From bench to bedside, blade, and back: FAP expression in juvenile angiofibroma. Potential implications for FAPI-PET/CT imaging and targeted therapy?
Lukas Pillong, Caroline Burgard, Florian Rosar, Betül Demirkol, Rafail Ebner, Maximilian Linxweiler, Alessandro Bozzato, Bernhard Schick, Silke Wemmert

TL;DR
This study shows that FAP is expressed in juvenile angiofibroma, suggesting FAPI-PET/CT imaging could help diagnose and guide treatment for this rare tumor.
Contribution
First study to demonstrate FAP expression in juvenile angiofibroma and validate it with FAPI-PET/CT imaging.
Findings
FAP, Vimentin, and PECAM1/CD31 were consistently expressed in juvenile angiofibroma samples.
FAPI-PET/CT imaging accurately reflected FAP expression patterns in the tumor.
FAP expression varied significantly within and between tumors, indicating heterogeneity.
Abstract
Juvenile angiofibroma (JA) is a rare, benign fibrovascular tumor that predominantly affects adolescent males. The underlying biological mechanisms remain poorly understood. Fibroblast activation protein (FAP), known for its involvement in tumor invasion, matrix remodeling, and angiogenesis, has been implicated in various malignancies but has not been studied in JA so far. We investigated FAP expression in JA samples (N = 19) using real-time (RT)-PCR (N = 10) and immunohistochemistry (N = 18). In addition, Vimentin and PECAM1/CD31 were analyzed to further characterize the tumor microenvironment. For one patient, preoperative FAPI-PET/CT imaging was conducted, and FAP expression was correlated with radiotracer uptake. Postoperative histopathological analyses of the excised tumor were performed to validate the imaging findings. We found consistent expression of FAP, Vimentin and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
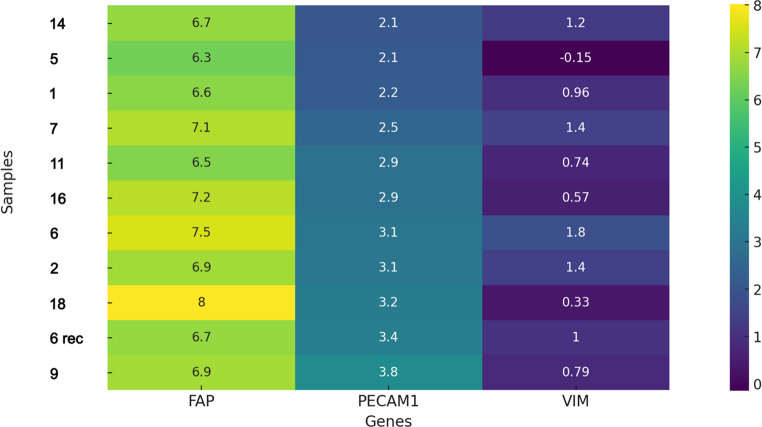 Figure 1
