Prognostic value of the ratio of globally sclerotic glomeruli in patients with idiopathic IgA nephropathy
Sinan Kazan, Savaş Öztürk, Müge Uzerk Kibar, Seyda Gul Ozcan, Raife Dilhan Alcelik Karacan, Necmi Eren, Mahmut Gok, Kultigin Turkmen, Hamad Dheir, Taner Basturk, Erhan Tatar, Omer Faruk Akcay, Meltem Gürsu, Hakki Arikan, Sena Ulu, Mehmet Deniz Ayli, Ilhan Kurultak

TL;DR
This study shows that the ratio of globally sclerotic glomeruli in kidney biopsies can predict long-term outcomes in patients with IgA nephropathy.
Contribution
The study identifies a specific RoGSG threshold (28.86%) as a strong predictor of adverse kidney outcomes in IgA nephropathy.
Findings
A RoGSG cutoff of 28.86% predicted adverse outcomes with high accuracy (AUC 0.917).
High RoGSG was an independent predictor of adverse outcomes alongside other factors like tubular atrophy and treatment response.
The prognostic value of RoGSG was consistent across key subgroups, including those with nephrotic syndrome.
Abstract
IgA nephropathy (IgAN) is the most common primary glomerulonephritis worldwide. We assessed whether the Ratio of Globally Sclerotic Glomeruli (RoGSG) on diagnostic biopsy predicts subsequent kidney outcomes in a nationwide, multi‑center registry. Among 326 adults with idiopathic IgAN (mean age 39.1 ± 12.8 years; 60.1% male), 43 patients (13.2%) met a 5 year composite outcome defined as any of: doubling of serum creatinine or ≥ 50% decline in eGFR from baseline, eGFR < 15 mL/min/1.73 m2, or initiation of kidney replacement therapy. Receiver operating characteristic analysis identified a RoGSG cutoff of 28.86% for predicting the composite outcome (AUC 0.917, 95% CI 0.885–0.949; sensitivity 93.0%; specificity 84.5%). Using this threshold, 47.6% of patients with RoGSG ≥ 28.86% versus 1.2% with RoGSG < 28.86% reached the composite outcome. In multivariable models adjusted for clinical and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
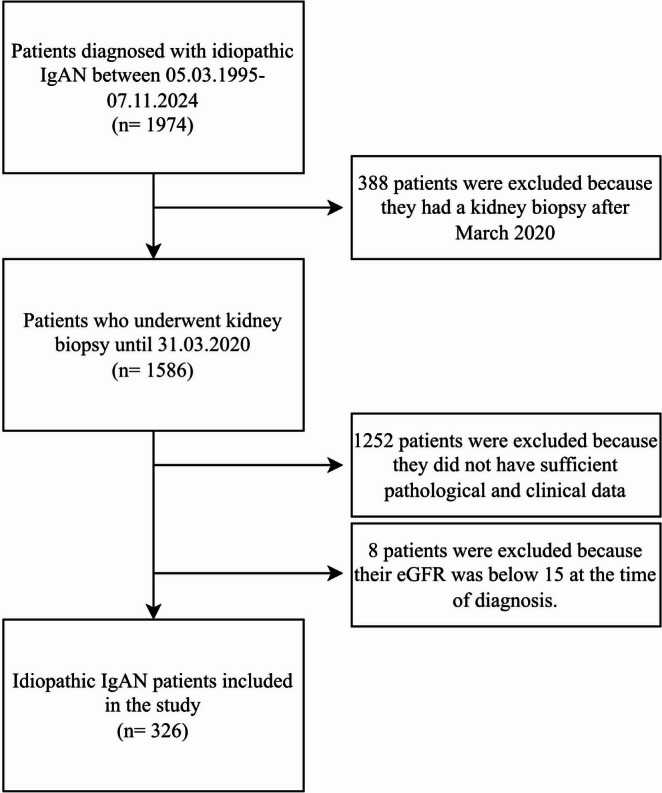 Figure 1
