Staphylococcal early-onset prosthetic valve endocarditis: a condition bound for surgery
Antonio de Santis, Eduardo Cukierkorn, Flavio Tarasoutchi, Roney Orismar Sampaio, Tshimbalanga Merite, Milena R. Paixão, Carlos Manuel A. Brandão, Elinthon T. Veronese, Francisco Monteiro de Almeida Magalhães, Tarso A. D. Accorsi, Guilherme S. Spina, Tania Mara Varejão Strabelli

TL;DR
Staphylococcal early-onset prosthetic valve endocarditis has high in-hospital mortality, especially for Staphylococcus aureus cases, and surgery improves survival.
Contribution
Identifies SAPVE as an independent risk factor for mortality and highlights the critical role of prosthetic valve replacement in improving survival.
Findings
Staphylococcus aureus prosthetic valve endocarditis (SAPVE) had significantly higher in-hospital mortality (80%) compared to CoNS PVE (43%).
Prosthetic valve replacement was associated with improved in-hospital survival (odds ratio 0.2).
SAPVE was identified as an independent risk factor for in-hospital mortality (odds ratio 10.2).
Abstract
Early-onset prosthetic valve endocarditis (EO-PVE) is linked to poor in-hospital outcomes. Staphylococcus spp. poses a significant concern due to its higher mortality rates compared to other major infectious agents. Provide a more detailed, comprehensive evaluation