Bilateral Multiple Thoracic Disc Herniation Decompressed Through a Posterior Transpedicle Approach: A Case Report
Mohammed Awad Mohammed, Ahmed M. Sonbol, Farid Kassab, Meshal Altowairqi, Hassan Sirajaldeen Alhassan Ali, Mohammed M. Elgack, Saeed Alshwekany

TL;DR
A rare case of four-level thoracic disc herniation was successfully treated using a less invasive posterior surgical approach.
Contribution
Demonstrates the effectiveness of a posterior transpedicle approach for multiple thoracic disc herniations.
Findings
The posterior transpedicle approach enabled safe decompression of four-level thoracic disc herniations.
This approach avoids the need for more invasive or combined surgical techniques.
The method is suitable for herniations at multiple consecutive levels and in different directions.
Abstract
A four-level thoracic disc prolapse is extremely rare, especially when surgical intervention is required. The level of the disc and the herniation's direction determine the surgical approach of selection. A 46-year-old male presented with a two-week history of severe, sudden back pain and weakness in his lower extremities. Clinical presentation was suggestive of thoracic radiculopathy and myelopathy. Magnetic resonance imaging confirmed four-level disc prolapses at the levels of T9-T10, T10-T11, and T11-T12, which were central and in both directions. Decompression and fixation were done through the posterior transpedicular approach. The surgical approaches for decompression of multiple thoracic disc herniations are not commonly discussed in the literature due to their rarity. Generally, the anterior trans-thoracic approach is preferred over the posterior approach for one or two-level…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
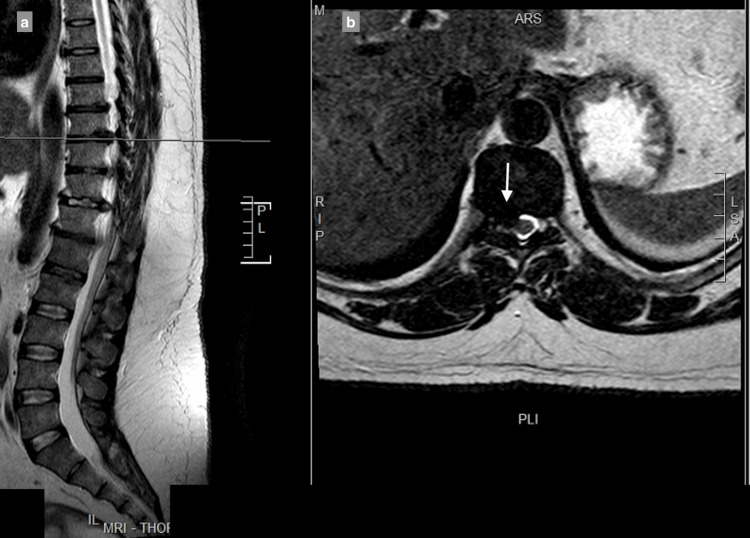 Figure 1
Figure 1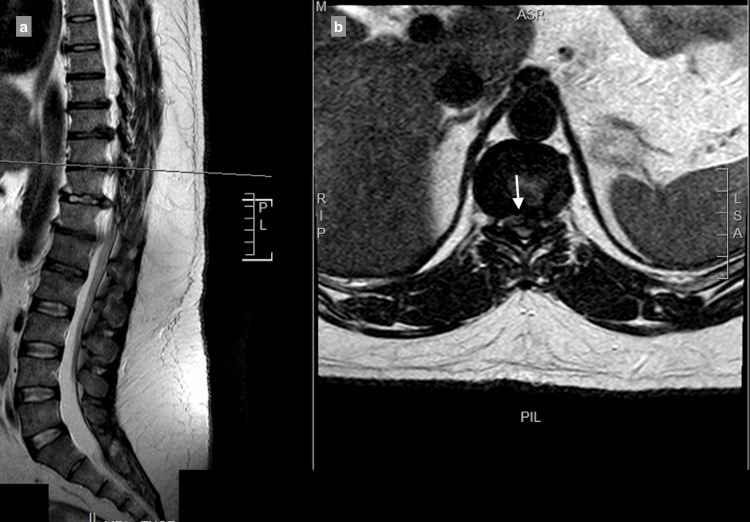 Figure 2
Figure 2 Figure 3
Figure 3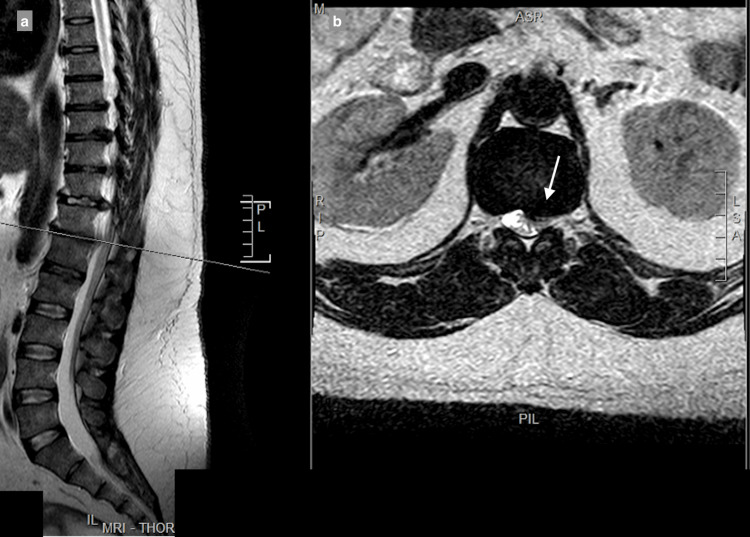 Figure 4
Figure 4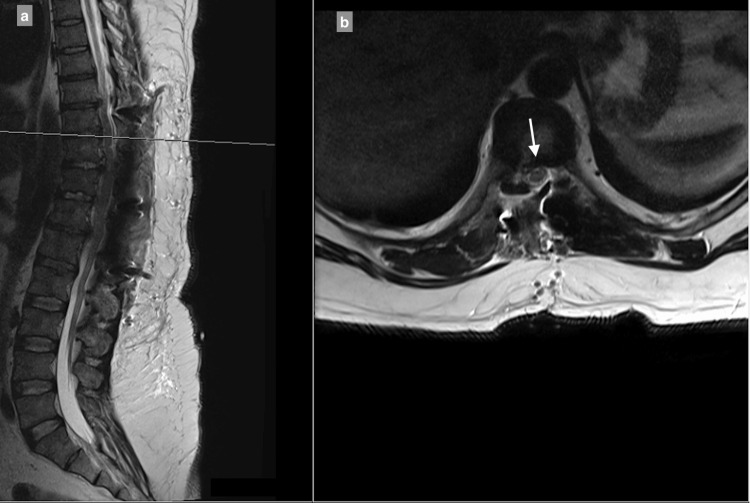 Figure 5
Figure 5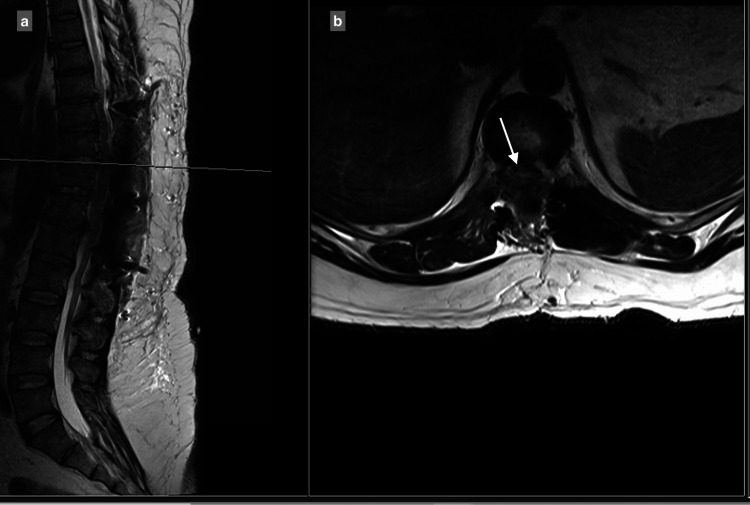 Figure 6
Figure 6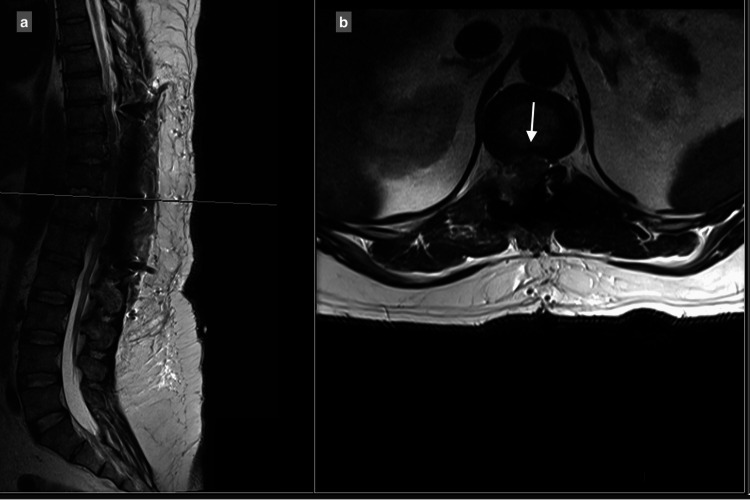 Figure 7