Figure 1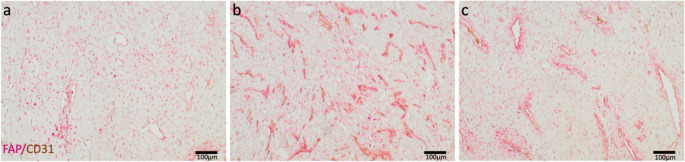 Figure 2
Figure 2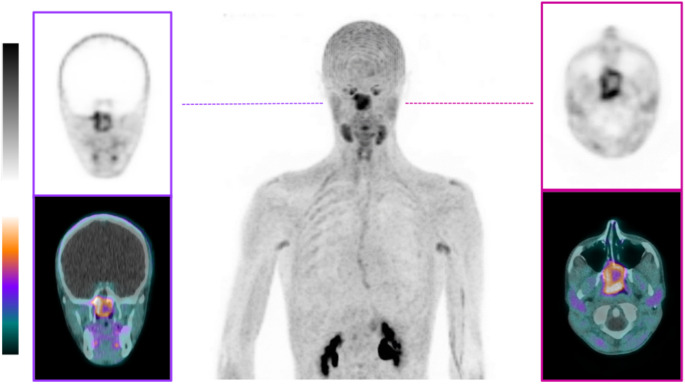 Figure 3
Figure 3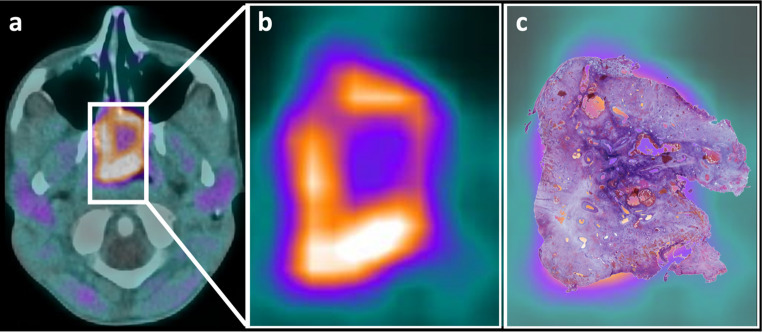 Figure 4
Figure 4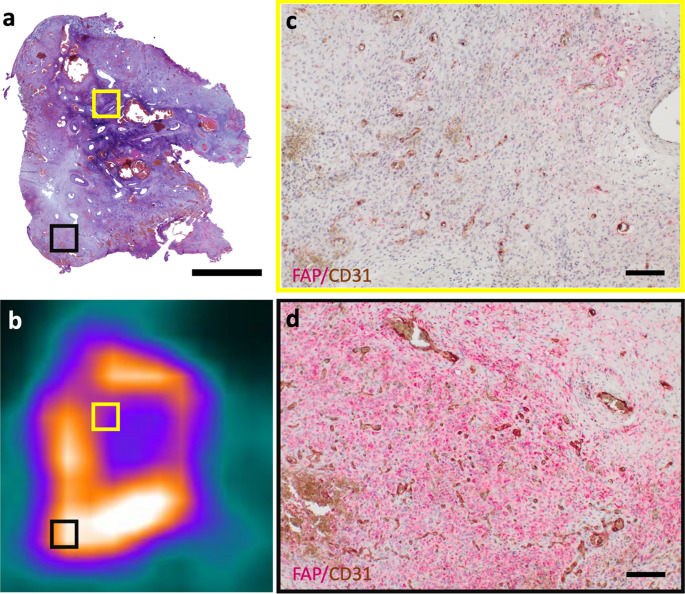 Figure 5
Figure 5- —Universität des Saarlandes (1036)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeptidase Inhibition and Analysis · Cardiac Structural Anomalies and Repair · Protease and Inhibitor Mechanisms
Introduction
Juvenile angiofibroma (JA) is a benign fibrovascular tumor that predominantly affects male adolescents. Recent studies suggest that it originates from persistent neural crest cells [1] at the site of remnants of the first branchial arch near the sphenopalatine foramen [2]. This embryological theory explains the tumor’s specific localization and unique vascular supply.
However, its almost exclusive manifestation in male adolescents suggested a hormonal influence. A study investigating various hormone receptor mRNAs unexpectedly identified luteinizing hormone receptor (LHR) in JAs [3]. Further investigations using in-situ hybridization and immunostaining confirmed LHR expression in JAs associated with pathological blood vessels [4]. As the physiological LH serum levels rise in male puberty, this can explain the sex-specific prevalence of JAs.
Epithelial-mesenchymal transition (EMT), a key process in embryogenesis, may further elucidate the distinct tumor architecture in JAs [1]. Numerous studies support this intriguing theory by identifying various embryological markers, such as laminin alpha 2 [5] and TSHZ1 [6]. Moreover, various growth factors, such as TGF-beta 1 [7] and FGF [8], have been identified, affecting both tumors’ vascular and fibrous components. Given that these are not specific to JAs, potential side effects in other body parts must be considered in therapeutic interventions targeting these growth factors.
