Prolonged Flow-Controlled Ventilation in a Patient With ARDS and Multiple Trauma: A Case Report
Romana Erblich, Wolfgang Puchner, Matthias Noitz, Marius Knöll, Bernhard Eichler, Stephan Kalb, Dominik Jenny, Thomas Tschoellitsch, Jens Meier, Martin W. Dünser

TL;DR
A 30-year-old patient with severe trauma and ARDS improved using flow-controlled ventilation when conventional methods failed.
Contribution
Demonstrates the potential of flow-controlled ventilation as a novel treatment for ARDS in complex trauma cases.
Findings
Flow-controlled ventilation improved oxygenation and reduced intracranial pressure quickly.
Lower minute volumes with FCV achieved better ventilation than conventional methods.
FCV was used for 96 hours without complications, suggesting its feasibility in critical cases.
Abstract
Flow-controlled ventilation (FCV) is characterized by a bidirectional linearized gas flow translating into a constant flow. We report the prolonged use of FCV in a 30-year-old patient with major trauma, including severe traumatic brain injury and posttraumatic ARDS, because the patient sustained other severe injuries such as those to the spine and pelvis. Conventional mechanical ventilation failed to attain normoxia and normocapnia, leading to hemodynamic compromise and refractory intracranial hypertension. FCV was used as an off-label rescue therapy because prone positioning and extracorporeal membrane oxygenation were contraindicated. Within a few hours, ventilation improved despite lower minute volumes. This was paralleled by a reduction in norepinephrine requirements and normalization of intracranial pressure. FCV was continued for 96 hours. This case report underlines the potential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
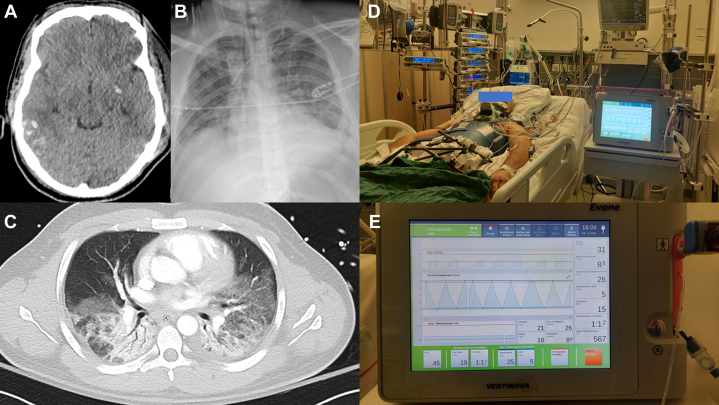 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Traumatic Brain Injury and Neurovascular Disturbances · Airway Management and Intubation Techniques
Flow-controlled ventilation (FCV) is characterized by a bidirectional linearized gas flow translating into a constant flow during inspiration and expiration. Differences between FCV and conventional mechanical ventilation include no pause phases during the respiratory cycle and direct measurement of airway pressures in the trachea.1^,^2 FCV is used commonly for intraoperative ventilation when small-bore endotracheal tubes are required.3 In these settings, FCV allows for adequate ventilation with minute volumes and driving pressures in the normal range.3 Compared with volume-controlled ventilation, FVC improves lung aeration and respiratory system compliance.4, 5, 6 In 2 porcine ARDS models, FCV improved oxygenation and CO_2_ removal with lower minute volumes and similar inspiratory pressures than volume-controlled or pressure-controlled ventilation.7^,^8 FCV was associated with an increase in normally aerated lung volumes, fewer signs of ventilator-induced lung injury,7 and faster hemodynamic stabilization.8 To date, only 2 small studies have evaluated the short-term (30 min and 4 hours) effects of FCV in patients with COVID-19-associated ARDS. During FCV, oxygenation and ventilation remained stable despite lower respiratory rates, peak inspiratory pressures, and minute volumes than with conventional mechanical ventilation.9^,^10 Herein, we report the first so far published, to our knowledge, clinical use of FCV in a patient with ARDS for > 24 hours.