of the clinical characteristics and in-hospital mortality predictors related to staphylococcal EO-PVE. This observational, retrospective, single-center study was conducted at a tertiary hospital in Brazil from 1997 to 2019, spanning a 22-year period. A total of 105 consecutive cases of left-heart staphylococcal EO-PVE were analyzed. There was a predominance of coagulase-negative staphylococci prosthetic valve endocarditis (CoNS PVE) over Staphylococcus aureus prosthetic valve endocarditis (SAPVE) (76% and 24%, respectively). Prosthetic valve replacement for EO-PVE treatment was performed in 73% of cases. In-hospital…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
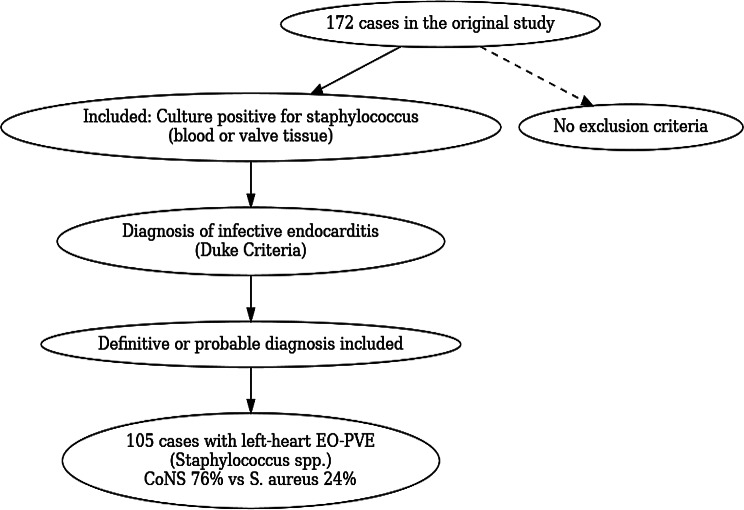 Figure 1
Figure 1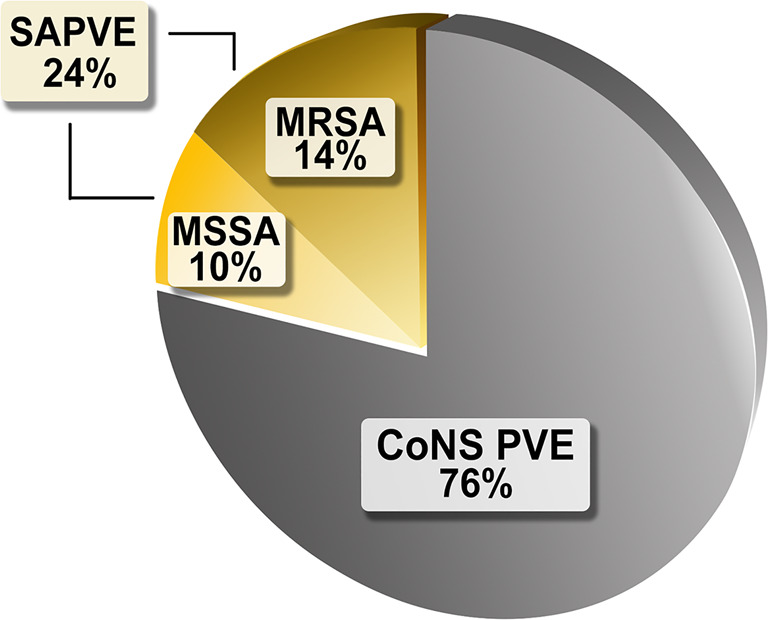 Figure 2
Figure 2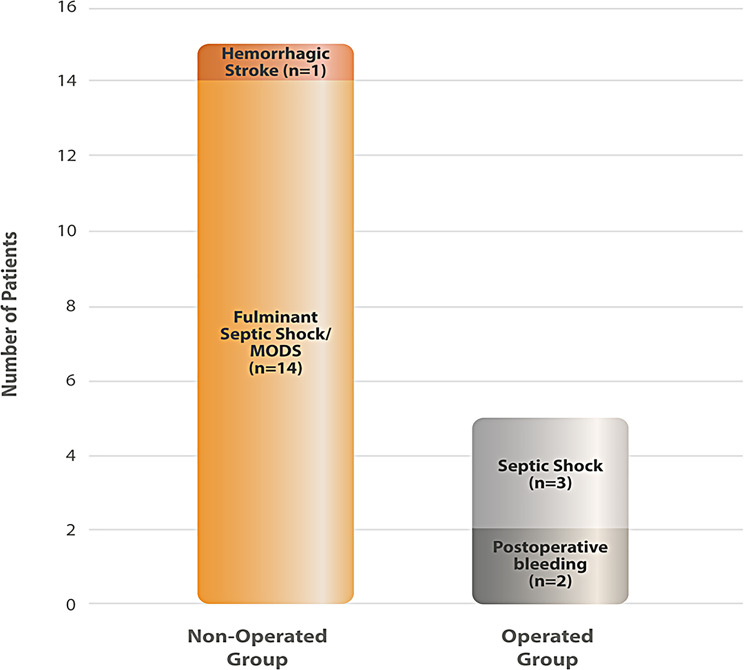 Figure 3
Figure 3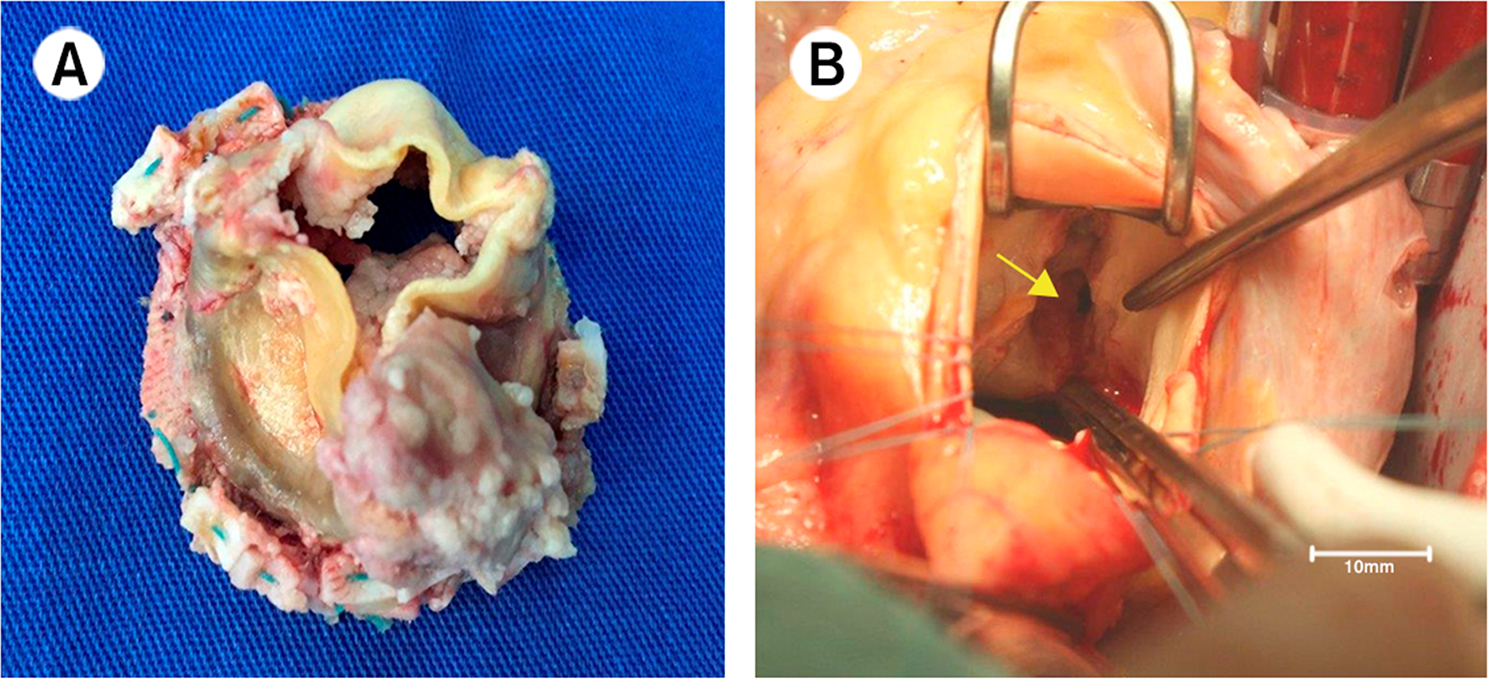 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Antimicrobial Resistance in Staphylococcus · Surgical site infection prevention
Introduction
Prosthetic valve endocarditis (PVE) occurs in 3–6% of patients within five years of valve replacement surgery and carries significant morbidity and in-hospital mortality [1, 2]. Early-onset prosthetic valve endocarditis (EO-PVE) is defined as infection diagnosed within one year after heart valve surgery [3]. The clinical use of this classification is justified by the distinct microbiological profile of this period, characterized by a higher prevalence of virulent hospital-acquired pathogens. Among these, Staphylococcus aureus is particularly notable for its aggressiveness, with mortality rates of up to 48.5% and frequent embolic complications affecting the central nervous system (CNS), spleen, kidneys, and peripheral arteries [4]. Previous studies demonstrate that S. aureus prosthetic infective endocarditis (SAPVE) is an independent predictor of in-hospital mortality [5]
Due to the complexity of decision-making in EO-PVE—often influenced by the severity of the clinical state and complications such as CNS embolism—management must be undertaken by a dedicated endocarditis team. Regarding therapy, most recommendations derive from relatively small retrospective studies, which consistently suggest higher mortality rates in non-operated patients. This study, therefore, aims to describe the clinical characteristics, in-hospital mortality predictors, and the role of surgical treatment in staphylococcal EO-PVE. The study population comprises exclusively left-sided EO-PVE, given its clinical significance and frequency, since tricuspid and pulmonary prostheses are uncommon.
