Interactive Virtual Assistant for Health Promotion Among Older Adults With Type 2 Diabetes: The IVAM-ED Randomized Clinical Trial
Lucas S. Matzenbacher, Frederico Ludwig da Costa, Laura Gomes Boabaid de Barros, Vicenzo Gheno, Isabela Semmelmann Maia, Luiza Machado Blank, Maria Antônia Bertuzzo Brum, Lucas Friedrich Fontoura, Thiago Wendt Viola, Carla Helena Augustin Schwanke, Giovani Gadonski

TL;DR
An interactive virtual assistant improved mental health and diabetes management in older adults with type 2 diabetes over 12 weeks.
Contribution
Demonstrates that a smart speaker-based behavioral intervention can effectively support mental and physical health in older diabetes patients.
Findings
Participants using the virtual assistant had significantly reduced mental distress compared to usual care.
The intervention improved quality of life and adherence to diabetes self-care behaviors.
Glycemic control improved in the intervention group, with no adverse events reported.
Abstract
Can an interactive virtual assistant device with a behavioral intervention model improve mental health and diabetes management among older individuals with diabetes? In this randomized clinical trial involving 112 older adults with type 2 diabetes, participants who used the interactive virtual assistant device experienced significant improvements in mental distress compared with those who received usual care. These findings suggest that an interactive virtual assistant device may enhance mental health outcomes for older individuals with diabetes, serving as a valuable add-on to support and complement existing treatment regimens. This randomized clinical trial evaluates whether an interactive virtual assistant device with a behavioral intervention model can improve mental health and diabetes management among older adults with diabetes. Older patients with diabetes often experience…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
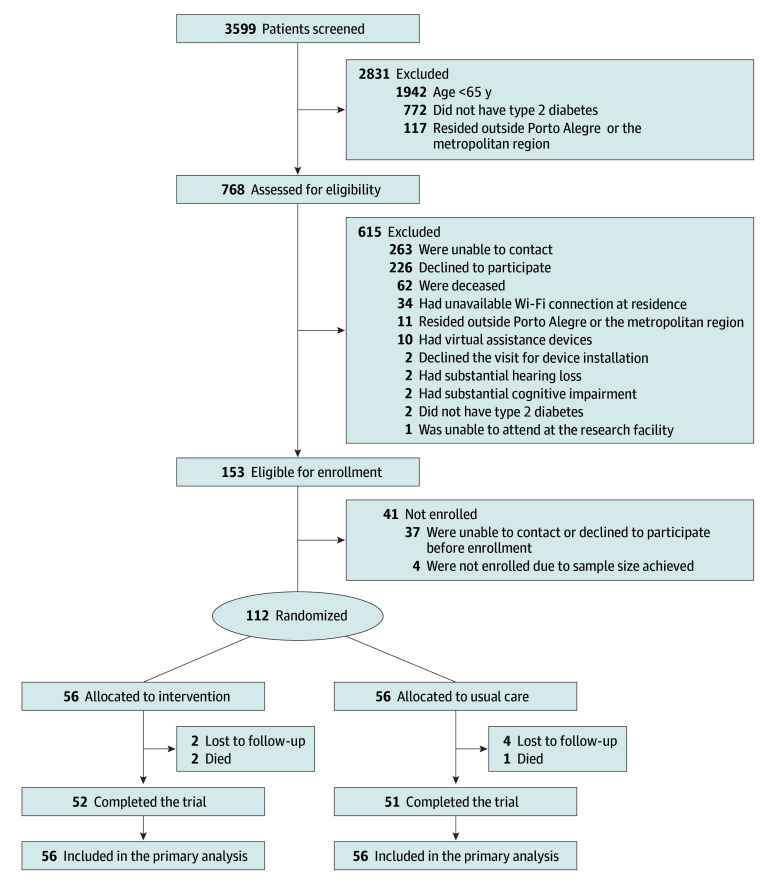 Figure 1
Figure 1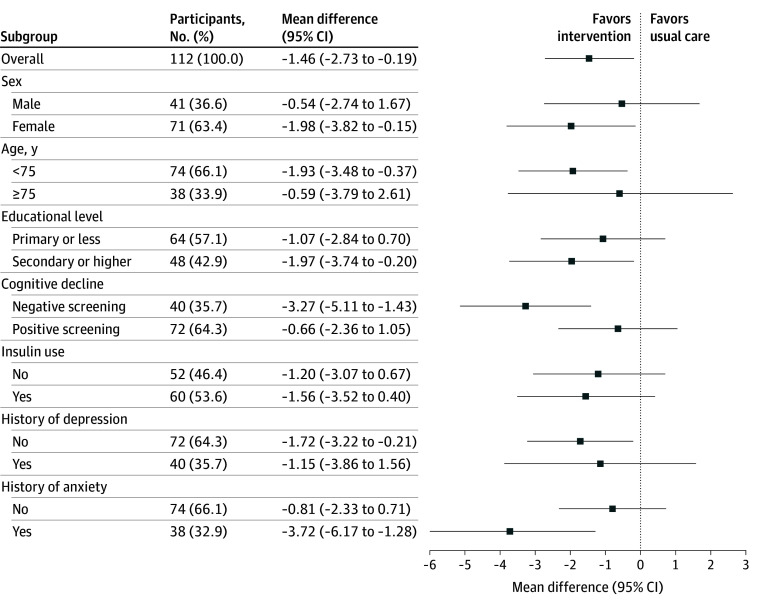 Figure 2
Figure 2| Characteristic | Usual care group (n = 56) | Smart speaker group (n = 56) |
|---|---|---|
| Age, y | 72.4 (6.0) | 72.6 (5.4) |
| Weight, kg | 76.0 (15.3) | 77.1 (15.3) |
| BMI | 30.0 (6.1) | 31.2 (6.0) |
| Sex, No. (%) | ||
| Female | 37 (66.1) | 34 (60.7) |
| Male | 19 (33.9) | 22 (39.3) |
| Educational level, No. (%) | ||
| No qualification | 6 (10.7) | 11 (19.6) |
| Primary education | 32 (57.1) | 36 (64.3) |