Figure 7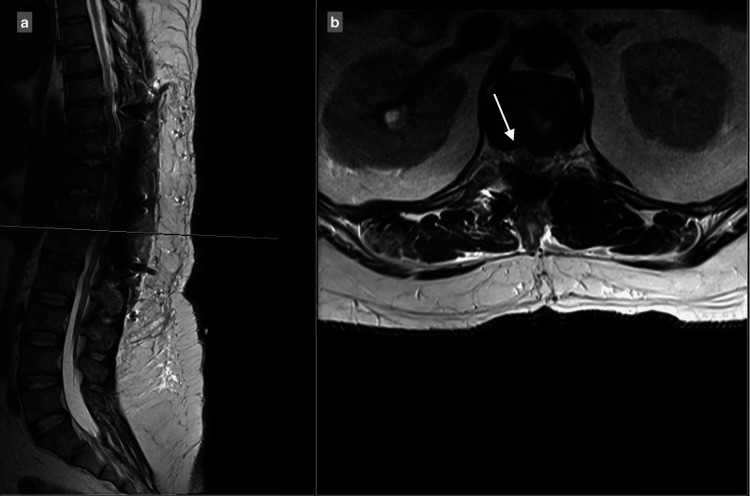 Figure 8
Figure 8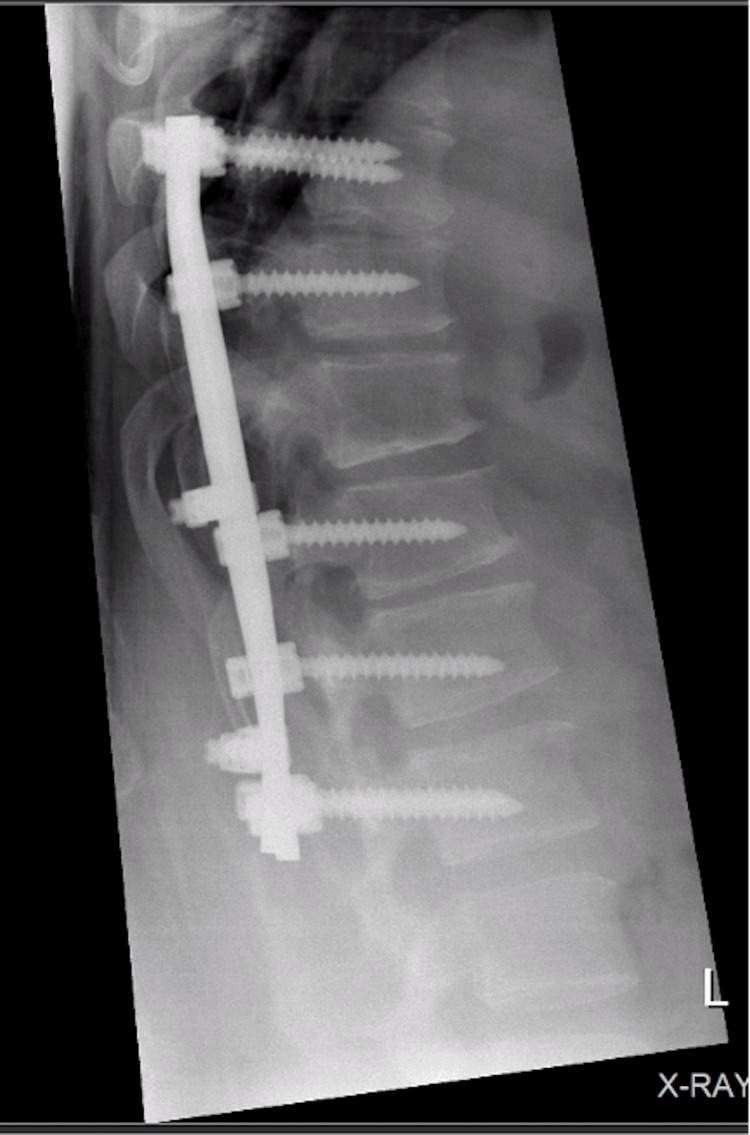 Figure 9
Figure 9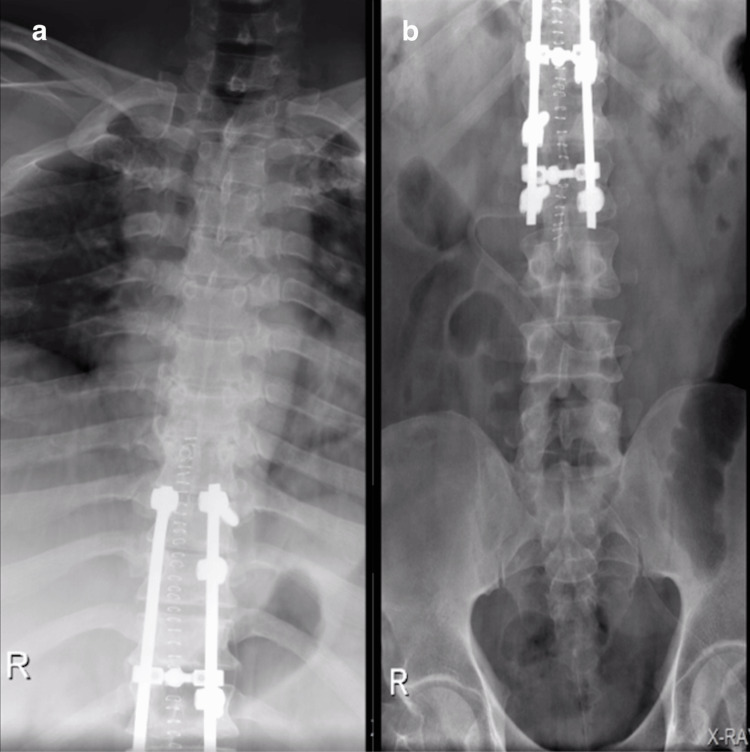 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Scoliosis diagnosis and treatment
Introduction
Disc herniation occurs in approximately 40-50 per 100,000 individuals, making it a relatively common condition. Thoracic disc herniation, by contrast, is extremely rare, with an estimated prevalence of 1 per 1,000,000 individuals [1]. A herniated or bulged disc may compress the neural elements [2]. The presentation and the diagnosis of thoracic disc herniation can be challenging because it can mimic other pathologies such as muscular chest wall pain, herpes zoster, gallstones, cholecystitis, and peptic ulcer [3]. Magnetic resonance imaging (MRI) is the preferred imaging modality for providing detailed assessment and accurate diagnosis of spinal pathology [4]. Management ranges from conservative measures to invasive surgical intervention, with the choice of surgical approach depending on the level of the disc and the direction of herniation [5-7]. Generally, the anterior trans-thoracic approach is preferred over the posterior approach for one or two-level herniation [5,8,9]. In this case, the presentation was deceptive, and the herniated discs were bilateral and at four levels. The surgical approach chosen was less invasive, and all the pathologies were approachable. This case report is noteworthy due to the limited literature discussing surgical approaches for multiple thoracic disc herniations requiring decompression.
Case presentation
A 46-year-old male presented with a two-week history of severe, sudden back pain and weakness in his lower extremities, inability to walk, and numbness involving his legs. The neurological examination revealed an inability to overcome gravity in the testable myotomes of the levels of L2, L3, L4, L5, and S1 of the bilateral lower extremities. Sensory testing for crude and fine touch, pain, and temperature was unremarkable bilaterally. Reflex examination showed hyperreflexia at the patellar tendon with the presence of clonus.