Methods
The current study is a sub-analysis of a historical cohort published by Siciliano et al. [3], which evaluated prosthetic valve endocarditis (PVE) at the Heart Institute (InCor), University of São Paulo Medical School, Brazil. The original study included patients diagnosed between 1997 and 2014, representing more than a decade of experience with PVE during the first postoperative year. Its primary objective was to assess the annual incidence of PVE within the first year after valve surgery and its microbiological profile. Diagnosis was established according to the Modified Duke Criteria (2000), with microorganisms identified through blood cultures and cultures of excised valve tissue. In contrast to the original study, the present analysis focused exclusively on staphylococcal early-onset PVE (EO-PVE), given its virulence and distinct clinical importance (Fig. 1). Only patients with culture-positive staphylococcal endocarditis were includedFig. 1Flowchart of inclusion criteria. Of the 172 cases from the original study, 105 fulfilled criteria for staphylococcal-related early-onset prosthetic valve endocarditis (EO-PVE), with distribution according to staphylococcus aureus and coagulase-negative staphylococci (CoNS)
For the present analysis, only patients with culture-positive staphylococcal endocarditis were included, given the virulence and distinct clinical importance of this group of microorganisms (Fig. 1). A total of 105 patients met the selection criteria: 103 fulfilled the definition of definite endocarditis, and two were classified as possible endocarditis. Among the included cases, coagulase-negative staphylococci (CoNS) were predominant (76%), while Staphylococcus aureus accounted for 24%. According to the Modified Duke Criteria, definite endocarditis requires either two major criteria, one major plus three minor criteria, or five minor criteria. Possible endocarditis was defined by the presence of one major plus one minor criterion or three minor criteria. For this analysis, both definite and probable cases were included. To ensure a homogeneous population, only left-sided prosthetic valve endocarditis was analyzed, given its higher prevalence and predominance in the cohort. The primary objective of this sub-analysis was to identify variables associated with poor prognosis in patients with staphylococcal PVE.
All surgical indications were determined by a dedicated multidisciplinary endocarditis team, composed of clinical cardiologists, cardiac surgeons, infectious disease specialists, intensive care physicians, and emergency physicians.
The primary outcome was in-hospital mortality. Demographic information, type of valve prosthesis (mechanical or biological), laboratory findings, microbiological profile, echocardiographic characteristics, clinical features, and data on prosthetic valve replacement surgery were also collected. For the multivariate model, only variables with statistical significance in the univariate analysis were included.
The available clinical and surgical information was limited to the original study database, which did not include details on previous sternotomies, operative time, or perioperative complications. Nevertheless, it was possible to calculate the pre-surgical Risk-E score (Risk Score for Cardiac Surgery in Active Infective Endocarditis) in 34 patients, providing valuable prognostic information despite these constraints. The results are presented in Table 1.Table 1. Demographic dataAll patients(n = 105)Mean age (years)51.3 ± 16.4Male sex67 (63%)In-hospital mortality52 (49%)Exclusive aortic endocarditis61 (58%)Exclusive mitral endocarditis39 (37.2%)Peri-annular abscess34 (32%)Aorto-cavitary fistula3 (2.8%)MSSA10 (9.5%)MRSA15 (14.2%)CoNS80 (76.1%)Severe Heart Failure related to prosthetic valve dysfunction (NYHA III/IV)22 (21%)Systemic embolism19 (18%)Median time from valve replacement surgery to diagnosis of PVE (in days)44 (25–93)Vegetation70 (66.6%)Biologic prosthetic valve98 (93.3%)Combined mitral and aortic valve endocarditis5 (4.8%)Prosthetic valve replacement77 (73%)Definitive Duke criteria103 (98%)Median time from PVE diagnosis to prosthetic valve replacement (in days)6 (3–12)Data are expressed as mean ± standard deviation, median, and interquartile range or number (%). MSSA: methicillin-sensitive Staphylococcus aureus; MRSA: methicillin-resistant Staphylococcus aureus; CoNS PVE: Coagulase-Negative Staphylococci prosthetic valve endocarditis; NYHA: New York Heart Association; PVE: Prosthetic valve endocarditis
The primary indications for prosthetic valve replacement were severe heart failure related to prosthetic dysfunction, peri-annular abscess or aorto-cavitary fistulas, large mobile vegetations with systemic embolization ( > 10 mm), and persistent sepsis despite properly guided antibiotic therapy for more than 5–7 days [2, 6, 7]. Owing to the historical design of the study, surgical indications were based on the contemporary guidelines available at the time. A comparative discussion with the most recent ESC 2023 guidelines—classifying indications into heart failure, uncontrolled infection, and high risk of embolism or established embolism—has been added to the Discussion section. The local ethics committee approved the present study.