| Secondary education | 16 (28.6) | 7 (12.5) |
| University degree or higher | 2 (3.6) | 2 (3.6) |
| Educational level, y | 7.5 (3.9) | 6.4 (4.2) |
| Monthly income, No. of Brazilian minimum wages | 2.5 (2.7) | 2.1 (2.2) |
| Diabetes duration, y | 16.5 (11.1) | 17.3 (12.2) |
| Diabetes complication, No. (%) | ||
| Macrovascular | 37 (66.1) | 36 (64.3) |
| Microvascular | 28 (50.0) | 35 (62.5) |
| Diabetes medication, No. (%) | ||
| Oral hypoglycemic agents | ||
| Metformin | 49 (87.5) | 42 (75.0) |
| Sulfonylureas | 17 (30.4) | 15 (26.8) |
| SGLT-2 inhibitors | 11 (19.6) | 17 (30.4) |
| DPP-4 inhibitors | 5 (8.9) | 2 (3.6) |
| Glitazones | 2 (3.6) | 0 |
| GLP-1 receptor agonists | 1 (1.8) | 0 |
| Insulin | 28 (50.0) | 32 (57.1) |
| HbA1c level, % | 7.8 (1.5) | 8.0 (1.6) |
| HbA1c level, mmol/mol | 61.7 (16.0) | 63.4 (17.0) |
| Mental health, No. (%) | ||
| Suicidal thoughts | 7 (12.5) | 5 (8.9) |
| Depression | 21 (37.5) | 19 (33.9) |
| Anxiety | 23 (41.1) | 15 (26.8) |
| Bipolar disorder | 2 (3.6) | 1 (1.8) |
| Blood pressure, mm Hg | ||
| Systolic | 136.5 (22.0) | 135.8 (20.9) |
| Diastolic | 75.4 (10.3) | 77.1 (10.6) |
| Plasma lipid level, mg/dL | ||
| Total cholesterol | 177.0 (48.6) | 181.1 (48.4) |
| LDL cholesterol | 98.9 (37.9) | 101.3 (41.6) |
| HDL cholesterol | 50.7 (13.3) | 49.2 (14.7) |
| Triglycerides | 165.0 (90.2) | 195.2 (149.2) |
| MMSE score | 24.8 (4.0) | 23.5 (4.5) |
| SRQ-20 score | 7.0 (4.7) | 7.9 (5.2) |
| SCI-R score | 36.5 (5.9) | 35.2 (6.8) |
| PSS score | 23.6 (10.3) | 20.6 (10.3) |
| SF-36 score | 50.2 (21.5) | 50.9 (22.2) |
| SRQ-20 score | Usual care group (n = 56) | Smart speaker group (n = 56) | Mean difference (95% CI) | Effect size | |
|---|---|---|---|---|---|
| At baseline, mean (SD) | 7.04 (4.67) | 7.89 (5.15) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE) | 7.66 (0.43) | 6.39 (0.45) | −1.28 (−2.51 to −0.04) | 0.41 | .04 |
| At 12 w, fully adjusted mean (SE) | 7.75 (0.42) | 6.29 (0.44) | −1.46 (−2.73 to −0.19) | 0.48 | .02 |
| Outcome | Usual care group (n = 56) | Smart speaker group (n = 56) | Mean difference (95% CI) | Effect size | |
|---|---|---|---|---|---|
| HbA1c | |||||
| At baseline, mean (SD), % | 7.80 (1.47) | 7.95 (1.55) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE), % | 8.03 (0.13) | 7.56 (0.14) | −0.47 (−0.84 to −0.10) | 0.51 | .01 |
| At 12 w, fully adjusted mean (SE), % | 8.04 (0.13) | 7.56 (0.14) | −0.48 (−0.85 to −0.11) | 0.52 | .01 |