In this context, the fibroblast activation protein (FAP) may emerge as an intriguing candidate, particularly intending new therapeutic options in JA treatment. FAP is a membrane-bound serine protease with both dipeptidyl peptidase and endopeptidase activity. While FAP expression is typically low or undetectable in healthy tissue [9, 10], its expression has been implicated not only in multiple malignancies but also in wound healing processes and various diseases such as arthritis [9]. Additionally, fibroblast differentiation [11], extracellular matrix (ECM) remodeling, and also tumor invasion and migration are attributed to FAP. Hence, FAP regulates signaling pathways that promote tumor growth and angiogenesis and was reported to be associated with antitumor immune responses [10].
Consequently, the FAP inhibitor (FAPI) has been effectively utilized in PET/CT diagnostics for a variety of oncological and non-oncological diseases [12, 13]. Hereby, FAPI-PET/CT is particularly valuable for tumor diagnosis, as clinical studies demonstrate its high sensitivity and specificity while providing better image contrast than traditional ^18^F-FDG-PET/CT [12]. The ^68^Ga-FAPI tracer displayed greater sensitivity in identifying primary tumors and metastases across multiple cancer types than ^18^F-FDG-PET/CT. This technology enables significant selective tumor uptake, creating new opportunities for non-invasive tumor characterization [14].
However, the role of FAP in JA has not yet been investigated. In this study, we investigated FAP expression in JA, serving as an interesting and promising target for the diagnosis and treatment of juvenile angiofibroma.
Materials and methods
Tumor specimens
This study analyzed tumor tissue samples from 19 male JA patients aged 11 to 24 (average age 15.8) who were diagnosed and underwent surgery at Saarland University Hospital between 2010 and 2024 (Suppl. Table 1). Written informed consent was obtained from all patients, and human tissue was used according to the Code of Ethics of the World Medical Association (Declaration of Helsinki) and approved by the Institutional Review Board (#218/10) at Saarland University.
Real-time PCR (RT-PCR)
RNA isolation and quantification
Total RNA was isolated from snap-frozen tumor tissue (N = 11) using the RNeasy Mini Kit (Qiagen) according to the manufacturer’s protocol. RNA concentration was quantified with a Nanodrop spectrophotometer, and 100 ng of total RNA was reverse transcribed using the Superscript IV Vilo kit (Thermo Fisher). RT-PCR reactions were carried out in technical triplicates for each primer pair utilizing TaqMan^®^ assays (FAP: Hs00990791_m1; PECAM1/CD31: Hs01065279_m1; Vimentin: Hs00958111_m1; ß2-microglobulin: Hs00187842_m1; Thermo Fisher) on an ABI StepOne Plus™ instrument (Applied Biosystems^®^ Life Technologies). The thermal profile for RT-PCR included a pre-incubation step at 95 °C for 20 s, followed by 40 cycles of denaturation at 95 °C for 1 s and annealing/extension at 60 °C for 20 s.
Normalization and data visualization
The PCR data were normalized using Delta-Ct values calculated relative to the housekeeping gene β2-microglobulin to account for input RNA quantity. To examine the relationships between the gene expression levels of FAP, PECAM1/CD31, and Vimentin, the data were assessed for normality and linearity. FAP, PECAM1/CD31, and Vimentin data showed normal distribution. Linearity occurred only for FAP and PECAM1/CD31, permitting Pearson’s correlation. For FAP-Vimentin and PECAM1/CD31-Vimentin, linearity was lacking, requiring Spearman’s rank correlation as a non-parametric test. The data were visualized using a heatmap to display gene expression levels. A divergent color scale was used, with blue indicating high gene expression and yellow indicating low gene expression.
Statistical validation, software and tools
All analyses and visualizations were performed using R and Python, leveraging key libraries such as pandas for data manipulation, seaborn and matplotlib for visualizations, and scipy for statistical analyses.
