The impact of heart failure and bleeding risk on clinical outcomes in patients after percutaneous coronary intervention
Yoshiyuki Yazaki, Yoshihisa Nakagawa, Ken Kozuma, Raisuke Iijima, Anna Tsutsui, Yoshitaka Murakami, Masayuki Fukuzawa, Satoru Abe, Go Kato, Hidehiko Hara, Masato Nakamura

TL;DR
Heart failure and high bleeding risk increase the chances of poor outcomes after heart procedures like PCI, requiring more careful patient management.
Contribution
This study identifies the independent impact of heart failure and high bleeding risk on adverse outcomes after PCI using a large registry.
Findings
Heart failure patients had a 1.59 times higher risk of MACCE after PCI compared to non-HF patients.
Heart failure patients had a 1.74 times higher risk of major bleeding after PCI compared to non-HF patients.
High bleeding risk was strongly associated with both MACCE and bleeding, regardless of heart failure status.
Abstract
In recent years, revascularization for ischaemic heart failure (HF) has received increasing attention, and percutaneous coronary intervention (PCI) has been positioned as a high-risk procedure. However, the risk of major bleeding and major adverse cardiac and cerebrovascular events (MACCE) after PCI for patients with ischaemic HF has not been adequately evaluated. HF patients were selected from the PENDULUM (Platelet rEactivity in patieNts with DrUg eLUting stent and balancing risk of bleeding and ischaemic event) registry to compare the efficacy and safety of PCI in HF and non-HF patients. In addition, the impact of high bleeding risk (HBR) defined as BARC 3 and 5 was evaluated in these patients. A total of 6266 patients were included; 16% (n = 1006) had a history of HF at enrolment. Patients with HF showed a higher MACCE rate than those without HF (18.4% versus 7.7%; adjusted hazard…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
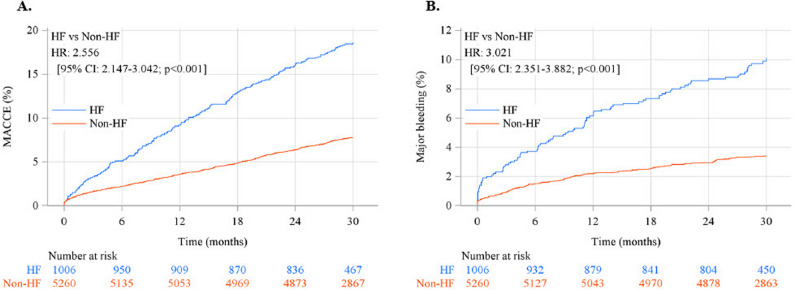 Figure 1
Figure 1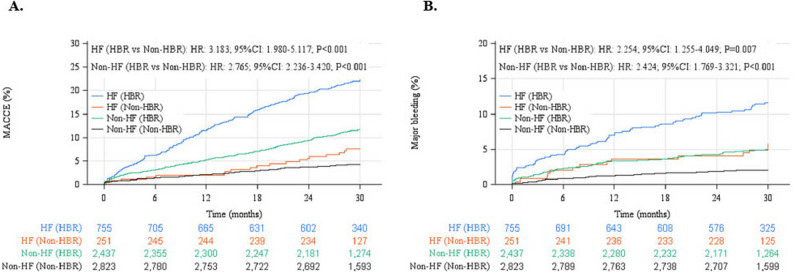 Figure 2
Figure 2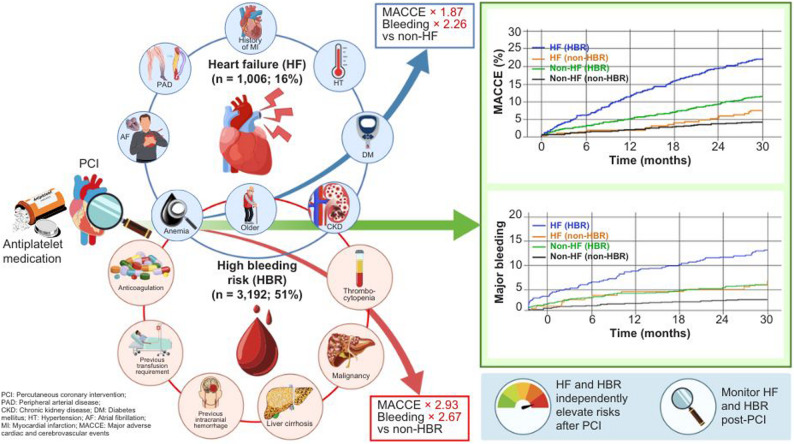 Figure 3
Figure 3- —Daiichi Sankyo Company, Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntiplatelet Therapy and Cardiovascular Diseases · Acute Myocardial Infarction Research · Mechanical Circulatory Support Devices
Introduction
In recent years, cardiovascular events after percutaneous coronary intervention (PCI) have been decreasing as a result of technological advances and the introduction of optimal medical treatment [1, 2]. However, with regard to medical management after PCI, a causal relationship between bleeding complications and subsequent increased cardiovascular mortality has been suggested, and strategies to prevent bleeding events are attracting attention [3, 4]. Therefore, the Academic Research Consortium – high bleeding risk (ARC-HBR) has strongly advocated for general bleeding risk assessment after PCI [5, 6]. Indeed, the PENDULUM (Platelet rEactivity in patieNts with DrUg eLUting stent and balancing risk of bleeding and ischaemic event) registry, a prospective, multicentre study of Japanese patients who underwent PCI, demonstrated that HBR patients who met the ARC-HBR criteria developed significantly more major bleeding [7, 8]. In addition, a post hoc analysis of this registry study reported that HBR patients had a 2.8-fold higher rate of thrombotic/ischaemic events than non-HBR patients [9]. These findings suggest that the management of HBR patients is complex, balancing bleeding and ischaemic events.
