A novel case of cutaneous plasmacytosis in a patient of Native American ancestry
Giovanna A. Miller, Tyler Enos, Scott D. Miller

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
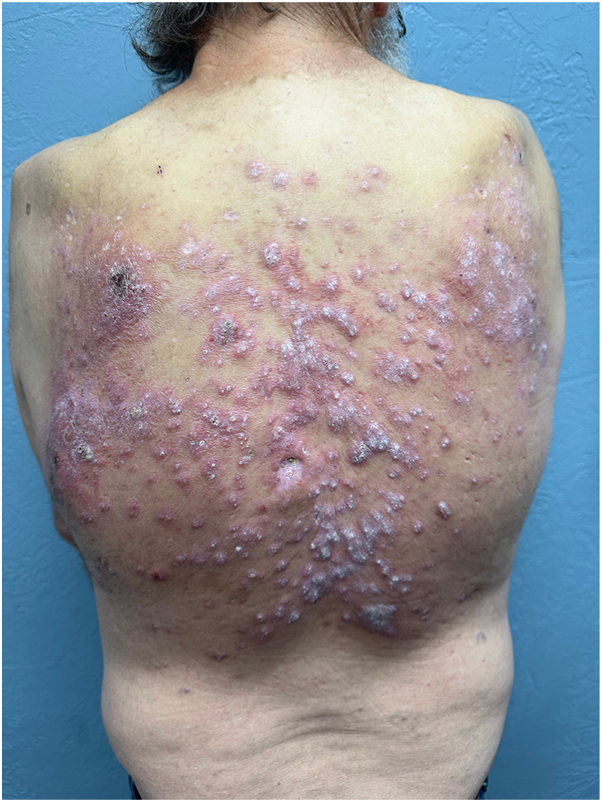 Figure 1
Figure 1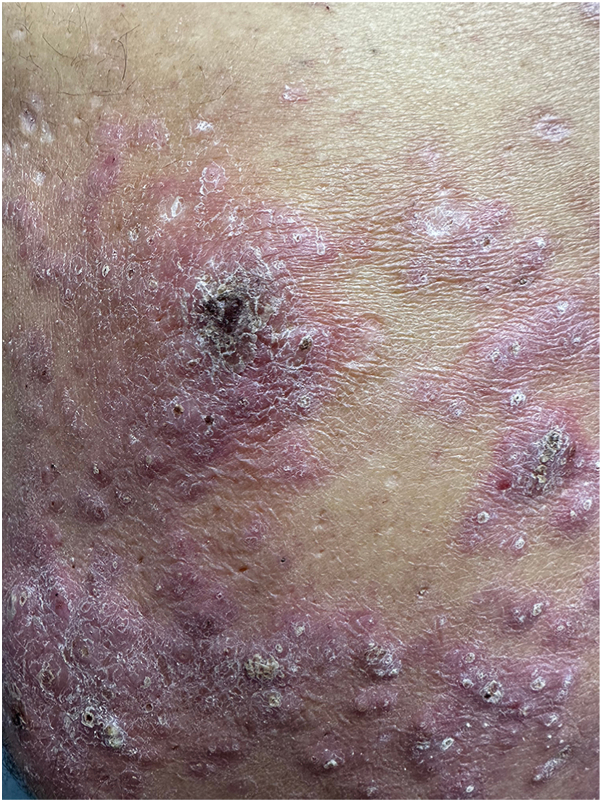 Figure 2
Figure 2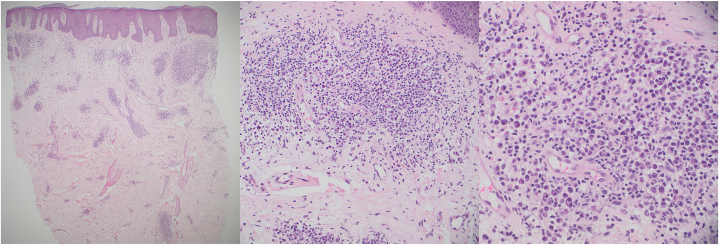 Figure 3
Figure 3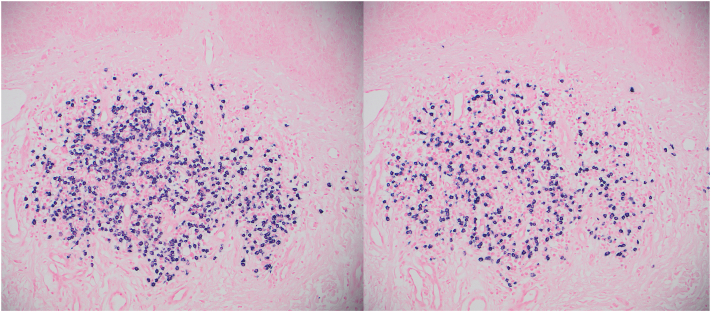 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Cutaneous lymphoproliferative disorders research · Myeloproliferative Neoplasms: Diagnosis and Treatment
Introduction
Cutaneous plasmacytosis is a rare condition of unknown etiology that occurs predominantly in patients of Southeast Asian descent and is characterized by the benign proliferation of polyclonal plasma cells. It typically presents as reddish-brown papules and plaques, most commonly affecting the trunk and face.1 In the literature, we found only 11 reported cases in individuals of non-Southeast Asian descent. Here, we report another rare exception: a 59-year-old male with Native American ancestry.
Case report
A 59-year-old male of mixed Occidental and Native American descent presented with a 20-year history of generally asymptomatic, reddish to violaceous hypertrophic papules and plaques on his back (Figs 1 and 2). He was otherwise in good health, without fever, chills, malaise, or weight loss. No evidence of polyneuropathy or organomegaly was found, and he had no history of travel outside the continental United States. Over the years, numerous providers had treated his rash with various therapies, including topical glucocorticosteroids of different strengths, oral antibiotics such as doxycycline, antimalarial drugs such as hydroxychloroquine, dupilumab, and oral isotretinoin. According to the patient, none of these treatments provided any benefit. Skin examination revealed nontender, reddish to