| At baseline, mean (SD), mmol/mol | 61.73 (15.91) | 63.43 (16.82) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE), mmol/mol | 64.31 (1.40) | 59.14 (1.50) | −5.17 (−9.21 to −1.12) | 0.51 | .01 |
| At 12 w, fully adjusted mean (SE), mmol/mol | 64.36 (1.45) | 59.08 (1.52) | −5.28 (−9.34 to −1.23) | 0.52 | .01 |
| SCI-R score | |||||
| At baseline, mean (SD) | 36.54 (5.94) | 35.20 (6.83) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE) | 36.51 (0.62) | 39.68 (0.64) | 3.17 (1.39 to 4.96) | 0.69 | <.001 |
| At 12 w, fully adjusted mean (SE) | 36.40 (0.63) | 39.80 (0.64) | 3.40 (1.61 to 5.19) | 0.75 | <.001 |
| PSS score | |||||
| At baseline, mean (SD) | 23.64 (10.27) | 20.64 (10.32) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE) | 22.03 (1.15) | 19.55 (1.20) | −2.47 (−5.63 to 0.68) | 0.29 | .13 |
| At 12 w, fully adjusted mean (SE) | 22.29 (1.15) | 19.29 (1.19) | −3.00 (−6.20 to 0.20) | 0.36 | .07 |
| SF-36 score | |||||
| At baseline, mean (SD) | 50.16 (21.49) | 50.90 (22.15) | NA | NA | NA |
| At 12 w, baseline-adjusted mean (SE) | 49.02 (2.06) | 57.21 (2.20) | 8.20 (2.47 to 13.93) | 0.56 | .005 |
| At 12 w, fully adjusted mean (SE) | 48.39 (1.97) | 57.84 (2.13) | 9.46 (3.65 to 15.26) | 0.68 | .001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Education · Mobile Health and mHealth Applications · Digital Mental Health Interventions
Introduction
One in 5 older individuals lives with type 2 diabetes, representing over 150 million people worldwide.^1,2^ Managing diabetes is complex, especially in at-risk populations such as older adults, which often experience cognitive decline, functional limitations, polypharmacy, and frailty.^3,4^ Additionally, both diabetes and aging increase the risk of mental health disorders, which in turn can further contribute to lower treatment adherence and poorer glycemic control.^5,6,7,8,9^
Developing new strategies to promote mental health and support diabetes management is crucial, and interactive virtual assistants based on artificial intelligence hold promising opportunities to improve lifestyle management and assist with insulin dosing, as demonstrated in previous studies.^10,11^ These devices are more financially accessible than other electronic ones and can provide continuous and personalized support through a user-friendly, voice-activated interface. This is particularly relevant for older adults, as they often face functional limitations and may lack the fine motor skills required to operate more complex devices.