Coronary artery disease is one of the most common comorbidities of heart failure (HF), and ischaemic heart failure is associated with a high incidence of cardiovascular events and a poor prognosis [10, 11]. Though the role of revascularization for ischaemic heart failure remains debatable, the use of PCI in HF patients with reduced ejection fraction has increased markedly, and such patients are widely recognized as a high-risk group for cardiovascular events [12, 13]. In addition, although not included as a risk factor in ARC-HBR, HF patients may have a higher bleeding risk due to their many comorbidities and medications [5, 6]. Thus, post-PCI management of patients with HF has similar considerations to those of patients with HBR and should be considered thoughtfully. However, whether the presence of HBR has any prognostic impact on bleeding events or cardiovascular events in the high-risk group after PCI in patients with HF is unclear. Therefore, the purpose of this study was to evaluate the impact of HBR on cardiovascular and bleeding events in HF patients after PCI as a post hoc analysis of the PENDULUM registry [7, 8]. In addition, the presence of HF was also evaluated for its effect on the relationship between HBR and the incidence of cardiovascular and bleeding events.
Methods
Study population and design
Full inclusion and exclusion criteria for the PENDULUM registry have been reported previously [7]. In brief, patients aged 20 years and older at the time of informed consent, indicated for PCI with a second-generation drug-eluting stent, and administered antiplatelet drugs were enrolled. HF was defined as a history of HF at enrolment, and the diagnosis was made by the attending physician based on congestive symptoms and laboratory findings. Baseline left ventricular ejection fraction was recorded when available, but it was not an inclusion requirement for the PENDULUM registry. For the post hoc criterion analysis, enrolled patients were previously stratified into HBR and non-HBR groups according to ARC-HBR criteria [8]. In this study, platelet reactivity was assessed using P2Y_12_ reaction unit (PRU) values between 12 and 48 h after PCI, and patients were divided into two groups, the high platelet reactivity (HPR) and the non-HPR groups, with 208 as the cut-off value [14].
Clinical outcomes
The primary endpoints were major adverse cardiac and cerebrovascular events (MACCE; the standard clinical definition comprising all-cause death, non-fatal myocardial infarction (MI), non-fatal stroke, and stent thrombosis) and major bleeding, as defined by BARC (Bleeding Academic Research Consortium) type 3 or 5 bleeding after the index PCI [15]. The secondary endpoints were the individual components of MACCE.
Statistical analysis
Baseline characteristics are described by frequencies and percentages for categorical variables and mean and standard deviation (SD) values for continuous variables. Fisher’s exact test was used for the comparison of categorical variables, and Student’s t-test was used to compare continuous variables. Cumulative incidence rates among comparison groups were calculated, and Kaplan-Meier curves and Cox proportional hazards models were used for the group comparison.
Two types of multivariate Cox proportional hazards models were used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). In the first Cox model, factors associated with MACCE and major bleeding events in patients with or without HF were examined. To adjust for confounders, the following clinically relevant factors were selected as in previous study [3, 7] : sex, age, body weight, diabetes mellitus, ACS (acute coronary syndrome)/non-ACS, presence of peripheral arterial disease (PAD), chronic kidney disease, anaemia, and history of stroke or cerebral haemorrhage for MACCE; and sex, body weight, ACS/non-ACS, presence of PAD, chronic kidney disease, anaemia, malignant tumour, and anticoagulation at discharge for major bleeding events. In the second Cox model, the relationship between HF/HBR and outcomes was assessed by HRs with 95% CIs based on multivariate Cox proportional hazards models. In the model, factors associated with MACCE and major bleeding events in patients with or without HF and HBR, and the interaction of HF and HBR, were examined. Because HBR was included in this model, variables used for HBR evaluation were not included. Thus, the following clinically relevant factors were selected to adjust for confounding: sex, diabetes mellitus, ACS/non-ACS, and presence of PAD for MACCE; and sex, ACS/non-ACS, and presence of PAD for major bleeding events.