Statistical analysis
All statistical analyses were performed with SPSS 21.0 statistical package (SPSS, Chicago, IL, USA). The distribution of numerical variables was assessed using the Kolmogorov–Smirnov test. Variables with a normal distribution are expressed as mean ± standard deviation, whereas variables with a non-normal distribution are presented as median and interquartile range (IQR). Qualitative variables are reported as numbers and percentages. In univariate analysis, comparisons between groups were made using the Student’s t-test or ANOVA for normally distributed variables, and the Mann–Whitney U or Kruskal–Wallis test for non-normally distributed variables, as appropriate. Categorical variables were compared using the chi-square test. For multivariate analysis, logistic regression analysis was used to predict the risk of in-hospital mortality. Values of p < 0.05 were considered statistically significant.
Results
Among these patients, we found 105 cases with left-heart EO-PVE due to Staphylococcus spp., with a predominance of Coagulase-Negative Staphylococci (CoNS) over Staphylococcus aureus (76% versus 24%, respectively).
The final population consisted of 105 patients (mean age 51.3 ± 16.4 years, with 63% male sex) with left-heart Staphylococcal endocarditis. The median time from the previous valve replacement surgery to the PVE diagnosis was 44 days (25–93). There was a predominance of CoNS PVE (n = 80, 76%) over SAPVE (n = 25, 24%; 60% methicillin-resistant Staphylococcus aureus [MRSA], 40% methicillin-sensitive Staphylococcus aureus [MSSA]), as represented in Fig. 2. With the present data, the team was unable to determine the different types of CONS.Fig. 2. Etiologic distribution of staphylococcal early-onset prosthetic valve endocarditis. CoNS PVE: coagulase-negative staphylococci prosthetic valve endocarditis; MSSA: methicillin-sensitive staphylococcus aureus; MRSA: methicillin-resistant staphylococcus aureus; SAPVE: staphylococcus aureus prosthetic valve endocarditis
Regarding the Duke criteria, 98% of the study population had definitive criteria. Prosthetic valve replacement for PVE treatment was performed in 73% of the patients, and the overall in-hospital mortality was 49%. The main complications were peri-annular abscess (32%); severe heart failure - New York Heart Association (NYHA) functional classification III/IV- related to prosthetic dysfunction (21%); systemic embolization (18%), and aorto-cavitary fistulas (3%). (Table 2). In comparison with CoNS PVE, SAPVE was associated with a higher in-hospital mortality (80% versus 43%, p < 0.001) and a trend towards earlier clinical presentation and diagnosis (median time from valve replacement to the PVE diagnosis: 33 days [18–94] versus 51.5 days [25.7–91.5], p = 0.05). However, there was a higher rate of prosthetic valve replacement for endocarditis treatment in CoNS PVE compared to SAPVE (83% versus 40%, p < 0.001, respectively) (Table 3). Only 5.7% (6/105) of patients were discharged from the hospital without surgical treatment.Table 2. Comparison of demographic data between SAPVE and CoNS PVEAll patients(n = 105)Risk E Group(n = 34)p-valueMean age (years)51.3 ± 16.457.2 ± 15.30.064Male sex67 (63.8%)21 (61.8%)0.992In-hospital mortality52 (49.5%)16 (47.1%)0.958Exclusive aortic endocarditis66 (62.9%)24 (70.6%)0.539Exclusive mitral endocarditis44 (41.9%)12 (35.3%)0.630Peri-annular abscess6 (5.7%)3 (8.8%)0.811Aorto-cavitary fistula34 (32.4%)15 (44.1%)0.299MSSA3 (2.9%)1 (2.9%)1.000MRSA70 (66.7%)25 (73.5%)0.592CoNS19 (18.1%)6 (17.6%)1.000Severe Heart Failure related to prosthetic valve dysfunction (NYHA III/IV)10 (9.5%)4 (11.8%)0.960Systemic embolism15 (14.3%)2 (5.9%)0.318Median time from valve replacement surgery to diagnosis of PVE (in days)80 (76.2%)28 (82.4%)0.608Vegetation25 (23.8%)6 (17.6%)0.608Comparison between the overall cohort (n = 105) and the Risk-E subgroup (n = 34 patients with available perioperative data). No significant differences were observed between groups, supporting the representativeness of the Risk-E subgroup. Data are expressed as mean ± standard deviation, median (interquartile range), or number (%). Comparisons were performed using Student’s t test or Mann–Whitney U test for continuous variables, and chi-square or Fisher’s exact test for categorical variables, as