Immunohistochemistry
To detect the expression of FAP, Vimentin, and PECAM1/CD31 in the different tissue components of JAs, formalin-fixed, paraffin-embedded samples available from 18 patients and two recurrent samples were utilized for immunohistochemistry. From each sample, 3-micron slides were deparaffinized, and heat-induced antigen retrieval was done in citrate buffer (pH 6.0). Incubation with the specific primary antibodies FAP (1:500, ab53066, Abcam), CD31 (1:40, Dako Agilent), and Vimentin (1:1000, M0725, Dako Agilent) was performed overnight at 4 °C. For negative controls, antibody dilution buffers without primary antibodies were applied. The DAKO Fast Red Kit and DAB Kits (K5005 and K5007, Dako Agilent) were used for detection according to the manufacturer’s instructions. Afterward, the slides were counterstained with Mayer’s Hematoxylin (MHS32, Merck). Two independent observers estimated the percentage and distribution of positive cells in JA stromal and endothelial cells. The overall immunoreactivity was scored using a four-tier scale system based on the rate of positive cells: 0, negative; 1, immunoreactivity in less than 25%; 2, moderate immunoreactivity in less than 75%; and 3, immunoreactivity in 75% or more of the cells.
68Ga-FAPI-04 PET/CT
^68^Ga-FAPI-04 was labeled as described previously [15]. After injecting 146 MBq of ^68^Ga-FAPI-04 (adapted to the patient’s body weight), PET/CT images were acquired 15 min post-injection with a Biograph 40 mCT PET/CT scanner (Siemens Medical Solutions). The slice thickness was 3 mm, and PET acquisition was performed from the skullcap up to and including the liver at 3 min/bed position. The extended field of view was 21.4 cm (TrueV). PET reconstruction was performed with a three-dimensional OSEM algorithm with three iterations, 24 subsets, Gaussian filtering, and a slice thickness of 5 mm. Decay, scatter, attenuation, and random correction were applied. For anatomical localization and attenuation correction, a low-dose CT scan was performed with an X-ray tube voltage of 120 keV and modulation of the tube current with CARE Dose4D with a reference tube current of 35 mAs. The CT scans were performed with a 512 × 512 matrix, reconstructed with an increment of 3 mm and a slice thickness of 5 mm.
Results
Gene expression analysis
RT-PCR analyses of 11 samples from 10 juvenile angiofibroma (JA) patients showed the distinct fibrovascular nature of JA. In all tumors, a heterogeneous expression of PECAM1/CD31 as a marker for vascular components and Vimentin, reflecting the mesenchymal and stromal characteristics of the tumor, was observed. Interestingly, all investigated tumors revealed a pronounced expression of FAP.
Data visualization
FAP expression was consistently observed in all samples. The heatmap (Fig. 1) displays the samples related to the PECAM1/CD31 expression from high to low. By correlation analysis, a tendency (r = 0.52; p = 0,08) for a positive relationship between FAP expression and PECAM1/CD31-positive vascular tumor areas was identified. No significant correlation was seen for patient age or grading.Fig. 1. Heatmap visualizing Delta-Ct values for the genes FAP, PECAM1(CD31), and Vimentin (VIM) in juvenile angiofibroma (JA) samples. The color scale ranges from blue (high gene expression) to yellow (low gene expression)
The varying expression levels, also between samples of the same patient (Sample 6), reflect the heterogeneity of JA.
Immunohistochemistry
Next, immunohistochemical studies validated the relationships indicated by PCR analyses and correlated expression patterns with tumor morphology. A double-staining approach for FAP and CD31 confirmed FAP expression in all JA samples showing FAP-positive stromal cells near CD31-positive vascular regions (Fig. 2) and FAP expression in endothelial CD31-positive cells. As our PCR findings suggested, the varied vascular and stromal components underscore spatial and functional differences within the tumor microenvironment.Fig. 2. Representative images of FAP (red signal) and CD31 (brown signal) immunohistochemistry of juvenile angiofibroma samples. (a) Sample 11, (b) Sample 12, and (c) Sample 2
Comparison of tumoral FAP-expression after immunohistochemical staining and 68Ga-FAPI-04 uptake
Based on the findings from RT-PCR and immunohistochemistry proving FAP expression in juvenile angiofibroma, we pursued the application of ^68^Ga-FAPI-04 PET/CT in a recent suspected case of JA to validate these insights in vivo preoperatively. The FAPI-PET/CT revealed significant uptake in the tumor region. Upon closer analysis of the imaging data, a particularly strong, circular uptake pattern was observed along the entire circumference of the tumor periphery (SUVmax 8.9, SUVpeak 7.1). In contrast, the tumor center exhibited comparatively lower uptake (SUVmax 4.7, SUVpeak 4.5 (Fig. 3)).Fig. 3. Maximum intensity projection (middle) of ^68^Ga-FAPI-04 PET/CT of an 18-year-old man with histopathologically proven juvenile angiofibroma. Additional coronal (left) and axial (right) reconstructions