All statistical analyses were performed using SAS, version 9.4 (SAS Institute, Cary, NC, USA). All tests were two-sided, and P = 0.05 was considered significant.
Results
Patient characteristics
A total of 6266 patients were included in this post hoc study, of whom 1006 had a history of HF (755 in the HBR group and 251 in the non-HBR group). Demographically, patients with HF were significantly more likely to be older and have diabetes mellitus, hypertension, a history of myocardial infarction, PAD, and atrial fibrillation (Table 1). Concerning laboratory values, patients with HF were significantly more likely to have lower haemoglobin, estimated glomerular filtration rates, and left ventricular ejection fraction than those without HF (Table 1).
Table 1. Baseline characteristics of patients with and without heart failureTotal(n = 6,266)HF(n = 1,006)Non-HF(n = 5,260)P valueAge (y), mean (SD)70.0 (10.7)72.8 (11.1)69.5 (10.6)< 0.001≥75 y2,325 (37.1)497 (49.4)1,828 (34.8)< 0.001Body weight (kg), mean (SD)63.9 (12.6)61.4 (13.2)64.4 (12.4)< 0.001≤50 kg794 (12.7)189 (18.8)605 (11.5)< 0.001Body mass index (kg/m2), mean (SD)24.21 (3.62)23.72 (3.96)24.31 (3.54)< 0.001Hypertension5,188 (82.8)895 (89.0)4,293 (81.6)< 0.001Hyperlipidaemia4,926 (78.6)762 (75.7)4,164 (79.2)0.017Diabetes mellitus2,771 (44.2)567 (56.4)2,204 (41.9)< 0.001Current cigarette smoking1,327 (21.2)181 (18.0)1,146 (21.8)0.007Peripheral arterial disease438 (7.0)106 (10.5)332 (6.3)< 0.001Atrial fibrillation539 (8.6)192 (19.1)347 (6.6)< 0.001Malignancy389 (6.2)78 (7.8)311 (5.9)0.032Previous MI1,575 (25.1)394 (39.2)1,181 (22.5)< 0.001Previous PCI2,566 (41.0)470 (46.7)2,096 (39.8)< 0.001Previous CABG265 (4.2)85 (8.4)180 (3.4)< 0.001History of ischaemic stroke657 (10.5)153 (15.2)504 (9.6)< 0.001History of cerebral haemorrhage124 (2.0)25 (2.5)99 (1.9)0.216History of renal insufficiency1,114 (17.8)346 (34.4)768 (14.6)< 0.001Clinical presentation ACS2,015 (32.2)261 (25.9)1,754 (33.3)< 0.001 Unstable angina790 (12.6)83 (8.3)707 (13.4)0.003 Non-STEMI323 (5.2)59 (5.9)264 (5.0)- STEMI908 (14.5)119 (11.8)789 (15.0)- Hb (g/dL), Mean (SD)13.30 (2.04)12.43 (2.47)13.46 (1.90)< 0.001 Hb: <11 g/dL (both)727 (11.6)250 (24.9)477 (9.1)< 0.001 eGFR (mL/min/1.73 m^2^), Mean (SD)61.25 (27.61)50.36 (33.37)63.34 (25.84)< 0.001 eGFR: <60 mL/min/1.73 m^2^2,690 (42.9)631 (62.7)2,059 (39.1)< 0.001Angiographic features-No. of diseased vessels- 13,165 (50.5)419 (41.7)2,746 (52.2)< 0.001 21,864 (29.7)316 (31.4)1,548 (29.4)- 31,151 (18.4)256 (25.4)895 (17.0)- Left main disease349 (5.6)92 (9.1)257 (4.9)- LVEF (%), mean, Mean (SD)56.73 (12.94)46.18 (15.00)58.80 (11.41)< 0.001 ≤40%241 (12.7)119 (38.0)122 (7.7)< 0.001Procedural dataPuncture site Radial access only4,374 (69.8)570 (56.7)3,804 (72.3)< 0.001 Femoral access1,631 (26.0)365 (36.3)1,266 (24.1)- Brachial access269 (4.3)74 (7.4)195 (3.7)- Radial access4,517 (72.1)594 (59.0)3,923 (74.6)- Imaging guided5,918 (94.4)946 (94.0)4,972 (94.5)0.548 PCI for chronic total occlusion428 (6.8)78 (7.8)350 (6.7)0.219Medical status at discharge Aspirin6,148 (98.1)968 (96.2)5,180 (98.5)< 0.001 P2Y12 inhibitor6,209 (99.1)986 (98.0)5,223 (99.3)< 0.001 Prasugrel3,924 (62.6)538 (53.5)3,386 (64.4)< 0.001 Clopidogrel2,223 (35.5)435 (43.2)1,788 (34.0)< 0.001 OAC621 (9.9)223 (22.2)398 (7.6)< 0.001 Proton pump inhibitor5,302 (84.6)858 (85.3)4,444 (84.5)0.536 