A Systematic Review Evaluating the Surgical Management of Cervical Spine Fractures in Patients With Ankylosing Spondylitis
Shahswar Arif, Zarina Brady, Reagan O'Kane, Ciaran Doherty, Christopher McKee, Jagdeesh Nijjher, Rakesh Dhokia, Nikolay Peev

TL;DR
This study compares surgical approaches for cervical spine fractures in ankylosing spondylitis patients, finding no significant difference in complications but a lower mortality rate with the combined approach.
Contribution
The study provides a systematic review comparing posterior-only and combined surgical approaches for cervical spine fractures in ankylosing spondylitis patients.
Findings
The posterior-only approach had fewer intraoperative and postoperative complications compared to the combined approach, but differences were not statistically significant.
The combined approach showed a significantly lower mortality rate compared to the posterior-only approach.
Both surgical approaches have advantages and disadvantages, suggesting case-by-case decision-making is needed.
Abstract
Patients with ankylosing spondylitis (AS) are vulnerable to cervical spinal fractures despite minute trauma. As there is a lack of consensus on which surgical approach is the most efficacious in treating cervical spinal fractures in AS patients, we sought to compare the posterior-only and combined (anterior-posterior) approach regarding intraoperative and postoperative complications. This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (ID: CRD42024284877). Studies published up to May 20, 2025, were searched in PubMed, MEDLINE, and CENTRAL (Cochrane Central Register of Controlled Trials) with predetermined terms. Studies reporting outcomes, including intraoperative and postoperative complications and mortality rate, were evaluated. Included studies underwent a risk of bias assessment. Seventeen studies (one…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
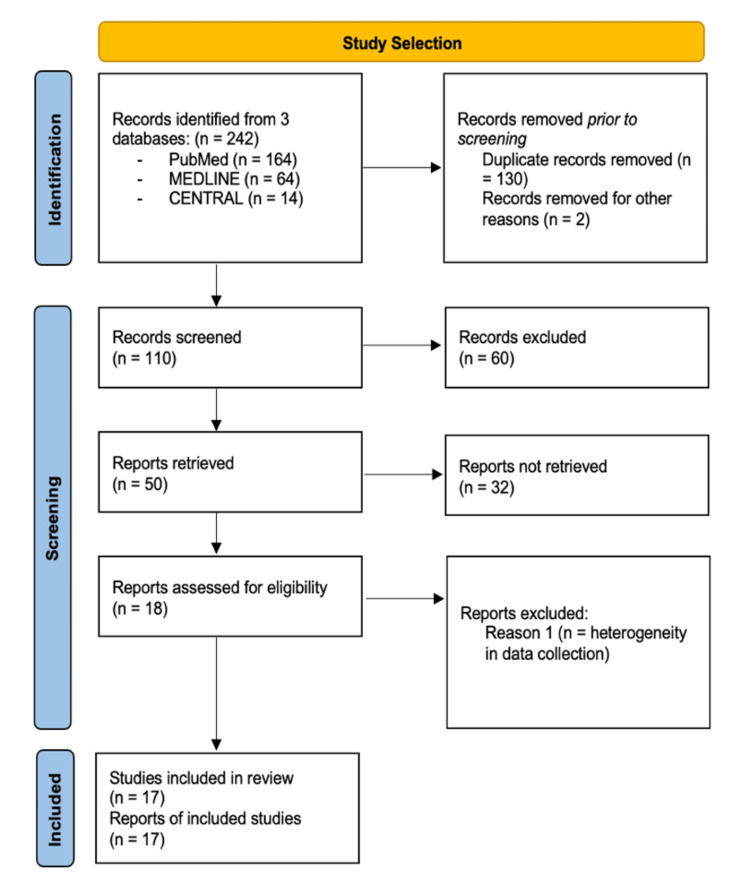 Figure 1
Figure 1| Study | Year | Bias due to confounding variable | Bias-participant selection | Bias in the classification of interventions | Bias due to deviation from the intended intervention | Bias due to missing data | Bias in measurement outcomes | Bias in the selection of reported unit | Overall bias |
| Alhashash et al. [ | 2023 | + | ? | + | + | + | + | + | + |
| Shetty et al. [ | 2023 | + | ? | + | + | ? | + | + | ? |
| Sharma et al. [ | 2022 | + | ? | + | + | ? | + | ? | ? |
| Tang et al. [ | 2022 | ? | ? | + | + | + | + | + | ? |
| Liu et al. [ | 2021 | + | ? | + | + | + | ? | + | + |
| Ren et al. [ | 2021 | + | ? | + | + | + | ? | ? | ? |
| Altun and Yuksel [ | 2016 | + | ? | + | + | + | + | ? | + |
| Lukasiewicz et al. [ | 2016 | + | ? | + | + | + | + | ? | + |
| Robinson et al. [ | 2015 | ? | ? | + | + | + | ? | ? | ? |
| Schiefer et al. [ | 2015 | ? | ? | + | + | x | + | ? | x |
| Robinson et al. [ | 2015 | ? | ? | + | + | + | + | + | ? |
| Mathews and Bolesta [ | 2013 | ? | ? | + | + | + | ? | + | ? |
| Kouyoumdjian et al. [ | 2012 | ? | ? | + | + | + | ? | + | ? |
| Lv et al. [ | 2009 | x | ! | + | + | + | ? | ? | x |
| Sapkas et al. [ | 2009 | + | ? | + | + | + | + | + | + |