MRI showed a central and right-sided disc prolapse at the T9-T10 level, a central disc prolapse at the T10-T11 level, a central and right-sided disc prolapse at the T11-T12 level, and a central and left-sided disc prolapse at the T12-L1 level, all causing cord compression at multiple levels (Figure 1-4).
9–T10 central and right-sided disc extrusion causing spinal canal stenosis with compression of the spinal cord: (a) T2-weighted sagittal view; (b) T2-weighted axial view.
T10-T11 central disc prolapse causing spinal canal stenosis, with compression of the spinal cord: (a) T2 sagittal view, (b) T2 axial view.
T11-T12 central disc and right-sided disc extrusion causes spinal canal stenosis, with compression of the spinal cord: (a) T2 sagittal view, (b) T2 axial view.
Central and left-sided T12–L1 disc prolapse causing spinal canal stenosis, with compression and a fanning appearance of the spinal cord: (a) T2 sagittal view, (b) T2 axial view.
Preoperative planning
A thoracotomy was considered for disc removal because the T10-T11 herniation was central and difficult to access via a posterior approach, whereas the remaining levels were amenable to posterior decompression. However, performing a thoracotomy would have required a thoracolumbar frenotomy to access T12-L1, which would not have facilitated decompression of the upper levels. Additionally, the disc herniations were located on both the right and left sides, potentially necessitating bilateral access, further limiting the suitability of a thoracotomy. Based on these considerations, a posterior transpedicular approach was selected.
Surgical technique and preparation
The patient was placed in a prone position on the Wilson frame. Motor evoked potentials were continuously monitored intraoperatively. A midline posterior approach was employed, with exposure of the bilateral laminae and facets from T9 to L2. Instrumentation was placed as follows: bilateral pedicle screws at T9, a unilateral left pedicle screw at T10, T11 was skipped, a unilateral left pedicle screw at T12, a unilateral right pedicle screw at L1, and bilateral pedicle screws at L2.
The decompression process commenced with specific actions at varying vertebral levels. At the T12-L1 level, a hemilaminectomy was conducted on the left to perform a foraminectomy. By moving laterally to the cord, the bulging disc was identified, excised, and completely removed. Moving on to the T11-T12 level, a hemilaminectomy was carried out on the right side, and the bulging disc was removed through a laminectomy procedure without affecting the cord. Progressing to the T10-T11 level, a complete laminectomy was undertaken, and bilateral laminectomies were performed to remove the disc from both sides. A hooked instrument was utilized to reach the center and excise the bulging disc entirely. Subsequently, at the T9-T10 level, a hemilaminectomy was performed on the right side, alongside the foraminectomy, to remove the bulging disc without impacting the cord. Connecting rods were then introduced between T9 and L2 and secured using transverse rod connectors. Decortication was performed with autograft material to facilitate fusion. During the procedure, all discs were noted to be soft, and no calcification was encountered. Following the surgery, post-operative X-ray and MRI scans revealed satisfactory decompression and fixation, as depicted in Figures 5-10.
Postoperative MRI of T9-T10 showing the decompressed spinal cord with no apparent stenosis or collection: (a) T2 sagittal view, (b) T2 axial view.
Postoperative MRI of T10-T11 showing the decompressed spinal cord with no apparent stenosis or collection: (a) T2 sagittal view, (b) T2 axial view.
Postoperative MRI of T11-T12 showing the decompressed spinal cord with no apparent stenosis or collection: (a) T2 sagittal view, (b) T2 axial view.
Postoperative MRI of T12-L1 showing the decompressed spinal cord with no apparent stenosis or collection: (a) T2 sagittal view, (b) T2 axial view.
Postoperative X-ray lateral view showing good alignment with no loosening of the fused levels.
Postoperative X-ray A/P view showing good alignment with no loosening of the fused levels: (a) Thoracic spine (b) Thoraco-lumbar junction and lumbar spine.
The postoperative course was uneventful, with no change in neurological status during the three-day hospital stay. At the 2-month follow-up, following a structured physical therapy regimen, the patient exhibited a 30% increase in quadriceps muscle strength and a marked improvement in gait stability and balance during weight-bearing activities. He was walking normally with some deficit in light touch and pain sensations in the feet. At the 8-month follow-up, the patient has regained his baseline lower extremity strength and reports experiencing only mild back discomfort.