Figure 1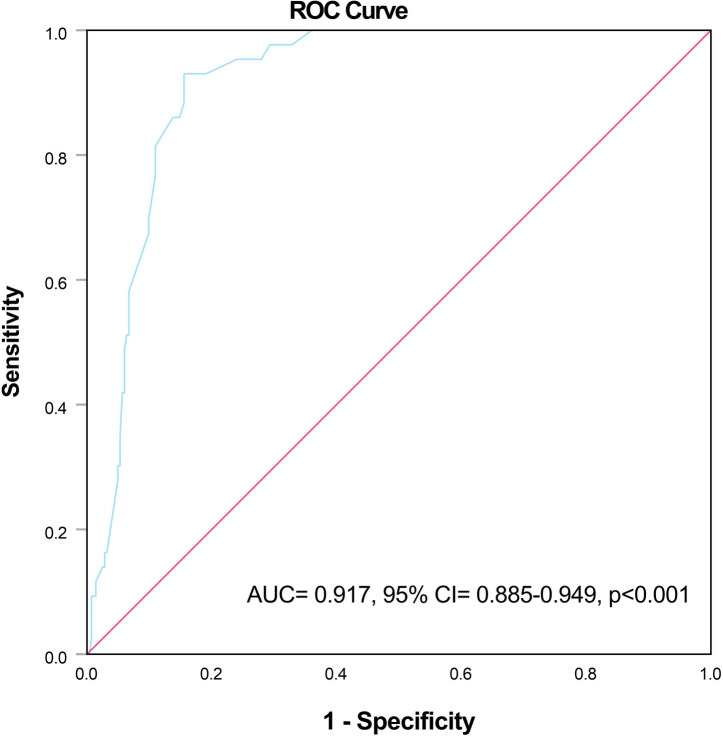 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Diseases and Glomerulopathies · Chronic Kidney Disease and Diabetes · Vasculitis and related conditions
Introduction
IgA nephropathy (IgAN) is the most common primary glomerulonephritis both in Turkey and worldwide^1,2^. Although it generally exhibits a relatively mild course compared to other glomerular diseases, it can progress to kidney failure (KF) in patients with certain clinical, laboratory, and pathological risk factors. Poor prognostic factors include demographic features such as advanced age, race, and hypertension; laboratory findings such as the presence and severity of proteinuria and low estimated glomerular filtration rate (eGFR) at diagnosis; and pathological features described by the Oxford classification (MEST‑C score), including mesangial hypercellularity, endocapillary hypercellularity, segmental sclerosis, tubular atrophy/interstitial fibrosis, and crescents^3^.
Global glomerulosclerosis is a marker of irreversible kidney damage and reduced kidney reserve. As sclerosis develops in some glomeruli, the functional burden on the remaining intact glomeruli increases, resulting in an elevated single‑nephron GFR^4^. Increased single‑nephron GFR may also lead glomerulosclerosis^5^. Glomerulosclerosis is considered a histopathological finding of chronicity in patients with IgAN and is one of the indicators of progression^6^. The Ratio of Globally Sclerotic Glomeruli (RoGSG) to the total number of glomeruli reflects the extent of irreversible parenchymal injury. This quantitative parameter, although not included in the Oxford classification, may provide additional prognostic information. Therefore, understanding its association with kidney outcomes may contribute to more accurate risk stratification in patients with IgAN.
In this study, we aimed to investigate the prognostic significance of the RoGSG on kidney outcomes in patients with idiopathic IgAN.