| Taggard and Traynelis [ | 2000 | ? | ? | + | + | x | + | ! | x |
| Olerud et al. [ | 1996 | ? | ? | + | + | + | ? | + | ? |
| Characteristics | AS patients with spinal fracture cohort |
| Study design (n) | |
| Prospective | 1 |
| Retrospective | 16 |
| N | 858 |
| Average age (years) | 59.9 |
| Mechanism of injury, n (%) | |
| Major trauma (motor vehicle accidents, assaults/crush) | 43 (25%) |
| Falls | 173 (66%) |
| Fracture level, n (%) | |
| C1 | 2 (2.9%) |
| C2 | 5 (5.2%) |
| C4 | 3 (3.2%) |
| C5 | 4 (3.4%) |
| C6/C7 | 185 (50.6%) |
| C7 | 10 (8%) |
| C7/T1 | 18 (9%) |
| Fracture type, n (%) | |
| A | - |
| B1 | - |
| B2 | 19 (13%) |
| B3 | 60 (54%) |
| C | 35 (31.1%) |
| Preoperative neurological deficit, n (%) | 168 (77.7%) |
| Characteristics | Posterior-only approach | Combined (anterior-posterior) approach |
| Surgical details | ||
| EBL (ml) | 306.38 | 458.33 |
| Operation time (mins) | 161.11 | 213.67 |
| Intraoperative complications, n (%) | ||
| Epidural haematoma | 2 (5.8%) | 1 (20%) |
| Durotomy | 2 (3.7%) | 1 (10%) |
| Screw loosening/loss of fixation | 1 (2.8%) | 3 (12.5%) |
| Postoperative complications, n (%) | ||
| Wound infection | 5 (12%) | 2 (8.3%) |
| Pulmonary complications | 4 (7.7%) | 3 (30%) |
| Dysphagia | 0 (0%) | 4 (27.5%) |
| Pneumonia | 6 (8.8%) | 3 (30%) |
| Urinary tract infection | 0 (0%) | 2 (20%) |
| DVT | 2 (16.7%) | 2 (20%) |
| Mortality rate, n (%) | 13 (24.5%) | 3 (9.2%) |
| Characteristics | Posterior-only approach | Combined approach | P-value |
| Intraoperative complications, n (%) | 4 (4.8%) | 2 (15%) | >0.05 |
| Postoperative complications, n (%) | 17 (7.5%) | 16 (22.6%) | >0.05 |
| Instrumented-related complications, n (%) | 1 (2.8%) | 3 (12.5%) | >0.05 |
| Mortality rate, n (%) | 13 (24.5%) | 3 (9.2%) | >0.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpondyloarthritis Studies and Treatments · Spinal Fractures and Fixation Techniques · Scoliosis diagnosis and treatment
Introduction and background
Ankylosing spondylitis (AS) is an autoimmune condition involving the spine, sacroiliac joints, and entheses [1]. The cervical spine, followed by the thoracolumbar region, is the most frequent spinal fracture site in AS patients [1,2]. There is often a delay in diagnosis, as the symptoms are not very overt [1-3]. Standard imaging is not optimal for noticing the osteoporosis-linked shearing fractures, particularly in the spine. Even with the slightest fracture suspicion, computed tomography (CT) and magnetic resonance imaging (MRI) should be recommended [4-6]. Neurological deficit can occur at the time of the fracture or upon its displacement, specifically in hyperextension injuries [7]. Surgery is indicated in cases with unstable fractures and severe neurological deficit [5,6,8]. The goal is to prevent complications linked with nonoperative measures [9]. There is still no consensus on the best approach to treat AS-linked cervical spinal fractures. Thus, we performed a systematic review of randomized controlled trials and prospective and retrospective studies to evaluate the postoperative neurological function and perioperative complications in surgically treated AS patients with cervical spinal fractures.