Postoperative correlation of FAPI-PET-uptake distribution with immunohistochemistry
The tumor was resected in toto and subsequently processed for immunohistochemical analyses. Interestingly, the uptake characteristics from the FAPI-PET were corroborated postoperatively through immunohistochemical staining of the corresponding specimen (Fig. 4), further underscoring the consistency between preoperative imaging and histological findings.Fig. 4FAPI-PET/CT imaging and corresponding histological projection in juvenile angiofibroma (JA). (a) Axial fusion image of FAPI-PET and CT showing the tumor. (b) Magnified FAPI-PET view highlighting peripheral tracer uptake and central hypo-uptake in JA. (c) Projection of the histological section (Hematoxylin and eosin (HE) staining) from the resected tumor, demonstrating spatial correlation with the imaging findings
Immunohistochemical staining showed pronounced FAP expression in the excised tumor periphery, aligning with tracer-rich areas noted in the FAPI-PET. In contrast, the tumor center had a lower FAP density (Fig. 5).Fig. 5. Correlation of histology, FAPI-PET imaging, and immunohistochemistry in juvenile angiofibroma. a) HE staining of an axial tumor section (Scale Bar 5.5 mm) matches the FAPI-PET/CT axial slice (a). Both images show the tumor periphery (black box) and vascularized center (yellow box) with marked regions. C, d (Scale Bar 100 µm) Immunohistochemical double staining for FAP (red signal) and CD31 (brown signal) from the center (c) and periphery (d) of the tumor, referenced in A and B. Differential FAP expression is clear, with stronger staining in the periphery (d) than in the center (c)
Discussion
Due to its distinctive pathophysiological features, JA represents a diagnostic and therapeutic challenge. Current research seeks to understand JA’s pathophysiology to develop new diagnostics and better treatments. As useful targets are lacking, surgical excision remains the gold standard. While the expression of FAP has been well-documented in numerous malignant epithelial tumors [16–23], FAP was not detected in benign epithelial tumors so far [24]. This study is the first to demonstrate FAP expression in JAs. We successfully employed FAPI-PET/CT imaging, providing a direct translational “bench-to-bedside” approach. Our findings offer new biological insights and a promising foundation for innovative diagnostic and therapeutic strategies regarding JAs. Our RT-PCR and immunohistochemical studies confirmed FAP’s role in JA. While there were quantitative differences in FAP expression across samples, PCR showed FAP present in all investigated JAs. Most samples showed moderate FAP expression alongside vimentin and PECAM1/CD31. Individual cases exhibited variations, like higher vimentin with lower FAP and PECAM1/CD31, highlighting tumor morphological heterogeneity and regional adaptability. Additionally, comparisons of samples from the same patient revealed intratumoral heterogeneity based on the expression profile.
Immunohistochemical analyses confirmed heterogeneous FAP distribution, showing varying levels of expression based on stromal and endothelial components. This highlights the potential of targeting FAP in the diagnosis and treatment of JA. FAPI-PET revealed spatial allocation, with higher expression at the tumor periphery and less in the center. Immunohistochemical reactivity against CD31 indicates that FAP is primarily expressed near irregular vascular spaces, the proposed area of tumor origin.
Role of FAP in EMT and angiogenesis
FAP expression in JA may be explained by the epithelial-mesenchymal transition (EMT), a process that influences tumorigenesis and progression. Previous studies have described EMT as contributing to tumor development [1, 3, 6, 7].
Hereby, EMT is a critical process in tumor biology that facilitates the transition of epithelial into mesenchymal cells. Notably, the perivascular FAP expression in stromal cells correlates with the presence of EMT markers [25]. FAP expression has been observed, furthermore, not only in cells of mesenchymal origin [26–28] but also in transformed neuroectodermal cells [29]. They also contribute to tumor progression, invasion, and metastasis by modifying the extracellular matrix and further releasing pro-angiogenic signals [30–32].