NSAIDs334 (5.3)55 (5.5)279 (5.3)0.818 Steroids249 (4.0)47 (4.7)202 (3.8)0.218 Antihyperlipidemic agent5,406 (86.3)812 (80.7)4,594 (87.3)< 0.001Modified ARC-HBR HBR patients3,192 (50.9)755 (75.0)2,437 (46.3)< 0.001 Complex PCI1,279 (20.4)259 (25.7)1,020 (19.4)< 0.001 High platelet reactivity (PRU > 208)2,229 (35.6)448 (44.5)1,781 (33.9)< 0.001Data are presented as mean (standard deviation) or n (%) valuesACS* Acute coronary syndrome, AF Atrial fibrillation, ARC-HBR Academic Research Consortium for High Bleeding Risk, CABG Coronary artery bypass, eGFR estimated glomerular filtration rate, Hb Haemoglobin, HFHeart failure, LVEF Left ventricular ejection fraction, MI Myocardial infarction, NSAIDs Non-steroidal anti-inflammatory drugs, OAC Oral anticoagulant, PCI Percutaneous coronary intervention, PRU P2Y12 Reaction Units, STEMI ST-elevation myocardial infarction*LVEF assessed at baseline is restricted to 1902 participants
Association of HF with outcomes
The risk of MACCE was 2.56 times higher in patients with than in those without HF (Fig. 1A). Cardiac death, noncardiac death, and nonfatal stroke contributed significantly to the higher MACCE rate in HF patients than in non-HF patients. However, there were no significant differences in stent thrombosis and nonfatal MI (Table 2.). After adjustment, HF was still an independent risk factor for MACCE, with an adjusted HR of 1.59. Other identified risk factors for MACCE were male, elderly, low body weight, diabetes mellitus, acute coronary syndrome, PAD, history of stroke, low estimated glomerular filtration rate, and low haemoglobin level (Table 3).Fig. 1. Cumulative incidence of (A) major adverse cardiac and cerebrovascular events (MACCE; the standard clinical definition comprising all-cause death, non-fatal MI, non-fatal stroke, and stent thrombosis) and (B) major bleeding after percutaneous coronary intervention by with or without heart failure. CI, confidence interval; HF, heart failure; HR, hazard ratioTable 2Cumulative incidence of MACCE, major bleeding, and their componentsEvent rate, n (%) HF(n=1006)Non-HF(n=5260)HR (95% CI)(Ref: Non-HF)P valueMACCE [a]185 (18.4)403 (7.7)2.556 (2.147 - 3.042)<.001All-cause death154 (15.3)249 (4.7)3.450 (2.822 - 4.217)<.001Cardiac death43 (4.3)21 (0.4)11.313 (6.714 - 19.064)<.001Non-cardiac death111 (11.0)228 (4.3)2.720 (2.168 - 3.413)<.001Non-fatal myocardial infarction20 (2.0)81 (1.5)1.352 (0.829 - 2.206)0.227Non-fatal stroke31 (3.1)93 (1.8)1.846 (1.230 - 2.772)0.003Stent thrombosis3 (0.3)22 (0.4)0.740 (0.222 - 2.472)0.625Major bleeding [b]94 (9.3)175 (3.3)3.021 (2.351 - 3.882)<.001BARC Bleeding Academic Research Consortium, CI Confidence interval, HF Heart failure, HR Hazard ratio, MACCE Major adverse cardiac and cerebrovascular events, MI Myocardial infarction[a] Includes all-cause death, non-fatal myocardial infarction, non-fatal stroke, and stent thrombosis[b] BARC 3 and 5Table 3Multivariate adjusted hazard ratios of MACCE and Major bleedingnEvents, n (%)Unadjusted HR (95% CI)P valueAdjusted HR (95% CI)P valueMACCE HF: yes vs. no1,006 vs. 5,260185 (18.4%) vs. 403 (7.7%)2.513 (2.085 - 3.028)<.0011.586 (1.301 - 1.933)<.001 Sex: female vs. male1,357 vs. 4,909127 (9.4%) vs. 461 (9.4%)0.978 (0.793 - 1.205)0.8310.660 (0.522 - 0.835)<.001 Age: ≥75 vs. <75 y2,325 vs. 3,941294 (12.6%) vs. 294 (7.5%)1.688 (1.423 - 