appropriateTable 3Comparison of demographic data between SAPVE and CoNS PVEAll patients(n = 105)SAPVE(n = 25)CoNS PVE (n = 80)p-valueMean age (years)51.3 ± 16.455.3 ± 16.550 ± 16.30.16Male sex67 (63%)16510.98In-hospital mortality52 (49%)20 (80%)32 (43%)0.001Exclusive aortic endocarditis61 (58%)14470.73Exclusive mitralendocarditis39 (37%)10290.80Peri-annular abscess34 (32%)10240.35Severe heart failure related to prosthetic valve dysfunction (NYHA III/IV)22 (21%)6160.5Systemic embolism19 (18%)3160.36Median time from valve replacement surgery to diagnosis of PVE (in days)44 (25–93)33 (18–94)51.5 (25.7–91.5)0.05Vegetation70 (66.6%)17530.87Biologic prosthetic valve98 (93.3%)23750.75Prosthetic valve replacement77 (73%)10 (40%)67 (83%)0.001Definitive Duke criteria103 (98%)25 (100%)78 (97%)0.42Median time from PVE diagnosis to prosthetic valve replacement (in days)6 (3–12)9 (5.2 -12,5)6 (3–11)0.35Data are expressed as mean ± standard deviation, median, and interquartile range or number (%). SAPVE: Staphylococcus aureus prosthetic valve endocarditis; CoNS PVE: Coagulase-Negative Staphylococci prosthetic valve endocarditis; NYHA: New York Heart Association; PVE: Prosthetic valve endocarditis
In the SAPVE group, all patients who did not undergo prosthetic valve replacement died (n = 15). Despite surgical indications, 14 of these patients (93.3%) developed fulminant septic shock within 24 hours of hospital admission, leaving insufficient time for surgical planning, as illustrated in Fig. 3. Among those who underwent surgery, five patients died due to postoperative complications.Fig. 3. Histogram of death causes related to staphylococcus aureus prosthetic valve endocarditis (n = 20). In the non-operated group (n = 15), the major cause of death was fulminant septic shock with multiple organ dysfunction syndrome (MODS). In the operated group (n = 5), deaths were primarily related to postoperative septic shock and bleeding
On univariate analysis, significant risk factors for in-hospital mortality included older age (p < 0.001), aortic prosthetic endocarditis (p < 0.001), periannular abscess (p = 0.002), SAPVE (p < 0.001), NYHA functional class III/IV (p = 0.02), previous combined coronary artery bypass-grafting (CABG) with valve replacement surgery (p = 0.02), left ventricular dysfunction (p < 0.001), leukocytosis (p = 0.02) and higher C-reactive protein levels (p = 0.006), as presented in Table 4. Additionally, prosthetic valve replacement was significantly associated with improved in-hospital survival (p < 0.001). The median time from PVE diagnosis to prosthetic valve replacement in the surgical group (n = 77) was 6 days (3–12), with no statistically significant difference between the deceased and alive groups.Table 4. Univariate analysis of in-hospital mortality in staphylococcal PVEAlive(n = 53)Dead(n = 52)p-valueAge > 60 (years)8 (15%)25 (48%) < 0.001Male sex33 (62.2%)34 (65.3%)0.73Exclusive aortic endocarditis25(47.1%)41 (78.8%) < 0.001Previous combined valve replacement surgery with myocardial revascularization3 (5.6%)11 (21.1%)0.02Peri-annular abscess10 (18.8%)24 (46.1%)0.002SAPVE5 (9.4%)20 (38.4%) < 0.001Severe heart failure related to prosthetic valve dysfunction (NYHA III/IV)19 (35.8%)26 (50%)0.02Systemic embolism7 (13.2%)12 (23%)0.18Median time from valve replacement surgery to diagnosis of PVE (in days)35 (22–83)48 (29.7–99.2)0.27Vegetation34 (64.1%)36 (69.2%)0.58Biologic prosthetic valve49 (92.4%)49 (94.2%)0.71Prosthetic valve replacement for endocarditis treatment47 (88.6%)30 (57.6%) < 0.001Median time from PVE diagnosis to prosthetic valve replacement (in days)7 (5–14.5)5 (3–9)0.06LVEF (%)61.9 ± 11.450.6 ± 18.4 < 0.001Hemoglobin (mg/dL)10.7 ± 1.9610.3 ± 1.850.33Leukocytes count (x10^3^ cells/mm^3^)13 ± 6.1716.2 ± 6.90.02Platelet count (x10^3^ cells/mm3)189.4 ± 81.2153.9 ± 92.80.06C-reactive protein (mg/L)96.2 ± 45.7183.5 ± 89.40.006Data are expressed as mean ± standard deviation, median, and interquartile range or number (%). Laboratory data presented in the table represent preoperative values. LVEF: Left ventricular ejection fraction, measured preoperatively.; SAPVE: Staphylococcus aureus prosthetic valve endocarditis; NYHA: New York Heart Association; PVE: Prosthetic valve endocarditis