Review
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (ID: CRD42024284877). The search strategy in the published protocol included studies reporting neurological evaluation and perioperative complication rate comparing surgical approaches (posterior-only or combined approach) in AS patients with cervical spinal fractures. Inclusion criteria regarding the study design included randomized controlled trials (RCTs), retrospective studies, and prospective studies. In addition, only studies that evaluated AS patients with cervical spine fractures were considered for inclusion. For quantitative analysis, intraoperative complications such as epidural haematoma and incidental durotomy were evaluated, instrument-related complications such as screw loosening/loss of fixation were evaluated, and postoperative complications such as dysphagia, pneumonia, urinary tract infection, and deep vein thrombosis were included. A detailed search of studies published on PubMed, MEDLINE, and CENTRAL (Cochrane Central Register of Controlled Trials) up to May 20, 2025, was carried out. The search strategy included keywords ("Ankylosing Spondylitis", "Cervical Spine Fractures", "Peri-operative Complications", "Spinal Fractures") to identify potential articles. Figure 1 illustrates the study selection process using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart [10].
PRISMA flowchart for study selectionPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; CENTRAL: Cochrane Central Register of Controlled Trials
The search strategy was compiled in consultation with neurosurgical and orthopaedic surgeons, and no language or publication date restrictions were used. Titles as well as summaries of all studies underwent evaluation by authors independently, followed by the full-text screening of any studies that warranted inclusion. Conflicts were resolved by two senior co-authors (RD, NP). Authors used a standardized data extraction form to collate the study design, publication year, gender and age of patients, body mass index, mechanism of injury (major trauma/falls), fracture level (cervical), surgical approach (posterior-only, combined), intraoperative complications (epidural haematoma, iatrogenic durotomy), instrument-related complications (screw loosening/loss of fixation), postoperative complications (dysphagia, pneumonia, urinary tract infection, deep vein thrombosis), length of hospital stay, and mortality rate. Studies published in duplicate were only included once. All included studies underwent a risk of bias assessment, shown in Table 1 [9,11-26]. Studies that did not include the anterior or posterior or combined approaches were not included; studies that were not published in English or case reports were not included either.
Results
The preliminary search resulted in 242 original articles after the removal of duplicates, of which 110 articles were deemed potentially eligible. A total of 17 studies were included in the final quantitative analyses. Characteristics of the included studies are summarized in Table 2. The relevant 17 studies published between 1983 and 2023 were included.
