011) described the case of a 50-year-old woman with AOSD and recurrent GD, raising the possibility of shared pathophysiological mechanisms [6]. In their report, the authors also referred to five additional cases of concurrent presentation (Table 2).
In 2014, Hu et al. reported another case of AOSD associated with thyroid dysfunction in a 43-year-old woman with preexisting GD, whose course was complicated by active AOSD [5]. The same study cited a similar observation previously published by Chen et al. [8].
These findings revived the debate on whether a pathophysiological link exists between the two diseases and highlighted the importance of reciprocal screening.
Although the pathogenesis of both AOSD and GD is complex and multifactorial, several overlapping features have been identified. From a genetic perspective, both conditions are associated with certain HLA-DRB1 alleles. Immunologically, a predominance of T-helper 1 (Th1)-mediated immune response, characterized by elevated levels of tumor necrosis factor-α (TNF-α), soluble TNF receptor 1, interleukin (IL)-6, and IL-18, plays a central role in AOSD pathogenesis.
IL-18, in particular, has been recognized as a key mediator within the inflammatory cascade, capable of inducing other cytokines such as IL-1β, which alters the tight junction integrity of human thyrocytes, along with IL-8, TNF-α, and interferon-γ (IFN-γ) [9].
Moreover, high serum levels of C-X-C motif chemokine ligand 10 (CXCL10), an IFN-γ-inducible chemokine, have been reported in both AOSD and GD patients, compared to healthy controls and other autoimmune disorders [10,11].
Conclusions
This case highlights the rare coexistence of AOSD and GD in a young patient and adds to the limited number of similar reports in the literature. The diagnosis was supported by compatible clinical, biological, and imaging findings, and by the exclusion of infectious, malignant, and other autoimmune causes. Although a shared immunoinflammatory background between these two conditions has been suggested, the exact relationship remains unclear. Further studies are needed to determine whether this association is coincidental or reflects common pathogenic pathways, and to clarify its potential diagnostic and therapeutic implications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thyroid dysfunction in rheumatoid arthritis: a controlled prospective survey Ann Rheum Dis Shiroky JB Cohen M Ballachey ML Neville C 454456521993832339810.1136/ard.52.6.454PMC 1005071 · doi ↗ · pubmed ↗
- 225 year follow-up of the Aland thyroid study of 1956. Thyroid status and incidence of rheumatoid arthritis Acta Endocrinol Suppl (Copenh) Wahlberg P Nyman D Carlsson SA 47522511983 https://pubmed.ncbi.nlm.nih.gov/6573099/6573099 · pubmed ↗
- 3Thyroid disorders in systemic lupus erythematosus Ann Rheum Dis Goh KL Wang F 579583451986374098210.1136/ard.45.7.579PMC 1001940 · doi ↗ · pubmed ↗
- 4Thyroid disease in Sjögren's syndrome Arthritis Rheum Karsh J Pavlidis N Weintraub BD Moutsopoulos HM 13261329231980 https://doi.org/10.1002/art.1780231118744797010.1002/art.1780231118 · doi ↗ · pubmed ↗
- 5Adult-onset Still's disease associated with thyroid dysfunction: case report and review of the literature Open Rheumatol J Hu Y Wang H Deng J 912820142506796410.2174/1874312901408010009 PMC 4110384 · doi ↗ · pubmed ↗
- 6Simultaneous relapse of Basedow's disease in a patient with adult-onset Still's disease (Article in Japenese)Nihon Rinsho Meneki Gakkai Kaishi Torigoe M Miyamura T Nakamura M 4264303420112204143110.2177/jsci.34.426 · doi ↗ · pubmed ↗
- 7Adult Still's disease: a multicenter survey of Japanese patients J Rheumatol Ohta A Yamaguchi M Tsunematsu T 10581063171990 https://pubmed.ncbi.nlm.nih.gov/2213780/2213780 · pubmed ↗
- 8Coexistence of adult-onset Still's disease and autoimmune hyperthyroidism in a patient who responded to corticosteroids and β-blocker Immunopharmacol Immunotoxicol Chen HS Yu KH Ho HH 6966993220102020162510.3109/08923971003677816 · doi ↗ · pubmed ↗