Given the current lack of evidence regarding the use of these devices as a complementary tool to usual care among older adults with type 2 diabetes, we conducted the IVAM-ED (Interactive Virtual Assistant for Mental Health Promotion and Self-Care Management in Elderly with Type 2 Diabetes) randomized clinical trial. The primary objective of this trial was to determine whether an interactive virtual assistant with a voice interface, built with a behavioral intervention model, could improve mental health and reduce psychological distress among older patients with type 2 diabetes. Secondary objectives were to assess its impact on quality of life, perceived stress, adherence to diabetes self-care behaviors, and glycemic control.
Methods
Study Design
The IVAM-ED trial was a single-center (São Lucas Hospital, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, Brazil), open-label, parallel, 2-group randomized clinical trial investigating an interactive virtual assistant device activated by voice for mental health and diabetes-related self-care compared with usual care. The trial protocol and statistical analysis plan were approved by the Research Ethics Committee of Pontifical Catholic University of Rio Grande do Sul and are presented in Supplement 1.^12^ All participants provided written informed consent before enrollment. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Participants
We enrolled older adults (aged ≥65 years) with type 2 diabetes residing in Porto Alegre or the metropolitan region with a Wi-Fi connection at home, who received outpatient care at São Lucas Hospital. Enrollment occurred between June 22, 2023, and February 8, 2024, and the last patients completed the trial in May 2024. A detailed description of the recruitment procedures is provided in the study protocol (Supplement 1).^12^ Key exclusion criteria included having an interactive virtual assistant device and presenting severe hearing or cognitive impairments at the time of enrollment. A full list of the eligibility criteria is provided in eAppendix 1 in Supplement 2.
Randomization and Blinding
Participants who met the eligibility criteria attended an initial study visit (week −1), in which they signed a consent form and had baseline data collected. At the end of the visit, they were randomly assigned in a 1:1 ratio using a computer-generated simple random sequence without stratification or blocking to receive the interactive virtual assistant device (Smart Speaker Echo Dot, 3rd generation [Amazon]) for home use for 12 weeks or to continue with usual care. All randomization procedures were conducted by an independent researcher (J.A.) and revealed by standard text message at the end of the baseline visit. Participants and investigators were blinded until the end of baseline evaluation. The investigator responsible for supervising statistical analysis remained blinded until all study analyses were completed.
Interventions
Intervention Group (Smart Speaker Group)
Participants assigned to the intervention group received the smart speaker for home use. The device was installed during a home visit by the research team 7 days (±7 days) after the baseline assessment. It was programmed using a standard multicomponent behavioral intervention model, featuring automatic interactions for medication and glucose test reminders, health tips, and educational podcasts to improve diabetes management and mental health. The behavioral intervention was developed by a multidisciplinary diabetes care group specifically for this study and was implemented using the device’s native reminder function for medication and glucose-test alerts, together with a custom Alexa Skill designed to automatically deliver the daily health tips and weekly podcast components of the intervention. A user manual, containing information on the device’s main commands (eg, “Alexa, play music”), was provided to encourage the use of native device functions. Detailed content and frequency of each health tip and podcast episode are available in the study protocol (Supplement 1).^12^
Control Group (Usual Care)
Individuals assigned to the usual care group were instructed to maintain their usual care routine. Additionally, they received a booklet with general health information and guidance on accessing a webpage, created by the research team, in which they could listen to the podcast episodes and view the health tips that were automatically provided through the smart speaker to participants in the intervention group. The booklet was provided to standardize the information given to participants in both the intervention and usual care groups.
Follow-Up Phone Calls
All participants enrolled in the study received 5 follow-up phone calls, conducted every 2 weeks. The main goal of the calls was to prevent dropouts and monitor adverse events. No motivational interventions were conducted. To ensure equal contact across groups and to minimize potential bias, participants in the usual care group received an additional call at week 0, corresponding to the device installation.