Results
A total of 326 patients with idiopathic IgAN were included. The mean age at diagnosis was 39.1 ± 12.8 years, and 60.1% (n = 196) were male. Hypertension and diabetes mellitus were present in 32.8% and 8.0%, respectively; 16% reported active smoking. Nephrotic syndrome was present in 21.8% (n = 71). Baseline laboratory parameters included median serum creatinine 1.1 mg/dL (IQR 0.8–1.6), BUN 17 mg/dL (IQR 13–25), serum albumin 4.0 g/dL (IQR 3.6–4.3), and spot urine protein‑to‑creatinine ratio 1550 mg/g (IQR 800–3015). Table 1 summarizes baseline features.Table 1. General characteristics of all patients and comparison in terms of composite kidney endpoint status.Composite kidney endpointCharacteristicsAll patients (n = 326)Present (n = 43)Absent (n = 283)pAge at diagnosis, years39.1 ± 12.836.7 ± 12.939.4 ± 12.80.200Male gender, %-n60.1–19667.4–2959–1570.320Hypertension, %-n32.8–10727.9–1233.6–950.492Diabetes, %-n8–264.7–28.5–240.551Active smoker, %-n16–5248.8–2111–31 < 0.001Nephrotic syndrome, %-n21.8–7141.9–1818.7–530.001Immunosuppression, %-n56.4–18465.1–2855.1–1560.250Response to immunosuppression, %-n86.4–15939.3–1194.9–148 < 0.001BUN at diagnosis, mg/dL17 (13–25)23 (16–30)16 (13–24) < 0.001Serum creatinine at diagnosis, mg/dL1.1 (0.8–1.6)1.5 (1–1.8)1.1 (0.8–1.5)0.002Serum albumin, g/dL4 (3.6–4.3)3.6 (3.3–4)4 (3.7–4.4) < 0.001Hemoglobin, g/dL13.3 ± 2.113.3 ± 1.613.3 ± 2.10.818Spot urine protein/creatinine ratio, mg/g1550 (800–3015)2100 (1263–3800)1385 (800–2950)0.034Mesangial hypercellularity, %-nM0M122.4–7377.6–25314–686–3723.7–6776.3–2160.174Endocapillary hypercellularity, %-nE0E178.5–25621.5–7060.5–2639.5–1781.3–23018.7–530.004Segmental sclerosis, %-nS0S156.7–18543.3–14158.1–2541.9–1856.5–16043.5–1230.870Tubular atrophy/interstitial fibrosis, %-nT0T1T257.4–18733.7–1108.9–2918.6–832.6–1448.8–2163.3–17933.9–962.8–8 < 0.001Crescents, %-nC0C1C277.6–25318.7–613.7–1267.4–2923.3–109.3–479.2–22418–512.8–80.065Total number of glomeruli15 (9.8–23)12 (9–18)16 (10–23)0.124Number of globally sclerotic glomeruli2 (1–4)5 (4–8)2 (0–3) < 0.001RoGSG, %12.5 (3.2–29.6)40 (35.7–50)11.1 (0–22.2) < 0.001RoGSG, ratio of global sclerotic glomeruli; BUN, blood urea nitrogen.
Composite renal outcomes
Over 5 years, 43 patients (13.2%) reached the composite outcome. Among them, 62.8% required kidney replacement therapy, 30.2% experienced doubling of serum creatinine, and 7.0% progressed by eGFR < 15 mL/min/1.73 m^2^. Patients who reached the outcome had higher baseline creatinine and BUN, lower albumin, more frequent nephrotic syndrome and active smoking, and lower response rates to immunosuppression (Table 1).