Multivariate analysis showed that SAPVE was an independent risk factor for in-hospital mortality (odds ratio [OR] 10.2; p = 0.006; 95% CI [1.89–55.2]) and reinforced the potential protective effect of prosthetic valve replacement in staphylococcal EO-PVE (OR 0.2; p = 0.04; 95% CI [0.04–0.93]).
Discussion
Although rare, EO-PVE has a high potential for clinical complications and significant in-hospital mortality. From an etiopathogenic perspective, previous studies have demonstrated a predominance of staphylococcal infections in these scenarios, with a prevalence of nearly two-thirds of the cases [2, 8]. The present work was designed due to the clinical relevance and scarcity of previous studies focusing on this etiological subgroup of PVE. [4, 9, 10–13] While Streptococcus spp. and Enterococcus spp. are recognized as the second and third most frequent pathogens in infective endocarditis, the present study specifically aimed to evaluate staphylococcal EO-PVE, primarily because of its particularly aggressive clinical course.
Staphylococcal EO-PVE demonstrates a high virulence with an in-hospital mortality of 49% and high rates of clinical complications (peri-annular abscess-32%, heart failure-NYHA class III/IV-21%, systemic embolization-18%). Moreover, staphylococcal EO-PVE often requires a combination treatment strategy, including the association of proper antimicrobial therapy and valve replacement surgery (with a surgical rate of 73%).
Staphylococcal EO-PVE was diagnosed correctly, with 98% of the study population presenting definite endocarditis according to the Duke modified criteria. Vegetations were the most common echocardiographic feature (found in 66.6% of the cases). Fig. 4 represents multiple prosthetic vegetations in a staphylococcal EO-PVE (panel A) and an aorto-right ventricular fistula (panel B).Fig. 4. Staphylococcal early-onset prosthetic valve endocarditis examples. Panel A: multiple prosthetic vegetations with associated valvular dysfunction. Panel B: aorto-right ventricular fistula (yellow arrow)
Regarding the staphylococcal species, coagulase-negative strains were predominant (76%) compared to S. aureus (24%), with some notable clinical differences between them. SAPVE presented a higher fatality rate than CoNS PVE (80% versus 43%, p < 0.001) and a propensity to earlier clinical presentation (median time from previous valve replacement surgery to the PVE diagnosis of 33 days [18–94]). Conversely, SAPVE had a lower rate of prosthetic valve replacement than CoNS PVE (40% versus 83%, p < 0.001). Despite the inherent limitations of an observational study, the high mortality associated with SAPVE may be related to these observed lower rates of surgical treatment. The specific analysis of deaths in the SAPVE group demonstrated that from the 15 non-operated cases, 14 (93.3%) were due to fulminant septic shock leading to multiple organ dysfunction syndrome (MODS) in less than 24 hours. Thus, despite clinical indication, there was no proper time to perform the prosthetic valve replacement. In current guidelines, one of the most frequent indications for valve replacement in infective endocarditis is a clinical condition known as uncontrolled infection, defined by persistent sepsis despite proper antibiotic therapy for more than seven days [2, 6, 7]. Reinforcing the aggressiveness of SAPVE with early-onset sepsis, our study suggests that the time window for proper surgical intervention in these situations could be narrower than in other etiologies. The definition of the standard 7-day period for treatment failure appears to be overly compliant when considering such an inexorable progression. Early prosthetic valve replacement, before clinical irreversibility, may be crucial in obtaining favorable outcomes. In this sepsis scenario, antibiotic and intensive care for achieving an optimal clinical condition for surgical intervention seem to be unfeasible. In contrast, Sohail et al. identified a subgroup of patients with SAPVE in a previous retrospective and unicentric study, suggesting that exclusive clinical management could potentially prevent in-hospital mortality. This small group (4 patients) was characterized by age < 50 years with good clinical conditions and no cardiac complications or systemic embolization [9]. In our population, no cases with such a favorable outcome without surgical intervention existed.