Primary Outcomes
For the posterior-only cohort, the overall intraoperative complication rate was four (4.8%), with incidental durotomy and epidural haematoma occurring in two (3.7%) and two (5.8%) patients, respectively. In the combined (anterior-posterior) approach group, the overall intraoperative complication rate was two (15%), with incidental durotomy and epidural haematoma occurring in one (10%) and one (20%) patient, respectively (Table 3). The instrument-related complication rate was lower in the posterior-only cohort (1, 2.8%) than in the combined approach group (3, 12.5%) (Table 4). Postoperative complication rate was higher in the combined approach cohort (16, 22.6%) in comparison to the posterior-only approach group (17, 7.5%). Frequently reported postoperative complications for the combined and posterior-only approaches were pneumonia (3 (30%) vs. 6 (8.8%)), wound infection (2 (8.3%) vs. 5 (12%)), and pulmonary complications (3 (30%) vs. 4 (7.7%)) (Table 3). As regards the mortality rate, the posterior-only cohort had a higher mortality rate (13, 24.5%) in comparison to the combined approach cohort (3, 9.2%) (p<0.05) (Table 4).
Discussion
This systematic review evaluated the posterior-only and combined (anterior-posterior) approaches to determine a conclusion on which approach is efficacious in treating spinal fractures in AS patients. With the increasing elderly population, the number of geriatric patients is also increasing. Patients aged above 80 years were reported to be an independent risk factor for postoperative complications [27,28].
In our systematic review, low-energy trauma was the main mechanism of spinal fractures in AS patients. This matches the trend observed in literature, in which falls were noted to be the most frequent injury mechanism [29]. Research has shown that AS is a contributing factor in low-energy traumatic spinal fractures [20]. The positive sagittal alignment itself is an independent risk factor for spinal fractures [30]. The majority of acute fractures of the spine in AS cohorts occur in the cervical region, especially at C6-C7 [31].
Posterior-only and combined approaches are the most frequently used techniques for subaxial spinal fractures [31-35]. Potential limitations regarding the posterior-only approach relate to posterior screw placement owing to the absence of osteological landmarks in AS [36]. Another drawback of the posterior-only approach in AS cases relates to unstable cervical spine fractures and deformities linked to the positioning of the patient. The majority of patients have a degree of kyphotic alignment with an extension-type injury. Surgeons could take into account placing the patient on a frame that allows controlled kyphosis, such as through a Wilson-type frame [7]. The combined approach gives the most construct stability [37,38].
AS patients are more susceptible to developing a neurological function deficit after spinal trauma. The literature reported neurological deficit in half of the patients [25]. Such results showed that cervical fractures in AS patients can result in severe neurological function deficit. Moreover, AS patients are susceptible to secondary neurological function deficit owing to unstable fracture configuration between fused segments [39]. Luksanapruksa et al. reported improvement in neurological function (American Spinal Injury Association (ASIA) scale) in the majority of patients in posterior-only and combined (anterior-posterior) approaches; however, two patients from the posterior-only cohort had worsening of neurological function, while no patients from the combined group worsened neurologically [40]. Literature evaluating direct comparative analyses between posterior-only and combined approaches (in such cases) is scarce [41]. The most common intraoperative complication recorded in our review was epidural haematoma. The most common instrument-related complications included were screw loosening and loss of fixation. Olerud et al. reported that fixation loss was significantly more common in one-side-only surgical approaches [26]. Due to the weakened spinal anatomy and the fact that the spine only moves at the site of the fracture, a single-side-only fixation will not withstand the stress forces focused on the internal fixation. In terms of postoperative complication rate, the posterior-only approach yielded a lower complication rate. In our review, pneumonia was one of the most commonly reported postoperative complications in both approaches [42]. An increased incidence of pulmonary diseases is observed in AS cases owing to the restrictive ankylosis of the thoracic cage [43]. Such results can help surgeons in choosing surgical approaches in AS patients with spinal fractures [42]. Momeni et al. reported that upper lobe fibrosis, interstitial pulmonary disease, and sleep apnoea are linked to AS. As the respiratory system is at a higher risk in severe AS cases, cardiopulmonary function should be taken into account when managing spinal fractures in AS patients [44].