Predictive value of RoGSG
ROC analysis identified a RoGSG cutoff of 28.86% (AUC 0.917, 95% CI 0.885–0.949; p < 0.001; sensitivity 93.0%; specificity 84.5%). When stratified by this threshold, 84 patients (25.8%) were high RoGSG (≥ 28.86%) and 242 (74.2%) were low (< 28.86%). Composite outcome incidence was 47.6% in high versus 1.2% in low RoGSG groups (p < 0.001; Table 2).Table 2. Comparison of the patients in terms of RoGSG groups.RoGSG GroupCharacteristicsLow RoGSG (< 28.86) (n = 242)High RoGSG (≥ 28.86) (n = 84)pAge at diagnosis, years39.01 ± 13.239.18 ± 11.90.823Male gender, %-n58.7–14264.3–540.438Hypertension, %-n30.6–7439.3–330.177Diabetes, %-n7.9–198.3–70.820Active smoker, %-n11.6–2828.6–24 < 0.001Nephrotic syndrome, %-n20.2–4926.2–220.283Immunosuppression, %-n53.7–13064.3–540.098Response to immunosuppression, %-n93.1–12170.4–38 < 0.001BUN at diagnosis, mg/dL16 (12–22)23 (16–30) < 0.001Serum creatinine at diagnosis, mg/dL1.1 (0.8–1.5)1.5 (1.1–1.8) < 0.001Serum albumin, g/dL4 (3.7–4.3)3.9 (3.5–4.2)0.056Hemoglobin, g/dL13.21 ± 2.113.41 ± 1.80.409Spot urine protein/creatinine ratio, mg/g1357 (791–2800)1785 (1075–3771)0.030Mesangial hypercellularity, %-nM0M124.4–5975.6–18316.7–1483.3–700.172Endocapillary hypercellularity, %-nE0E180.2–19419.8–4873.8–6226.2–220.222Segmental sclerosis, %-nS0S158.3–14141.7–10152.4–4447.6–400.372Tubular atrophy/interstitial fibrosis, %-nT0T1T264–15532.6–793.3–838.1–3236.9–3125–21 < 0.001Crescents, %-nC0C1C280.6–19517.8–431.7–469–5821.4–189.5–80.002Composite kidney endpoint, %-n1.2–347.6–40 < 0.001RoGSG, ratio of global sclerotic glomeruli; BUN, blood urea nitrogen.
Subgroup analyses
To explore whether the prognostic effect of high RoGSG (≥ 28.86%) varied across clinically relevant strata, we performed exploratory subgroup analyses according to nephrotic syndrome, response to immunosuppression, smoking status, TA/IFTA grade (T0–T1 vs T2), and dichotomized medians of baseline proteinuria, serum creatinine, and age. For each stratum, event frequencies and unadjusted odds ratios (ORs) were calculated for high versus low RoGSG.
Heterogeneity was assessed using logistic regression models containing a multiplicative RoGSG × subgroup interaction term. Given limited events and multiple testing, these analyses were considered hypothesis-generating.
Regression analyses
In multivariable analysis (Table 3), high RoGSG (≥ 28.86%) and TA/IFTA grade 2 remained independently associated with the composite outcome, whereas other covariates lost statistical significance after adjustment. Non-response to initial immunosuppression was also independently associated with higher risk, consistent with univariate findings.Table 3. Risk factors for composite kidney endpoint.UnivariateMultivariateCharacteristicsOR95% CIpOR95% CIpNephrotic syndrome (vs. absent)3.1251.590–6.140 < 0.0010.7080.043–11.5480.809Active smoking (vs non-smoker)7.7603.835–15.700 < 0.00116.3240.885–301.0970.060Response to immunosuppression (vs. resistant)0.0350.012–0.099 < 0.0010.0140.001–0.3760.011BUN (per mg/dL)1.0001–1.0400.056Creatinine (per mg/dL)1.8051.078–3.0210.0250.1620.009–2.7860.210Protein to creatinine ratio (per mg/g)1.0021.001–1.0050.0080.9990.999–1.0000.135Albumin (per g/dL)0.3170.187–0.547 < 0.0010.1260.013–1.2460.076Endocapillary hypercellularity (vs. E0)2.8371.437–5.6030.00310.7100.786–146.0260.075Segmental sclerosis (vs. S0)0.9370.489–1.7940.843Tubular atrophy/interstitial fibrosis (vs. T0)T1T23.26358.7831.322–8.05319.961–172.8220.010 < 0.0012.64633.9150.223–31.45828.181–408.1800.441 < 0.001High RoGSG (vs. low RoGSG)72.42421.457–244.461 < 0.00133.1826.233–179.1610.004BUN, blood urea nitrogen; RoGSG, ratio of global sclerotic glomeruli.