Study Procedures and Timeline
Participants attended 2 in-person visits at the Clinical Research Center of São Lucas Hospital as part of the study: the baseline evaluation (week −1) and the final evaluation at the end of the intervention period (week 12). Sociodemographic characteristics were assessed at baseline and were self-reported. Outcomes were assessed at both visits by a trained member of the research team (L.S.M., F.L.d.C., L.G.B.d.B., V.G., I.S.M., L.M.B., and M.A.B.B.). The intervention period began at week 0, marked by the device installation (intervention group) or the additional phone call (usual care group). A comprehensive study timeline with specific items evaluated during each visit is provided in the study protocol (Supplement 1).^12^
Diabetes management, including medication adjustments, was provided by participants’ usual health care team and occurred independently of the study procedures. As part of the trial, no additional cointerventions were implemented beyond the predefined study components. Consistent with the pragmatic design of the trial, no motivational strategies or adherence support were delivered to sustain engagement with the smart speaker intervention.
Outcomes
Primary Outcome
The prespecified primary outcome was the between-group mean difference (MD) in mental distress at the 12-week follow-up, accessed using the Brazilian version of the Self-Reporting Questionnaire (SRQ-20).^13^ The SRQ-20 score assesses depression, anxiety, and other common mental health disorder symptoms during the month preceding the evaluation. The total score ranges from 0 to 20, with higher scores indicating greater mental distress.
Secondary Outcomes
Prespecified secondary outcomes included the between-group MDs at the 12-week follow-up in quality of life, assessed using the 36-Item Short Form Health Survey, in which scores range from 0 to 100 in each of 8 domains, with higher scores indicating greater quality of life; adherence to diabetes self-care behaviors, assessed using the Self-Care Inventory Revised questionnaire, in which scores range from 11 to 55, with higher scores indicating a higher level of care related to diabetes; perception of stress, assessed using the Perceived Stress Scale, in which scores range from 0 to 56, with lower scores indicating a reduced level of stress; and glycemic control (hemoglobin A_1c_ [HbA_1c_]). Additional secondary outcomes included lipid profile (total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglyceride levels) and blood pressure (systolic and diastolic). All surveys were previously validated to the study population.^14,15,16^ A detailed description of each outcome is provided in eAppendix 2 in Supplement 2.
Sample Size
For the primary outcome, the study target sample size was 112 (56 per group). This was calculated using a 2-sample t test framework, assuming 90% power, an α level of .05, a 1:1 allocation ratio, a 20% dropout rate, and an anticipated effect size of 0.68 (Cohen d). The effect size was based on a similar trial published by Fulmer et al.^17^
Statistical Analysis
Study Outcomes
Primary and secondary end point analyses were conducted including all randomized participants, analyzed as randomized. Missing outcome data at 12 weeks were imputed using multiple imputation by chained equations with 5 imputations, assuming data were missing at random. As all variables were continuous, linear regression models were used for imputation. As the study was pragmatic in nature, adherence to the intervention was not considered for the analyses.
To assess the impact of the intervention, between-groups pairwise comparisons of the final mean of each outcome variable at 12 weeks were conducted using analysis of covariance. Two analysis of covariance models (baseline-adjusted model and fully adjusted model) were performed as prespecified in the statistical analysis plan. Both models included randomization as a fixed factor and the outcome variable as the dependent variable. For the baseline-adjusted model, the baseline value of the corresponding outcome variable was included as a covariate. The fully adjusted model included age, sex, years of education, individual income, and Mini-Mental State Examination score, in which scores range from 0 to 30, with higher scores indicating better cognitive performance, alongside the baseline value of the outcome variable to account for potential imbalances between groups.
Parameter estimates and their corresponding 95% CIs were pooled across the 5 imputed datasets according to Rubin rules and calculated using robust SE estimation. Baseline-adjusted and fully adjusted MDs at 12 weeks, along with their respective 2-sided 95% CIs and P values, were reported for each outcome. No adjustments were made for multiple comparisons, and statistical significance was considered at an α level of .05. All statistical analyses were performed using SPSS Statistics, version 27.0.1 (IBM Inc).
The effect size for all end points was reported as standardized MDs. Given the large number of secondary outcomes and the lack of adjustment for multiple comparisons, secondary end points should be considered only for hypothesis generation.