Although the exact role of FAP in JA remains unclear, our findings offer insights into FAP’s potential role in tumor development in JA, indicating it may aid tumor progression via EMT and promote angiogenesis. FAP is primarily expressed in the peripheral tumor tissue of JA, corroborated by studies showing its presence in human endothelial cells, where it influences microvascular reorganization and capillary morphogenesis through enzymatic activity [33–37]. Busek et al. found that FAP is expressed by transformed glioblastoma cells and stromal cells with mesenchymal markers near dysplastic blood vessels. This aligns with perivascular FAP staining in JAs. These mesenchymal cells release pro-angiogenic factors, supporting tumor growth [25]. The angiogenic effects may also arise from its co-expression with MMP-9 as a “pro-angiogenic signaler” [38]. Moreover, an indirect influence of FAP on endothelial cell migration and neovascularization through extracellular matrix reorganization has been described [39]. These findings suggest that FAP may contribute to tumor progression and angiogenesis in JAs. However, its exact pro-angiogenic effects should be explored in further studies. In addition to EMT, stromal activation processes and specific differentiation pathways may also contribute to the expression of FAP in JA. In epithelial tumors, FAP is typically expressed by cancer-associated fibroblasts (CAFs), a heterogeneous population of stromal cells characterized by markers such as FAP, α-smooth muscle actin (SMA), and vimentin. These cells actively participate in extracellular matrix remodeling, immunomodulation, and angiogenesis [40–44]. Activated fibroblasts, called myofibroblasts, also play an important role in wound healing and fibrosis. A hallmark of functional myofibroblasts in this context is the expression of α-SMA, which is associated with increased contractility, ECM production, and secretion of inflammatory mediators [45, 46].
In JA, immunohistochemical studies have shown α-SMA expression in vascular smooth muscle cells and focally in fibrotic-hyalinized stromal areas, suggesting localized myofibroblastic differentiation [47, 48]. Liang et al. identified α-SMA-positive perivascular cells as pericytes. They proposed that these cells are potential precursor cells of the fibrous tumor component, with transitional forms toward myofibroblasts being discussed [49].
A potential functional link between FAP and myofibroblasts is supported by preclinical studies demonstrating FAP as a marker of activated myofibroblasts during wound healing and tissue remodeling [50]. In a myocardial infarction model, FAPI-PET imaging was able to visualize the spatial activation of myofibroblasts, an observation that may represent an interesting parallel to our study. Further phenotypic and functional characterization of stromal cell populations in JA, particularly with regard to potential CAF-like features, therefore appears warranted.
Clinical validation through FAPI-PET/CT, diagnostic and therapeutic implications
A significant innovation of our study is the clinical validation of the observed FAP expression in JA tissue samples using FAPI PET/CT imaging. An excellent correlation between uptake in ^68^Ga-FAPI-04 PET/CT and the tumoral FAP expression after immunohistochemical FAP-staining with a higher expression in the periphery and a lower amount in the tumor center was shown. This heterogeneous FAP distribution suggests the beginning of EMT in the tumor periphery, associated with possible ECM remodeling.
Usually performed magnetic resonance imaging (MRI) and additional computed tomography (CT) scans reveal, in general, a highly vascularized lesion with a unique growth pattern, including the expansion of the sphenopalatine foramen, extension into the pterygopalatine fossa with anterior bulging of the posterior maxillary sinus wall, as well as extension through other foramina and fissures. Bony destruction may also be observed at the pterygoid plate and along the sphenoid sinus floor. However, expanded pathologies or atypically located JA and uncertainties from limited experience with this rare tumor can complicate radiological differentiation. Radiological assessment is often insufficient in clinical practice, and a biopsy of this highly vascularized tumor has a high risk of severe bleeding. Preferably, an angiography is performed to determine the tumor’s blood supply and identify the typical vascularization pattern before tumor excision. Combined with MRI and CT, this method allows for the diagnosis of JA and gives the potential for simultaneous embolization during angiography.