2.004)<.0011.222 (1.014 - 1.474)0.035 Weight: ≤50 vs. >50 kg794 vs. 5,325130 (16.4%) vs. 443 (8.3%)2.061 (1.680 - 2.528)<.0011.766 (1.393 - 2.239)<.001 Diabetes: yes vs. no2,771 vs. 3,495324 (11.7%) vs. 264 (7.6%)1.540 (1.297 - 1.829)<.0011.285 (1.075 - 1.537)0.006 ACS: yes vs. no2,015 vs. 4,251203 (10.1%) vs. 385 (9.1%)1.170 (0.978 - 1.399)0.0851.355 (1.131 - 1.624)<.001 Peripheral arterial disease: yes vs. no438 vs. 5,82894 (21.5%) vs. 494 (8.5%)2.545 (2.003 - 3.233)<.0011.435 (1.112 - 1.853)0.006 History of cerebral infarction or haemorrhage: yes vs. no619 vs. 5,43393 (15.0%) vs. 465 (8.6%)1.821 (1.442 - 2.300)<.0011.400 (1.104 - 1.775)0.006 CKD: eGFR≥30-<60 vs. ≥60 mL/min/1.73 m22,093 vs. 3,431198 (9.5%) vs. 217 (6.3%)1.546 (1.263 - 1.892)<.0011.233 (0.998 - 1.524)<.001 CKD: eGFR <30 vs. ≥60 mL/min/1.73 m2597 vs. 3,431161 (27.0%) vs. 217 (6.3%)4.904 (3.957 - 6.076)2.470 (1.905 - 3.204) Anaemia: Hb≥11-<13 (M)≥11-<12 (F) vs. ≥13 (M)/≥12 g/dL (F)1,412 vs. 3,947169 (12.0%) vs. 237 (6.0%)2.123 (1.730 - 2.604)<.0011.521 (1.223 - 1.891)<.001 Anaemia: Hb <11 (both) vs. ≥13 (M)/≥12 g/dL (F)727 vs. 3,947154 (21.2%) vs. 237 (6.0%)3.973 (3.223 - 4.898)1.916 (1.484 - 2.473)Major Bleeding HF: yes vs. no1,006 vs. 5,26094 (9.3%) vs. 175 (3.3%)2.938 (2.242 - 3.849)<.0011.739 (1.300 - 2.325)<.001 Sex: female vs. male1,357 vs. 4,90961 (4.5%) vs. 208 (4.2%)1.111 (0.822 - 1.502)0.4940.723 (0.514 - 1.016)0.062 Weight: ≤50 vs. >50 kg794 vs. 5,32562 (7.8%) vs. 200 (3.8%)2.395 (1.787 - 3.210)<.0012.090 (1.494 - 2.922)<.001 Anaemia: Hb ≥11-<13 (M)/≥11-<12 (F) vs. ≥13 (M)/≥12 g/dL (F)1,412 vs. 3,94768 (4.8%) vs. 119 (3.0%)1.610 (1.176 - 2.206)<.0011.170 (0.845 - 1.619)0.002 Anaemia: Hb <11 (both) vs. ≥13 (M)/≥12 g/dL (F)727 vs. 3,94771 (9.8%) vs. 119 (3.0%)3.650 (2.694 - 4.946)1.903 (1.332 - 2.719) ACS: yes vs. no2,015 vs. 4,25188 (4.4%) vs. 181 (4.3%)1.153 (0.884 - 1.505)0.2941.391 (1.061 - 1.824)0.017 Peripheral arterial disease: yes vs. no438 vs. 5,82839 (8.9%) vs. 230 (3.9%)2.483 (1.734 - 3.555)<.0011.597 (1.093 - 2.333)0.016 Malignant tumour: yes vs. no389 vs. 5,87727 (6.9%) vs. 242 (4.1%)2.074 (1.380 - 3.116)<.0011.699 (1.124 - 2.568)0.012 Anticoagulation at discharge: yes vs. no621 vs. 5,64565 (10.5%) vs. 204 (3.6%)3.179 (2.372 - 4.260)<.0012.628 (1.939 - 3.563)<.001 CKD: eGFR ≥30-<60 vs. ≥60 mL/min/1.73 m22,093 vs. 3,431105 (5.0%) vs. 98 (2.9%)1.811 (1.355 - 2.420)<.0011.413 (1.045 - 1.910)<.001 CKD: eGFR <30 vs. ≥60 mL/min/1.73 m2597 vs. 3,43162 (10.4%) vs. 98 (2.9%)4.037 (2.877 - 5.667)2.119 (1.422 - 3.158)*ACS Acute coronary syndrome, CI Confidence interval, CKD Chronic kidney disease, eGFR estimated glomerular filtration rate, F Female, HR Hazard ratio, M Male, MACCE Major adverse cardiovascular and cerebrovascular events, PCI *Percutaneous coronary intervention
Effect on outcomes with HBR status by with or without HF
For this analysis, HF and non-HF patients were further stratified into HBR and non-HBR groups (Supplementary Table 1). In common with both HF and non-HF groups, HBR patients were older, underweight, and had more comorbidities such as hypertension, PAD, malignancy, haemodialysis, history of stroke, atrial fibrillation, and more multi-vessel disease than non-HBR patients (Supplementary Table 1). In addition, smoking was rather infrequent, and the rate of ACS was low in HBR patients (Supplementary Table 1).