Sensitivity Analysis
Seven subgroup analyses were conducted for the primary outcome: sex (male vs female), age (<75 years vs ≥75 years), educational level (primary or less vs secondary or higher), cognitive decline (present vs absent, based on the Mini-Mental State Examination score with education-adjusted cutoffs), insulin use (yes vs no), history of depression (yes vs no), and history of anxiety (yes vs no). Six subgroup analyses were prespecified in the study protocol, and an additional unplanned analysis of history of anxiety was included due to its high prevalence in the sample. The age cutoff was originally set at 80 years, but this was changed to 75 years due to the low number of participants aged 80 years or older. Similarly, the educational-level category was adjusted from graduate to secondary education, given the small number of participants with a graduate degree. Formal comparisons between subgroups were not performed, and P values were not reported.
In addition to the subgroup analyses, 2 prespecified sensitivity analyses were performed using different methods for handling missing data: (1) a baseline observation carried forward approach and (2) a complete-case analysis excluding participants with missing outcome data. These analyses aimed to assess the impact of missing data on the study outcomes.
Results
Study Participants
Between June 22, 2023, and February 8, 2024, a total of 112 participants (56 per group; mean [SD] age, 72.5 [5.7] years; 71 females [63.4%] and 41 males [36.6%]) were randomized (Figure 1). Overall, 103 participants (92.0%) completed the trial and had the final outcome assessments (52 in the intervention group and 51 in the usual care group). Reasons for nonattendance at the 12-week follow-up included being lost to follow-up (6 participants) and death (3 participants). None of the participants withdrew from the study. Baseline demographic and clinical characteristics were similar across study groups (Table 1 and eTables 1 and 2 in Supplement 2) and between participants with and without missing outcome data (eTable 3 in Supplement 2).
Participant Flow Diagram for the IVAM-ED (Interactive Virtual Assistant for Mental Health Promotion and Self-Care Management in Elderly with Type 2 Diabetes) Trial
The mean (SD) HbA_1c_ level was 7.9% (1.5%) (to convert percentage of total hemoglobin to proportion of total hemoglobin, multiply by 0.01), and the mean (SD) duration of diabetes was 16.9 (11.6) years, with 68.8% of participants living with diabetes for 10 years or more. The socioeconomic level of participants was low, as the mean (SD) individual income was 2.3 (2.4) Brazilian minimum wages per month, and 24.1% of participants had completed secondary education or higher.
Mental Distress
The baseline-adjusted mean (SE) SRQ-20 score at the end of the intervention period was 6.39 (0.45) for the smart speaker group and 7.66 (0.43) for the usual care group. Pairwise comparisons between groups at 12 weeks revealed an MD of −1.28 (95% CI, −2.51 to −0.04; P = .04) (Table 2). The difference remained significant after adjusting for sociodemographic variables, with a fully adjusted mean (SE) SRQ-20 score of 6.29 (0.44) for participants in the intervention group and 7.75 (0.42) for those in the usual care group (MD, −1.46 [95% CI, −2.73 to −0.19]; P = .02), suggesting a reduction in mental distress among participants who used the smart speaker and a positive impact of the intervention on mental health.
Quality of Life and Stress
Evaluation of quality of life at 12 weeks showed that participants randomized to the smart speaker group had higher 36-Item Short Form Health Survey scores after the intervention period, with a fully adjusted MD of 9.46 (95% CI, 3.65 to 15.26; P = .001), indicating an improvement in quality of life (Table 3). Stress levels, as measured by the Perceived Stress Scale, were not statistically significantly lower in the smart speaker group (fully adjusted MD, −3.00 [95% CI, −6.20 to 0.20]; P = .07).
Diabetes-Related Outcomes, Blood Pressure, and Lipid Profile
At the 12-week follow-up, participants from the smart speaker group presented a higher score on the Self-Care Inventory Revised, with a fully adjusted MD of 3.40 (95% CI, 1.61 to 5.19; P < .001), suggesting a greater adherence to diabetes-related self-care behavior (Table 3). They also presented lower HbA_1c_ levels, with a fully adjusted mean (SE) HbA_1c_ level at 12 weeks of 7.56% (0.14%) (59.08 [1.52] mmol/mol) in the intervention group compared with 8.04% (0.13%) (64.36 [1.45] mmol/mol) in the usual care group. The fully adjusted MD was −0.48% (95% CI, −0.85 to −0.11; P = .01), indicating a significant reduction in the HbA_1c_ level among participants in the intervention group and better glycemic control (Table 3). No significant differences were observed in blood pressure and levels of total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, or triglyceride concentrations between the groups (eTable 4 in Supplement 2).