Case Report
A 30-year-old White man (height, 170 cm; weight, 80 kg) was admitted with severe injuries: traumatic brain injury (Glasgow Coma Scale score, 4 points; multiple contusions and intracerebral and subarachnoid hemorrhages) (Fig 1A), unstable cervical spine fractures, bilateral rib fractures, bilateral lung contusions, subcapsular splenic hematoma, renal contusion, unstable pelvic ring fracture, and lower extremity fractures. The injury severity score was 59 points. After resuscitation, external fixation of the pelvis was performed emergently and an intracranial pressure (ICP) monitoring device was introduced. Despite cardiorespiratory stabilization, the absence of an intracranial hematoma amenable to surgical evacuation, deep multimodal sedation, osmotherapy, and normothermia, ICP peaked up to 25 mm Hg. Forty-eight hours after trauma, right-sided decompressive hemicraniectomy was performed. Simultaneously, a progressive deterioration in respiratory function required higher ventilator support with increasing inspiratory oxygen concentrations and minute volumes to attain normoxia and normocapnia. On day 3, ARDS had developed (Figs 1B, 1C, Table 1).11 Within a few hours, Paco_2_ rose to 68 mm Hg, triggering ICP plateaus of up to 26 mm Hg. Norepinephrine requirements had increased to 0.46 μg/kg/min to maintain cerebral perfusion pressure at 55 to 60 mm Hg. Prone positioning was contraindicated because of the unstable cervical spine injury and intracranial hypertension, as was venovenous extracorporeal membrane oxygenation because of intracranial hemorrhages and an increased overall bleeding risk. As a rescue therapy, mechanical ventilation was switched from pressure-controlled ventilation (Hamilton C6; Hamilton Medical) to FCV using a dedicated ventilator (Evone; Ventinova Medical) (Figs 1D, 1E). The endotracheal tube (inner diameter, 8.0 mm) was connected to the ventilator system using the conventional tube adapter (Evone Conventional Tube Adapter; Ventinova Medical), and the pressure monitoring catheter was introduced up to the tip of the endotracheal tube. As suggested in a previous study,12 FCV settings were individualized by compliance-guided positive end-expiratory pressure and peak pressure titration. Within 3 hours, the partial arterial oxygen and Paco_2_ improved, despite lower minute volumes (Table 1). Norepinephrine requirements decreased and ICP consistently fell to < 23 mm Hg. FCV was continued for 96 hours until ventilator lung function and ICP had stabilized, although this exceeded the maximum approved time for use of the FCV ventilator (< 72 hours). The patient then was switched back to pressure-controlled ventilation using a standard ventilator (Hamilton C6). Definitive surgical procedures (cervical spine stabilization, pelvic ring osteosynthesis) and tracheostomy were performed subsequently. The ensuing hospitalization was complicated by peripheral pulmonary embolism, nosocomial COVID-19, rhabdomyolysis-induced acute kidney injury, and ventilator-associated pneumonia. On day 31 after sustaining trauma, the patient was transferred from the ICU to the rehabilitation unit. At discharge, he was awake, was able to communicate, and exhibited a mild right-sided hemiparesis.Figure 1A-E, Imaging from the 30-year-old White male patient. A, Cerebral CT scan exhibiting brain edema, subarachnoid, and intracerebral hemorrhages. B, C, Chest radiograph (B) and CT scan (C) with features of ARDS. D, Photograph showing ICU setup. E, Photograph showing and flow-controlled ventilator (Evone; Ventinova Medical).Table 1. Course of Ventilator Settings, Gas Exchange, and Other Clinical Parameters Before and During FCVVariablePCVFCV Time Point (h)31224487296Ventilation settings Inspiratory flow, L/min65191919201920 Fio_2_0.70.40.40.550.650.550.6 PEEP, mbar12857888 Peak pressure, mbar28302730333030 Tidal volume, mL430550605560640630680 Compliance, mL/mbar27262625232527 Resistance, mbar/L/s89119NANANA Respiratory rate, beats/min25151415141413 Minute volume, L/min10.88.68.88.98.98.88.9 Mechanical power, J/mina21161616191818Gas exchange Pao_2_ to Fio_2_ ratio114191195127116152148 Paco_2_, mm Hg68444046464544 pH7.267.397.417.357.367.427.47Other clinical parameters ICP, mm Hg24222220181412 Heart rate, beats/min1011079394908796 Mean arterial pressure, mm Hg91748569897797 Norepinephrine dose, μg/kg/min0.460.310.320.390.330.190FCV = flow-controlled ventilation; ICP = intracranial pressure; NA = not available; PCV = pressure-controlled ventilation; PEEP = positive end-expiratory pressure.aCalculated according to the following formula: 0.098 × respiratory rate × tidal volume (L) × (peak pressure – 0.5 × [plateau pressure – PEEP]).11