Discussion
Multilevel and bilateral thoracic disc herniations are rare, with an estimated annual incidence of approximately 1 per million individuals, and account for a small proportion of all disc herniations. Surgical intervention involving multiple levels is uncommon and remains inadequately addressed in the literature, which is largely limited to case reports and small clinical studies focusing on diagnostic considerations, surgical approaches, and patient outcomes [4,10].
Stillerman et al. followed 82 patients with thoracic disc herniation who underwent surgical decompression [11]. The choice of surgical approach for each patient depends on the position of the herniated disc, with the transthoracic approach being the most commonly used. Other surgical approaches include the transfacet pedicle-sparing, lateral extracavitary, and transpedicular techniques. Bohlman et al followed 19 patients with thoracic disc herniation who needed surgery [6]. Decompression was performed via an anterior transthoracic approach, which was found to carry a risk of spinal cord injury. Dickman et al. concluded that the anterior transthoracic approach is preferred for large central herniations, calcified discs, or transdural disc herniations, as posterior approaches in these settings carry a high risk of neurological injury [7]. Currier et al. performed 19 transthoracic discectomies and fusions, and they found that the procedure was safe. Conversely, laminectomies were commonly associated with neurologic deterioration [8]. While the transthoracic approach provides superior exposure for lower thoracic disc lesions, it was linked to higher morbidity and complication rates. In contrast, the transpedicular posterior approach affords ample exposure coupled with decreased surgical duration and blood loss, facilitating prompt mobilization and discharge [12]. The long-term outcomes of the posterior approach were comparable to those of the transthoracic approach [13].
In this case, the decision to utilize a posterior transpedicular approach was based on its minimally invasive nature. Moreover, given the presence of herniated discs across four contiguous levels with bilateral involvement, a combined approach would have required a more extensive surgical procedure. The herniated discs had no evidence of calcification, adhesions, or transdural penetration. Adequate access was achieved to decompress right-central, central, and left-central herniated discs. Obstacles, like disc adhesions, calcifications, and intradural penetration, may affect the decompression through the posterior approach and could lead to poor outcomes.
Conclusions
For multiple thoracic disc herniations requiring surgery, the posterior transpedicular approach provides bilateral access to the discs, allowing safe and adequate decompression while avoiding more invasive or combined approaches. It is important to note that factors such as disc adhesions, calcifications, and intradural penetration may limit decompression and contribute to suboptimal outcomes with this approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thoracoscopic treatment for single level symptomatic thoracic disc herniation: a prospective followed cohort study in a group of 167 consecutive cases Eur Spine J Quint U Bordon G Preissl I Sanner C Rosenthal D 6376452120122216009910.1007/s 00586-011-2103-0PMC 3326138 · doi ↗ · pubmed ↗
- 2Disc Herniation Dydyk AM Ngnitewe MR Mesfin FB Treasure Island (FL)Stat Pearls 2023 https://europepmc.org/article/med/28722852
- 3Thoracic disc herniations Neurosurg Clin N Am Dietze Jr DD Fessler RG 7590419938428158 · pubmed ↗
- 4The incidence and most common levels of thoracic degenerative disc pathologies Turk J Phys Med Rehabil Sarsılmaz A Yencilek E ÖzelçiÜ Güzelbey T Apaydın M 1551616420183145350610.5606/tftrd.2018.1302 PMC 6657757 · doi ↗ · pubmed ↗
- 5Thoracic Discogenic Syndrome Munakomi S; Mesfin FB Treasure Island (FL)Stat Pearls 2023 https://www.ncbi.nlm.nih.gov/books/NBK 470388/29262010 · pubmed ↗
- 6Anterior excision of herniated thoracic discs J Bone Joint Surg Am Bohlman HH Zdeblick TA 10381047701988 https://journals.lww.com/jbjsjournal/abstract/1988/70070/Anterior_excision_of_herniated_thoracic_discs_.12.aspx 3403572 · pubmed ↗
- 7Reoperation for herniated thoracic discs J Neurosurg Dickman CA Rosenthal D Regan JJ 15716291199910.3171/spi.1999.91.2.015710505498 · doi ↗ · pubmed ↗
- 8Transthoracic disc excision and fusion for herniated thoracic discs Spine (Phila Pa 1976) Currier BL Eismont FJ Green BA 323328191994817136510.1097/00007632-199402000-00012 · doi ↗ · pubmed ↗