Discussion
In this multicenter retrospective cohort, a higher RoGSG at diagnosis was strongly associated with adverse 5 year kidney outcomes in idiopathic IgAN, independent of clinical and histopathologic covariates. Our findings complement prior reports linking global glomerulosclerosis with progression and extend them by proposing an empirically derived threshold that may aid clinical risk stratification. Although several scoring and glomerular grading systems have been proposed to predict the prognosis of IgAN, each has its own limitations, and histopathological assessment remains a matter of ongoing discussion^7–10^. In this context, our study aimed to evaluate the predictive value and prognostic significance of RoGSG in relation to kidney outcomes.
Previous studies have consistently demonstrated that histopathological alterations in glomerulonephritis are significantly associated with disease chronicity and poor kidney outcomes. Global glomerulosclerosis is also one of these histopathological changes. Nakakita et al. recently conducted a study including patients with IgAN, and found that the percentage of global glomerulosclerosis was an independent risk factor for poor kidney outcomes in glomerulonephritis, regardless of the underlying disease^11^. Worawichawong et al. reported that global glomerulosclerosis, despite not being part of the Oxford classification, was associated with C4d deposition and unfavorable renal outcomes in patients with IgAN^12^. Nasri et al. reported that proportion of globally sclerotic glomeruli in patients with IgAN was significantly associated with various clinical and histopathological parameters^13^. In their multicenter retrospective study, Zou et al. demonstrated that the global glomerulosclerosis rate was a significant predictor of disease progression in IgAN^14^. Tan et al. found that global glomerulosclerosis may be a prognostic marker in patients with IgA vasculitis and nephritis^15^. The rate of global sclerosis has not only been investigated in patients with IgAN but also in other glomerulonephritis. Erdogmus et al., based on their 13 year cohort of patients with crescentic glomerulonephritis, identified that a global glomerulosclerosis rate greater than 24% was significantly associated with progression to ESRD^16^. Fakhrjou et al. demonstrated that in primary focal segmental glomerulosclerosis, the proportion of sclerotic glomeruli showed a strong correlation with serum creatinine levels and the degree of tubulointerstitial fibrosis^17^.
More recently, several contemporary studies have further refined prognostic understanding in IgA nephropathy. In a large long-term cohort, even clinically low-risk patients demonstrated substantial progression to kidney failure, emphasizing the need for refined risk stratification^18^. Jiang et al. showed that patients presenting with nephrotic syndrome had markedly worse renal survival, which aligns with our subgroup findings showing that high RoGSG retained prognostic significance even in this group^19^. Shirai S et al. found that even patients with mild proteinuria in IgAN and seemingly favorable baseline clinical status had significantly increased risk of renal progression when presenting with eGFR < 60 mL/min/1.73 m^2^, older age and higher serum IgA levels. This underscores the notion that sole reliance on conventional risk indicators may underestimate future adverse renal outcomes, reinforcing the potential value of additional histopathologic markers such as the RoGSG ratio in our cohort^3^. Our study adds to this growing body of evidence by examining RoGSG in a cohort of different ethnic background and by exploring a possible cutoff value that may aid in future validation efforts.
However, we caution against interpreting 28.86% as a definitive universal cutoff. The threshold was derived and evaluated in the same dataset and requires internal (e.g., bootstrapping) and external validation in independent cohorts before clinical adoption. Accordingly, we present this work as hypothesis‑generating.
Selection and exclusion bias merit emphasis. TSN‑GOLD is a registry drawing primarily from tertiary centers; referred patients may have had more severe disease than those managed locally. Moreover, the registry lacked complete follow‑up for many IgAN entries; our analytic cohort excluded individuals without adequate data, which could bias effect estimates. We could not reliably quantify loss‑to‑follow‑up (LFU) among non‑included patients; thus, we cannot determine whether LFU was random or selective—an acknowledged limitation.