Sensitivity Analysis
Stratified fully adjusted analyses for the primary outcomes showed consistent improvements favoring the smart speaker group across all subgroups. Greater MDs were observed among female participants (−1.98 [95% CI, −3.82 to −0.15]), those of younger age (−1.93 [95% CI, −3.48 to −0.37), those without a positive screening for cognitive decline (−3.27 [95% CI, −5.11 to −1.43]), and those with a history of anxiety (−3.72 [95% CI, −6.17 to −1.28]) (Figure 2). However, formal statistical comparisons were not performed between or within subgroups. Sensitivity analyses using different methods for handling missing data yielded similar results to the main analyses carried using multiple imputation (eTables 5 and 6 in Supplement 2).
Forest Plot of the Stratified Analysis by Subgroups for the Primary OutcomeMean difference represents between-group pairwise comparisons using an analysis of covariance model with baseline data of the Self-Reporting Questionnaire score (in which scores range from 0 to 20, with higher scores indicating greater mental distress), age, sex, educational level, income, and Mini-Mental State Examination (MMSE) score as covariates. In the stratified analyses by sex, age, educational level, and cognitive decline, the corresponding covariates (age, sex, educational level, and MMSE) were excluded from each model as appropriate. The model included all enrolled participants, with missing data replaced using multiple imputation. No statistical tests were performed to compare specific subgroups, as prespecified in the statistical analysis plan, because no adjustments for multiplicity were applied. Estimates and 95% CIs are reported for hypothesis-generating purposes only.
Adverse Events
There were no adverse events reported in this study. During follow-up, no participants reported adverse events or severe hypoglycemia episodes in either group. Only 1 participant from the intervention group complained about the frequency of automatic device interactions, but it was not sufficient to cause a substantial disturbance. During the trial, 3 patients died from causes not directly related to mental health or diabetes—1 from stroke, another from urinary sepsis, and a third from heart failure decompensation (eTable 7 in Supplement 2).
Discussion
In this randomized clinical trial involving 112 older adults with type 2 diabetes, we demonstrated the effectiveness of an interactive virtual assistant, built with a behavioral intervention model, in reducing mental distress compared with usual care. After 12 weeks, participants in the smart speaker group showed significant improvements in mental distress, with a reduction of −1.46 points on the SRQ-20 scale. The intervention was also associated with enhanced quality of life, better adherence to diabetes self-care behaviors, and improved glycemic control, although the impact on secondary outcomes should be interpreted as exploratory given the absence of multiplicity adjustment.
The improvement in mental distress observed in our study supports the hypothesis that smart speakers can provide emotional support for older people with diabetes. In a qualitative study conducted with patients from the intervention group, nearly 30% of participants reported feelings of humanization toward the device.^18^ This perception of the device as quasi-human may have contributed to the observed improvements in mental distress and quality of life in the IVAM-ED trial.
Beyond mental health and quality of life, the intervention was also associated with increased adherence to diabetes self-care behaviors and improved glycemic control, reflected in a 0.48% reduction in the HbA_1c_ level after 12 weeks of intervention. The continuous support and personalized medication reminders may have contributed to better adherence to diabetes management practices, ultimately improving diabetes-related outcomes. Additionally, the improvement in mental health may have positively influenced diabetes self-care behaviors, as reduced mental distress can enhance both motivation and capacity for disease management.^19^
Although consistent improvements were observed across all subgroups, the benefits for the primary outcome appeared to be greater among females, an important finding given that anxiety and mood disorders have consistently been shown to be more prevalent among women.^20,21^ Also, the greater impact observed among those with a previous history of anxiety and the lower impact among those with a history of depression suggest that the improvements may be more closely related to anxiety symptoms, as individuals with depression may be less engaged with the device due to their depressive mood. Additionally, subgroup analyses revealed that participants with higher educational backgrounds, those without cognitive decline, and those under the age of 75 years appeared to benefit more from the intervention. These findings suggest that older adults with lower educational backgrounds, cognitive limitations, or more advanced age may derive fewer benefits from a smart speaker–based intervention, potentially due to greater challenges in adapting to and engaging with the device.