Discussion
In this patient with ARDS, FCV was used as an off-label rescue therapy over 96 hours and delivered through a standard size endotracheal tube, because both prone positioning and extracorporeal membrane oxygenation were considered contraindicated. Within a short period of FCV, we observed a substantial improvement in ventilation and CO_2_ elimination, possibly resulting from better lung aeration and reduced dead space.4, 5, 6 Consecutive improvements in ICP and hemodynamic function paralleled the reversal of hypercapnia. Interestingly, oxygenation improved only moderately during FCV, whereas lung compliance remained unchanged. Although peak inspiratory pressures during FCV were higher than during pressure-controlled ventilation, mean airway pressures were probably lower, given that both peak and end-expiratory pressures during FCV are maintained only for very short moments during the respiratory cycle. Accordingly, the mechanical power delivered during FCV in this patient was approximately 25% lower than during conventional pressure-controlled ventilation. This finding is in line with results of prior studies.10
FCV also was associated with disadvantages in this patient. First, endotracheal suctioning was possible only when the ventilator circuit was disconnected and the pressure monitoring catheter was removed partially. Second, the patient required the maximum inspiratory flow rate that the FCV ventilator was able to deliver to achieve a sufficient minute ventilation. No safety margin was left. Furthermore, operation of the FCV ventilator resulted in a relevant noise level perceived as disturbing by other patients and staff. Although not immediately pertinent to this patient, who required deep sedation because of intracranial hypertension, the FCV ventilator would have not allowed for spontaneous or assisted ventilation.
This case report underlines the potential benefits of FCV as a novel ventilation method in patients with ARDS and justifies future studies evaluating the outcome effects of FCV in this population with complex injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hamaekers A.E.W.Götz T.Borg P.A.J.Enk D.Achieving an adequate minute volume through a 2 mm transtracheal catheter in simulated upper airway obstruction using a modified industrial ejector Br J Anaesth 104320103823862010069710.1093/bja/aep 391 · doi ↗ · pubmed ↗
- 2Barnes T.van Asseldonk D.Enk D.Minimisation of dissipated energy in the airways during mechanical ventilation by using constant inspiratory and expiratory flows—flow-controlled ventilation (FCV)Med Hypotheses 12120181671763039647410.1016/j.mehy.2018.09.038 · doi ↗ · pubmed ↗
- 3Schmidt J.Günther F.Weber J.Flow-controlled ventilation during ear, nose and throat surgery: a prospective observational study Eur J Anaesthesiol 36520193273343073042210.1097/EJA.0000000000000967 · doi ↗ · pubmed ↗
- 4Schmidt J.Günther F.Weber J.Glottic visibility for laryngeal surgery: tritube vs. microlaryngeal tube: a randomised controlled trial Eur J Anaesthesiol 361220199639713164451410.1097/EJA.0000000000001110 PMC 6855316 · doi ↗ · pubmed ↗
- 5Weber J.Straka L.Borgmann S.Schmidt J.Wirth S.Schumann S.Flow-controlled ventilation (FCV) improves regional ventilation in obese patients—a randomized controlled cross-over trial BMC Anesthesiol 2012020243199221310.1186/s 12871-020-0944-y PMC 6986135 · doi ↗ · pubmed ↗
- 6Weber J.Schmidt J.Straka L.Wirth S.Schumann S.Flow-controlled ventilation improves gas exchange in lung-healthy patients—a randomized interventional cross-over study Acta Anaesthesiol Scand 64420204814883182875510.1111/aas.13526 · doi ↗ · pubmed ↗
- 7Schmidt J.Wenzel C.Spassov S.Flow-controlled ventilation attenuates lung injury in a porcine model of acute respiratory distress syndrome: a preclinical randomized controlled study Crit Care Med 4832020 e 241e 2483185600010.1097/CCM.0000000000004209 PMC 7017946 · doi ↗ · pubmed ↗
- 8Abram J.Martini J.Spraider P.Individualised flow-controlled versus pressure-controlled ventilation in a porcine oleic acid-induced acute respiratory distress syndrome model Eur J Anaesthesiol 40720235115203674904610.1097/EJA.0000000000001807 PMC 10256303 · doi ↗ · pubmed ↗