The results showed that the incidence of MACCE was about 3.2-fold higher in HBR patients with HF and about 2.8-fold higher in those without HF than in non-HBR patients (Fig. 2A). The rate of MACCE in HF patients without HBR was lower than that of non-HF patients with HBR. The components of MACCE with and without HBR are shown in the supplementary tables (Supplementary Tables 2, 3).
Fig. 2. Cumulative incidence of (A) major adverse cardiac and cerebrovascular events (MACCE; the standard clinical definition comprising all-cause death, non-fatal MI, non-fatal stroke, and stent thrombosis) and (B) major bleeding after percutaneous coronary intervention by with or without heart failure and HBR. CI, confidence interval; HBR, high bleeding risk; HF, heart failure; HR, hazard ratio
Major bleeding was also about 2.3 to 2.4 times more common in HBR patients compared with non-HBR patients, irrespective of HF (Fig. 2B).
Table 4 shows the outcomes of the Cox proportional hazards models analyses. There was no evidence of interactions with HBR status by the prevalence of HF for MACCE and major bleeding (HR 0.97. 95%CI 0.55–1.70, p for interaction = 0.913, HR 1.31, 95% CI 0.64–2.70, p for interaction 0.456 respectively).
Table 4. Multivariate adjusted hazard ratios of MACCE and major bleeding according to HF and HBR n Events, n (%)HR (95% CI)P valueMACCE [1] HF vs. Non-HF1,006 vs. 5,260185 (18.4%) vs. 403 (7.7%)1.872 (1.524–2.300)< 0.001 HBR vs. Non-HBR3,192 vs. 3,074447 (14.0%) vs. 141 (4.6%)2.933 (2.330–3.692)< 0.001Interaction HF * HBR--0.969 (0.551–1.705)0.913Major bleeding [2] HF vs. Non-HF1,006 vs. 5,26094 (9.3%) vs. 175 (3.3%)2.262 (1.236–4.141)0.008 HBR vs. Non-HBR3,192 vs. 3,074198 (6.2%) vs. 71 (2.3%)2.666 (1.891–3.758)< 0.001Interaction HF * HBR--1.309 (0.636–2.694)0.465ACS Acute coronary syndrome, CI Confidence interval, HF Heart failure, HR Hazard ratio, MACCE Major adverse cardiac and cerebrovascular events, PAD Peripheral arterial disease[1] multivariable Cox proportional hazards model: adjusted with sex, DM, ACS, PAD[2] multivariable Cox proportional hazards model: adjusted with sex, ACS, PAD
Discussion
The present study showed that (1) after PCI, HF patients are at significantly higher risk of MACCE and major bleeding events, (2) HBR is associated with higher MACCE and major bleeding irrespective of HF and non-HF patients, and (3) both HF and HBR are independent determinants of MACCE and major bleeding. Therefore, this study suggests that each was independently associated with prognosis and should be considered in management.
There were significantly more MACCE (2.56 folds) and major bleeding events (3.02 folds) in HF patients after PCI. Furthermore, even after adjustment, HF was a risk factor for both MACCE and major bleeding. The American College of Cardiology/American Heart Association guidelines also reported that a history of congestive HF is a high-risk condition for cardiovascular events [16]. HF creates a hypercoagulable state that is associated with adverse events, including stroke, systemic embolism, and mortality [17–20]. Interestingly, in the present study, HPR, suggesting ineffectiveness of antiplatelet agents, was observed more frequently in HF patients. This may be due to the elevated levels of pro-thrombotic and pro-inflammatory cytokines observed in patients with HF. Thus, inadequate antiplatelet action may be the cause of the higher MACCE rate in HF patients. All other identified risk factors for MACCE in this study were consistent with previous reports and well-known factors [8, 21, 22]. The majority of the identified factors were components of the ARC-HBR in which consensus agreement was achieved. Further, HF was suggested to be an independent factor for major bleeding [22]. Previous studies reported incidence rates of bleeding events ranging from 8.0% to 12.9% in patients undergoing PCI with HF. [23, 24] The incidence rate of major bleeding events in HF patients after PCI was 9.3% in the present study, which was consistent with the results of previous studies. Thus, the risk of major bleeding after PCI for patients with HF is likely to be extremely high, because ARC defined HBR as an annual major bleeding event rate > 4%. The association between the pathophysiology of HF and bleeding has been mentioned to involve low cardiac output and increased central venous pressure due to congestive heart failure causing abnormal intestinal function, which induces bleeding from the mucosa of the gastrointestinal tract [25]. In addition, heart failure patients after PCI needed to receive antiplatelet therapy, further increasing the risk of bleeding, including gastrointestinal bleeding [24]. Another explanation is that HF frequently coexists with many features included in the HBR criteria and is similarly associated with multiple comorbidities, concomitant medications, and a higher rate of hospital readmissions, etc. In Japan, the impact of HF may be more pronounced than in other countries. It has been reported that many HF patients in Japan are underweight and frail, whereas many HF patients overseas are obese. Indeed, in the present study, the HF group had significantly lower weight than the non-HF group. In addition, the HF group had significantly lower Hb and more frequent anaemia than the non-HF group.