In our systematic review, the combined approach yielded a lower mortality rate in comparison to the posterior-only approach. The risk of mortality is higher in AS patients with cervical fractures in comparison to thoracolumbar fractures. Death frequently occurred in patients with postoperative complications, especially when the pulmonary function was compromised, such as pneumonia, pulmonary fibrosis, pulmonary embolism, and acute respiratory distress syndrome [41,45].
The strengths of this systematic review are as follows: no systematic review directly evaluates surgical approaches regarding perioperative neurological improvement and perioperative complications, and the systematic review is timely and will be valuable to surgeons choosing approaches when treating cervical spinal fractures in AS patients. The limitations of this review are the following: the number of studies included is limited. There is an absence of standardized surgical procedures for the treatment of cervical fractures in AS patients. Another drawback of this relates to the wide range of scores relating to the neurological function evaluation, so several studies had to be excluded from quantitative analysis. No randomized controlled trials have been conducted on this study, resulting in a low quality of the included studies.
Conclusions
The results of this systematic review suggest that both combined and posterior-only approaches have advantages and disadvantages and approach selection should be done on a case-by-case basis. Surgical intervention involving open reduction and internal fixation prevents worsening and improves neurological function in AS patients with cervical fractures. The combined approach yielded superior postoperative neurological outcomes as well as mortality rates in comparison to the posterior-only approach. However, the posterior-only approach yields superior outcomes with regard to intraoperative, instrument-related, and postoperative complications. Future randomized controlled trials evaluating different surgical approaches reporting objective measures are needed to form a consensus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Association of immune function with bone mineral density and biochemical markers of bone turnover in patients with anklylosing spondylitis Int J Clin Pract Yilmaz N Pence S Kepekçi Y Geyikli I Ozaslan J 681685572003 https://pubmed.ncbi.nlm.nih.gov/14627178/14627178 · pubmed ↗
- 2Cervical spine involvement in ankylosing spondylitis Clin Rheumatol El Maghraoui A Bensabbah R Bahiri R Bezza A Guedira N Hajjaj-Hassouni N 94982220031274067110.1007/s 10067-002-0681-2 · doi ↗ · pubmed ↗
- 3HLA-B 27-restricted T cells from patients with ankylosing spondylitis recognize peptides from B*2705 that are similar to bacteria-derived peptides Clin Exp Immunol Frauendorf E von Goessel H May E Märker-Hermann E 35135913420031461679810.1046/j.1365-2249.2003.02289.x PMC 1808853 · doi ↗ · pubmed ↗
- 4Ankylosing spondylitis Lancet Braun J Sieper J 1379139036920071744882510.1016/S 0140-6736(07)60635-7 · doi ↗ · pubmed ↗
- 5Spinal fractures in ankylosing spondylitis: patterns, management, and complications in the United States - analysis of latest nationwide inpatient sample data Neurospine Kandregula S Birk HS Savardekar A 7867971820213500033310.14245/ns.2142712.356PMC 8752689 · doi ↗ · pubmed ↗
- 6Occupational disease 2108. Degenerative changes of the cervical spine as a causality criterion in the assessment of discogenic diseases according to Be KV 2108 [Article in German]Unfallchirurg Hartwig E Schultheiss M Krämer S Ebert V Kinzl L Kramer M 30631210620031271985110.1007/s 00113-002-0561-x · doi ↗ · pubmed ↗
- 7Management of cervical spine injuries in patients with ankylosing spondylitis J Neurosurg Detwiler KN Loftus CM Godersky JC Menezes AH 210215721990229591810.3171/jns.1990.72.2.0210 · doi ↗ · pubmed ↗
- 8Errors of level in spinal surgery: an evidence-based systematic review J Bone Joint Surg Br Longo UG Loppini M Romeo G Maffulli N Denaro V 154615509420122310963710.1302/0301-620X.94B 11.29553 · doi ↗ · pubmed ↗