Smart speakers have been proposed to enhance independent living, reduce loneliness, and support patient self-management, with over 50 studies^22^ demonstrating their feasibility and acceptability in health-related settings, although clinical trials evaluating their effectiveness remain scarce. In this context, the IVAM-ED trial provides novel evidence that a smart speaker–based behavioral intervention can improve mental distress and diabetes-related outcomes among older adults with type 2 diabetes. To our knowledge, it is the first randomized study to evaluate the impact of such an intervention on diabetes management in older adults, highlighting its potential clinical relevance while underscoring the need for further research. Future studies with longer follow-up periods, a larger proportion of participants aged 75 years or older, and device modifications to enhance accessibility for those with cognitive limitations or limited educational backgrounds could provide valuable insights into the intervention’s impact across a broader older population.
Limitations
This study has limitations. First, the nature of the intervention required an open-label design, which could introduce performance, detection, and response bias. Follow-up phone calls were conducted to help mitigate performance bias, and similar dropout rates across study groups support internal validity. Systematic training of the research team was implemented to reduce detection and response bias, and the improvement in HbA_1c_ level, an objective outcome not subject to participant or assessor influence, reinforces the validity of the study’s findings. Second, the intervention period was short, which could have led to an overestimation of the intervention’s effect size, as the impact of behavioral interventions tends to decline with longer follow-up periods. Third, the study’s inclusion criteria requiring a Wi-Fi connection at home may have selected participants more familiar with technology and therefore more likely to interact with the device and benefit from it, although only a small proportion of participants assessed for eligibility lacked Wi-Fi at home. Additionally, our study included participants from a middle-income country, recruited at a single study site, with low income and limited educational background, which may further limit the generalizability of the findings.
Conclusions
This randomized clinical trial found that an interactive virtual assistant device, built with a behavioral intervention model, improved mental distress among older individuals with type 2 diabetes compared with standard care. Exploratory analyses also suggested improvements in quality of life, adherence to diabetes-related self-care behaviors, and glycemic control. These findings suggest that this easily implemented self-management intervention could significantly enhance health outcomes in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World population prospects 2022: summary of results. United Nations. 2022. Accessed November 10, 2024. https://digitallibrary.un.org/record/3989515
- 2IDF Diabetes Atlas. 10th ed. International Diabetes Federation; 2021. Accessed November 10, 2024. https://diabetesatlas.org/media/uploads/sites/3/2025/02/IDF_Atlas_10th_Edition_2021.pdf
- 3Lee SH. The growing challenge of diabetes management in an aging society. Diabetes Metab J. 2023;47(5):630-631. doi:10.4093/dmj.2023.027937793980 PMC 10555539 · doi ↗ · pubmed ↗
- 4American Diabetes Association Professional Practice Committee. 13. Older adults: standards of care in diabetes—2024. Diabetes Care. 2024;47(suppl 1):S 244-S 257. doi:10.2337/dc 24-S 013 38078580 PMC 10725804 · doi ↗ · pubmed ↗
- 5Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney RM, Clouse RE. Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care. 2000;23(7):934-942. doi:10.2337/diacare.23.7.934 10895843 · doi ↗ · pubmed ↗
- 6Sartorius N. Depression and diabetes. Dialogues Clin Neurosci. 2018;20(1):47-52. doi:10.31887/DCNS.2018.20.1/nsartorius 29946211 PMC 6016052 · doi ↗ · pubmed ↗
- 7Chae WR, Kohring C, Rohde C, Köhler-Forsberg O, Otte C, Holstiege J. Eight-year nationwide study of the bidirectional association between type 2 diabetes and depression in nearly 8 million German outpatients. BMJ Open Diabetes Res Care. 2024;12(3):e 003903. doi:10.1136/bmjdrc-2023-003903 38719506 PMC 11085903 · doi ↗ · pubmed ↗
- 8Zenebe Y, Akele B, W/Selassie M, Necho M. Prevalence and determinants of depression among old age: a systematic review and meta-analysis. Ann Gen Psychiatry. 2021. doi:10.1186/s 12991-021-00375-x 34922595 PMC 8684627 · doi ↗ · pubmed ↗