HF increased the risk of MACCE and major bleeding, and HBR increased the risk of MACCE and major bleeding regardless of HF. Since the present study found no interaction in the relationship between HF and HBR for MACCE and major bleeding, HF and HBR are likely to be independently related to prognosis. The wide confidence intervals indicate limited power for the interaction analyses; nonsignificant results should not be taken as evidence of equivalence. Conclusions on the independence of HF and HBR effects remain tentative, and larger studies are needed to confirm potential effect modification. A previous study reported that patients with bleeding events after PCI had significantly higher rates of cardiovascular events [26, 27]. In addition, there is a report that bleeding events in acute decompensated HF were associated with HF re-hospitalization [28]. In this study, many patient characteristics overlapped between HBR and HF, suggesting that the observed association between bleeding and cardiovascular events may reflect shared underlying mechanisms. However, this interpretation remains speculative, as no temporal analyses were conducted to formally support a causal or sequential relationship. The plausible mechanisms of bleeding events with subsequent mortality include activation of the coagulation cascade, increased prothrombotic cytokine levels, hypovolemia, anaemia, reflex tachycardia, transfusion of blood products, and cessation of antiplatelet and anticoagulant therapies [26]. In particular, as a potential mechanism underlying bleeding-induced inflammation and prothrombotic states, it has been demonstrated that the hemostatic process following bleeding can trigger inflammation, which in turn serves as a potent prothrombotic stimulus by activating platelets and the coagulation cascade [29].
Clinical implications
In the present study, HF patients had more atrial fibrillation and anticoagulants than non-HF patients, resulting in high rates of bleeding, as well as a high percentage of patients with low EF and undergoing complex PCI and a high risk of cardiovascular thrombotic events.
That the P2Y12-infibitor monotherapy reduced bleeding events without increasing ischemic events in patients undergoing complex PCI was reported [30]. In this study, nearly all patients were discharged on dual antiplatelet therapy, suggesting that subsequent transition to P2Y12 inhibitor monotherapy may contribute to improved clinical outcomes.
Therefore, optimizing the balance between ischemic and bleeding events is important for HF patients undergoing PCI, such as those included in this study, especially those with AF. Careful risk management during both the peri-PCI and post-PCI phases is essential to improve outcomes in AF patients undergoing PCI [31]. For example, procedural strategies using intracoronary imaging, the appropriate selection of antithrombotic agents, and the tailoring of treatment duration are critical considerations. Moreover, the safety and efficacy of direct oral anticoagulant monotherapy as an antithrombotic strategy for patients with HF, coronary artery disease, and AF have been reported, suggesting that such an approach may help reduce both bleeding and cardiovascular events in the high-risk population represented in the present study [32].
Furthermore, HF patients underwent complex PCI more frequently than non-HF patients, and consequently the use of femoral artery access was also higher in this study. These findings suggest that access site selection may have contributed to the increased incidence of bleeding events following PCI. The importance of selecting an access site that minimizes periprocedural bleeding complications during PCI has been well recognized. [33] Procedural characteristics differed substantially between HF and non-HF groups, and only limited adjustment was feasible, which may have influenced bleeding comparisons. Unfortunately, further stratified analyses were not possible with the available data. Future studies are warranted to clarify the impact of procedural strategies in this high-risk population.
In summary, patients with factors of HF and HBR after PCI should be considered more important in daily clinical practice to improve their prognosis. In addition, we should pay attention to the occurrence of major bleeding, as well as MACCE, after PCI for patients with HF. Although HF is not widely recognized as a risk factor for major bleeding, major bleeding may be a cause of subsequent MACCE. Therefore, such patients should be recognized as a high-risk population, warranting long-term risk monitoring and frequent follow-up. In addition, careful consideration of the optimal antithrombotic therapy for each individual patient is essential. In the future, larger studies aimed at reducing the risk of MACCE and bleeding events in a general population of HF patients after PCI seem warranted.