Our data from retrospective expression and immunohistochemical analyses and its validation through FAPI-PET/CT in a current case suggest that this imaging modality is a sensitive tool for differential diagnosis. FAPI-PET/CT in preoperative diagnostic work could reduce the need for invasive diagnostic procedures, such as angiography, in case of no intended surgery and premature biopsies. This new diagnostic facility offers the chance for follow-up of residual tumors. Hereby, non-intensive uptake in residual JA by FAPI-PET/CT suggests no remarkable growth pattern, enabling a further wait and scan policy.
Surgery can be challenging in highly vascularized tumors. Reducing the amount of vascularity and shrinking the JA size before the tumor is surgically removed is already of great interest. Therapeutic approaches that possess the potential to eradicate tumors completely, thereby making surgical interventions unnecessary, are particularly thrilling. In this context, innovative pharmacological treatment options are of great interest for treating JAs. In other tumor diseases, numerous FAP inhibitors have been investigated, and also theranostic approaches have been explored in nuclear medicine. FAP tracers can be used for targeted radionuclide therapies, specifically destroying tumor cells while sparing healthy tissue. FAP molecules coupled with therapeutic emitters such as Yttrium-90 enable diagnostic and therapeutic applications [12]. First clinical applications with ^90^Y-, ^177^Lu-, ^225^Ac-, and ^153^Sm-FAP tracers showed promising results [12, 14, 51]. FAP-binding peptides, such as FAP-2286, coupled to a radionuclide chelator, have been proposed for imaging using ^68^Ga-FAP-2286 and for therapeutic application using ^177^Lu-FAP-2286 in a wide range of FAP-positive tumors [51, 52].
Moreover, CAR-T cell therapies targeting FAP-expressing cells have also shown promising results in preclinical studies and are becoming an effective treatment method [53–55]. In addition, FAP-targeted monoclonal antibodies are under investigation [56, 57]. Furthermore, small-molecule inhibitors [58], combined with cytostatics [59] or chemotherapeutics [60], showed promising results in Phase II trials.
The identification of FAP in JA opens new diagnostic and treatment possibilities. These could enhance outcomes and lower risks associated with conventional treatments in complex cases.
Limitations
Although our study is promising and provides novel insights, several limitations must be considered. The heterogeneity of JA may result in pronounced interindividual variability in FAP expression, influenced by clinical factors such as patient age, tumor size, and stage, as well as by fibrotic remodeling processes and EMT activity. This heterogeneity may impact the sensitivity and specificity of FAPI-PET/CT imaging, as well as the efficacy of FAP-targeted therapies. Functional studies investigating the role of FAP in tumor progression and signaling pathway interactions are therefore needed to deepen our understanding of FAPI-PET/CT diagnostics across different patient subgroups and to refine potential therapeutic targets.
Furthermore, increased FAP expression has also been reported in benign conditions [40, 45], which may limit the specificity of FAPI-PET/CT for JA. Comparative analyses with other benign lesions of the nasopharyngeal region are thus required to validate the specificity of this imaging modality. Additionally, although JA is a benign tumor, its locally aggressive growth pattern and imaging characteristics can overlap with those of malignant head and neck tumors, such as nasopharyngeal carcinoma [61–63], and may even be difficult to distinguish from mesenchymal malignancies such as sarcomas [64]. In this context, a recent study demonstrated high FAP expression in various sarcomas [64], underscoring the need for cautious interpretation of FAPI-PET/CT results and thorough differential diagnosis. Therefore, FAPI-PET/CT findings in JA should always be interpreted within the clinical context, particularly given the tumor’s highly characteristic features—such as patient age, sex, and anatomical location—that support a high pretest probability. Similar to conventional angiography, where nonspecific hypervascularization gains diagnostic value only through clinical correlation, FAPI-PET/CT should be assessed in conjunction with clinical and endoscopic findings to ensure appropriate diagnostic specificity.
Conclusion
To our knowledge, this is the first study demonstrating FAP expression in JA. We demonstrated its diagnostic significance through an integrative, sequential “from-bench-to-bedside” approach by successfully using FAPI-PET/CT as a new diagnostic modality in these tumors. However, further investigations are necessary to exploit clinical experience and the potential of FAP-targeted approaches in clinical practice to optimize diagnosis and therapy in JA.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1