Biopsy acquisition is not standardized across centers. RoGSG may vary by cortical depth (superficial vs. juxtamedullary sampling) and by biopsy adequacy. Although biopsy adequacy was not pre‑specified in TSN‑GOLD and location metadata were not uniformly captured, these factors could influence RoGSG and should be addressed in future prospective studies.
Our subgroup analyses—particularly among patients with nephrotic syndrome and among initial responders—suggest that RoGSG conveys prognostic information beyond early clinical course. We summarize these interactions qualitatively in Supplementary Table S1 to avoid over‑precision not supported by registry granularity. Future work should test interactions formally in larger datasets with standardized treatments and longitudinal covariates (blood pressure, proteinuria).
Finally, while our multivariable model included multiple pathological features, high RoGSG and grade 2 TA/IF retained independent associations with outcome, supporting additive prognostic value. Still, unmeasured confounding remains possible.
Exploratory subgroup analyses (Supplementary Table S1) revealed directionally consistent associations of high RoGSG with the composite outcome across clinical strata, without statistically significant interaction. This suggests that the prognostic contribution of global glomerulosclerosis is relatively uniform across patient subgroups, although the limited event number warrants cautious interpretation.
Although the study has several strengths, certain aspects should be interpreted with caution. The multicenter design and relatively large, well-characterized cohort enhance the generalizability within the registry context, yet the retrospective nature may have introduced inherent biases in patient selection and data collection. In addition, inter-observer variability among centers and lack of prespecified biopsy adequacy could have influenced the consistency of pathological assessment. Age-related changes in global glomerulosclerosis were not adjusted for, which might have affected interpretation. Because of limitations in data capture, time-to-event and competing-risk analyses could not be performed and this is acknowledged as a key limitation, and analyses relied solely on baseline covariates. The RoGSG threshold was derived and evaluated in the same dataset without internal validation, which may have led to optimistic estimates of discrimination. Future work should include internal validation (e.g., bootstrapping, cross-validation) and external validation in prospective cohorts. Moreover, incomplete longitudinal data on treatment, blood pressure, and proteinuria, as well as heterogeneity in management approaches, leave room for residual confounding. Finally, since this registry reflects data from a single country, extrapolation to other populations should be made cautiously.
In summary, our findings suggest that a higher RoGSG at diagnosis is associated with an increased likelihood of adverse kidney outcomes in patients with idiopathic IgAN. This association appeared consistent across key clinical and treatment subgroups. When considered alongside other pathological markers, RoGSG may offer additional insight into prognosis and risk stratification. However, further studies—especially prospective, multiethnic, and externally validated ones—are needed before RoGSG can be incorporated into formal predictive models or clinical decision frameworks.
Material and methods
Patients
This multi‑center study is based on the Turkish Society of Nephrology Primary Glomerular Diseases Registry (TSN‑GOLD) and includes adult patients with biopsy‑proven idiopathic IgAN. To ensure a minimum of 5 years of follow‑up for outcome ascertainment, we included patients who underwent kidney biopsy on or before March 31, 2020 (cutoff chosen to allow complete 5 year follow‑up by March 2025). Patients with eGFR < 15 mL/min/1.73 m^2^ at diagnosis and those lacking adequate pathological or clinical follow‑up data were excluded. A total of 33 institutions contributed cases to this cohort.
Data definitions and timing of measurements
Demographics (age at diagnosis, sex), comorbidities (hypertension, diabetes mellitus), smoking status, presence of nephrotic syndrome, histopathology (Oxford MEST‑C), initiation and response to initial immunosuppressive therapy, and laboratory parameters were recorded. Baseline laboratory values, including serum albumin and hemoglobin, were defined as the closest measurements to the biopsy date within ± 14 days. Response to immunosuppression was defined as partial or complete remission per registry definitions.
Handling of missing data
We performed complete‑case analyses without imputation. Variables with > 10% missingness were not included in multivariable models.