Although the surgical indications in this study remain aligned with the 2023 ESC guidelines on infective endocarditis [14], the latter introduced some important modifications: the recommendation for urgent surgery (within 3–5 days) in cases of uncontrolled infection, and the need for discussion within the Endocarditis Team regarding early surgery in certain highly virulent microorganisms, including Staphylococcus aureus.
The univariate analysis showed 10 predictors of in-hospital mortality in this population. These predictors can be related to intrinsic features of the agent (S. aureus infections), clinical complications (peri-annular abscess, severe heart failure - NYHA class III/IV - related to prosthetic valve dysfunction), laboratorial features (high leukocyte count and C-reactive protein levels), patient profile (older age, previous combined valve replacement surgery with myocardial revascularization, left ventricular dysfunction) and aortic prostheses involvement. The lack of valve replacement surgery was associated with in-hospital mortality. Multivariate analysis reinforces the potential protective role of surgical intervention in staphylococcal EO-PVE, with an 80% relative reduction in in-hospital mortality (OR 0.2, p < 0.04). Moreover, multivariate analysis also indicates SAPVE as an independent and strong predictor of in-hospital mortality, emphasizing the high clinical aggressiveness of S. aureus compared to other staphylococcal species. As shown in Table 5.Table 5. Multivariate analysis of in-hospital mortality in staphylococcal PVEOR95% CIp-valueSAPVE10.21.89–55.20.006Prosthetic valve replacement0.20.04–0.930.04CI: Confidence interval; OR: Odds ratio; PVE: Prosthetic valve replacement; SAPVE: Staphylococcus aureus prosthetic valve endocarditis
Importantly, no statistically significant differences were observed between the Risk-E subgroup and the overall cohort in terms of demographic, clinical, microbiological, or echocardiographic variables. This finding supports the notion that the subgroup in which the Risk-E score could be calculated is representative of the entire population studied, thereby minimizing the risk of selection bias.
The present study has inherent limitations related to its unicentric and observational design. As a sub-analysis, the available clinical and surgical information was restricted to the original database. Consequently, potential biases may arise due to the lack of data regarding previous sternotomies, operative time, and perioperative complications. In addition, the absence of pre- and postoperative neurological status prevented us from evaluating the timing of surgery in patients with neurological complications. The lack of matching and adjustment for confounders, treatment selection biases, and the absence of randomization further compromise the intergroup comparative analysis. Nevertheless, the findings remain relevant given the relative scarcity of staphylococcal EO-PVE in clinical practice.
Conclusion
In conclusion, staphylococcal EO-PVE mortality is high, especially in SAPVE, where the majority of deaths were concentrated in non-operated patients. In this group, despite surgical indication, the early onset of septic shock and MODS does not allow immediate surgical intervention. Prosthetic valve replacement was significantly associated with in-hospital survival, and only 5.7% of the study population survived without valve replacement surgery.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Habib G, Lancellotti P, Antunes MJ, et al. Esc guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European society of cardiology (esc) endorsed by: European association for Cardio-thoracic surgery (eacts), the European association of nuclear medicine (EANM). Eur Heart J. 2015 2015;36(44):3075–12810.1093/eurheartj/ehv 31926320109 · doi ↗ · pubmed ↗