Study limitations
There are several limitations to the present study. This analysis used data from the PENDULUM registry and was conducted in a post-hoc manner, meaning that the absence of prespecified hypotheses and statistical models entails inherent risks of multiplicity and analytical bias. As such, causal inferences should be made with caution, and the results may be subject to residual or unmeasured confounding. This is particularly relevant because both HF and bleeding outcomes are influenced by various clinical, procedural, and therapeutic factors not fully captured in our data. In addition, although residual and unmeasured confounding factors could not be included in the Cox model, limiting the interpretation of our findings, the present study provides valuable insights into the outcomes of HF patients undergoing PCI. Future hypothesis-driven investigations in well-defined HF cohorts are needed to confirm these findings and strengthen the evidence for clinical practice. Further, information on the New York Heart Association functional class, Brain natriuretic peptide, a presence of prior hospitalization, and adverse events related with HF was lacking. As NT-proBNP measurements and echocardiographic data were unavailable, misclassification between HF with reduced and preserved ejection fraction cannot be excluded. Such nondifferential misclassification would likely bias associations toward the null, while the under-recognition of milder HF may overestimate risk among identified HF patients. Although history-based identification is clinically straightforward, the absence of standardized diagnostic criteria limits the interpretation of our findings. Additionally, a substantial proportion of important variables, including left ventricular EF, were missing in this registry. Imputation was not performed due to the high rate of missingness. This limitation may introduce bias and reduce the precision of the estimates, and therefore the results should be interpreted with caution. The causal relationship between HF and bleeding events was unclear. Because the PENDULUM study was not designed as a dedicated heart failure registry, detailed information regarding HF medications and treatment trajectories was not systematically collected. As a result, our ability to assess treatment effects or derive specific management implications is limited. The study population consisted entirely of Japanese patients, who exhibit the “East Asian paradox” of lower thrombotic and higher bleeding risk. [34] Consequently, the thrombotic and bleeding profiles may differ from Western populations, limiting the generalizability of our findings. Nonetheless, as previously reported, the relationship between platelet function and thrombotic events observed in ADAPT-DES [14] appears to be consistent with that in the PENDULUM study [7, 8].
Conclusions
In patients after contemporary PCI, HF and HBR were independently associated with a higher risk of MACCE and bleeding. De-escalation management of antithrombotic drugs that prevent major bleeding and reduce subsequent cardiovascular events is justified in HF and HBR cases. Future studies should focus on validating these results in a more generalized population of HF patients after PCI. There is also a need for prospective studies on this topic.
Data Availability
The datasets are available from the corresponding author on reasonable request.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nakamura M, Kadota K, Takahashi A, Kanda J, Anzai H, Ishii Y et al. Relationship between platelet reactivity and ischemic and bleeding events after percutaneous coronary intervention in East Asian patients: 1-year results of the PENDULUM registry [published correction appears in J Am Heart Assoc. 2020;9 e 014557]. J Am Heart Assoc. 2020;9:e 015439.10.1161/JAHA.119.015439 PMC 766088932394794 · doi ↗ · pubmed ↗
- 2Stone GW, Witzenbichler B, Weisz G, Rinaldi MJ, Neumann FJ, Metzger DC et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): A prospective multicentre registry study [published correction appears in Lancet. 2014;383:1128]. Lancet. 2013;382:614–623.10.1016/S 0140-6736(13)61170-823890998 · doi ↗ · pubmed ↗
- 3Yazaki Y, Nakamura M, Iijima R, Yasuda S, Kaikita K, Akao M, et al. Clinical Outcomes of Rivaroxaban Monotherapy in Heart Failure Patients With Atrial Fibrillation and Stable Coronary Disease: Insights From the AFIRE Trial. Circulation. 2021;144:1449-145133. 10.1161/CIRCULATIONAHA.121.05537434694893 · doi ↗ · pubmed ↗
- 4Scalise RFM, Salito AM, Polimeni A, Garcia-Ruiz V, Virga V, Frigione P, et al. Radial Artery Access for Percutaneous Cardiovascular Interventions: Contemporary Insights and Novel Approaches. J Clin Med. 2019;8:1727.10.3390/jcm 8101727 PMC 683302831635342 · doi ↗ · pubmed ↗
- 5Mak KH, Bhatt DL, Shao M, Hankey GJ, Easton JD, Fox KAA et al. Am heart J. Ethnic variation in adverse cardiovascular outcomes and bleeding complications in the clopidogrel for high atherothrombotic risk and ischemic Stabilization, Management, and avoidance (CHARISMA) study. 2009;157:658–65.10.1016/j.ahj.2008.08.03119332192 · doi ↗ · pubmed ↗