Treatment regimen information
Initial immunosuppression was administered in 56.4% (n = 184). Regimens were categorized as corticosteroids alone, corticosteroids plus cyclophosphamide, calcineurin inhibitors, mycophenolate mofetil, or supportive care only. The majority of patients received steroid-based regimens, whereas alternative immunosuppressive agents were used only in a small subset of cases. Agent-level dosing and duration were not consistently available across all centers in the registry; therefore, regimen-level summaries are provided Figs. 1 and 2.Fig. 1. Flowchart of patient selection. Of 1974 IgAN patients in the registry, 326 met eligibility (biopsy on/before 31 March 2020, adequate data, eGFR ≥ 15 mL/min/1.73 m^2^).Fig. 2ROC curve of RoGSG predicting the composite kidney outcome (AUC 0.917, 95% CI 0.885–0.949; p < 0.001).
Outcome
A composite kidney endpoint was considered as the development of any of the following within the 5 year follow-up period:
- Doubling of serum creatinine or a decrease in eGFR of more than 50% from baseline,
- Reduction in eGFR to less than 15 ml/min/1.73 m^2^,
- Initiation of renal replacement therapy (hemodialysis, peritoneal dialysis, or undergoing kidney transplantation).
RoGSG
The RoGSG was calculated as the percentage of globally sclerotic glomeruli, using the formula: (Number of global sclerotic glomeruli / Number of total glomeruli) × 100.
Ethics approval
All methods were carried out in accordance with relevant guidelines and regulations. The study protocol was reviewed and approved by the Istanbul University Istanbul Faculty of Medicine Clinical Research Ethics Committee at their meeting dated 29.06.2011 with decision number 09. As this was a retrospective analysis of anonymized data from the TSN-GOLD registry, the requirement for informed consent was waived by the ethics committee.
Statistical analyses
All statistical analyses were performed using SPSS version 27.0.1 (IBM Corp., Armonk, NY, USA). Two-sided p < 0.05 considered significant. Categorical variables were summarized as frequencies and percentages. Continuous variables were assessed for normality using the Shapiro–Wilk test and visual inspection of histograms. Normally distributed continuous variables were expressed as mean ± standard deviation (SD), while non-normally distributed variables were reported as median with interquartile range (Q1-Q3).
Patients were divided into two groups according to kidney outcomes: those who developed the composite endpoint and those who did not. Comparisons between groups were made using the chi-square test for categorical variables. The Fisher’s exact test was used in cases where chi-square test requirements were not met. For continuous variables, the independent samples t-test was used when the assumption of normality was met, and the Mann–Whitney U test was applied for non-normally distributed data.
The optimal cutoff value of the RoGSG in predicting the composite kidney outcome was determined using receiver operating characteristic (ROC) curve analysis. The Youden index was used to identify the best threshold. Patients were then reclassified into two groups based on this cutoff value.
Characteristics that were found to differ between patients with and without a composite kidney endpoint were considered as possible risk factors and included in logistic regression analysis. Variables associated with the composite kidney endpoint in univariate analysis were entered into a multivariate logistic regression model to assess their potential as independent risk factors. The enter method was used for multivariate analyses.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barbour, S. J., Coppo, R., Zhang, H., et al. Evaluating a new international risk-prediction tool in Ig A nephropathy [published correction appears in JAMA Intern Med. 2019 Jul 1;179(7):1007. 10.1001/jamainternmed.2019.2030.]. JAMA Intern Med. 2019;179(7):942–952. 10.1001/jamainternmed.2019.060010.1001/jamainternmed.2019.0600 PMC 658308830980653 · doi ↗ · pubmed ↗
- 2Jiang Y, Chen P, Zhao W, et al. Distinct characteristics and prognosis of Ig A nephropathy patients with nephrotic syndrome: a propensity score-matched cohort study. Front Med (Lausanne). 2024 Feb 19;11:1344219. 10.3389/fmed.2024.1344219. Erratum in: Front Med (Lausanne). 2024 Apr 17;11:1400735. 10.3389/fmed.2024.140073510.3389/fmed.2024.1344219 PMC 1091001538439903 · doi ↗ · pubmed ↗