violaceous hypertrophic papules and plaques covering most of the back, without associated palpable lymphadenopathy. A punch biopsy was performed to further characterize the eruption, showing a superficial and deep perivascular infiltrate composed of lymphocytes and numerous mature plasma cells without atypia (Fig 3). These cells were positive for cluster of differentiation 138. Kappa and lambda in situ hybridization revealed a ratio of approximately 2:1 (Fig 4). The immunoglobulin G4 to immunoglobulin G ratio was less than 20%. A spirochete immunohistochemical stain for organisms was negative.Fig 1. Cutaneous plasmacytosis presenting as reddish papules and plaques on the patient’s back.Fig 2. Close-up view of cutaneous plasmacytosis.Fig 3. Hematoxylin and eosin–stained section showing a superficial and deep perivascular infiltrate composed of lymphocytes, histiocytes, and numerous mature plasma cells. The left portion of the image is shown at 40× magnification, with 200× in the center and 400× on the right.Fig 4. Kappa (shown on the left at 100× magnification) and lambda (shown on the right) in situ hybridization studies reveal a ratio of approximately 2:1.
Laboratory workup included a complete blood count, protein electrophoresis, urinalysis, rapid plasma reagin, and HIV antibody testing, all of which were largely unremarkable, except for a mild elevation of gamma globulin at 2.1 (reference range: 0.4-1.8).
Discussion
We describe a patient with Native American ancestry who presented with a rare condition, cutaneous plasmacytosis, typically reported almost exclusively in individuals of Southeast Asian descent. The condition was first described in 1976 by Yashiro1 and later further characterized by Kitamura et al2 in 1980 as reddish-brown papules and plaques, usually favoring the trunk and face, composed of polyclonal plasma cells, and generally following a benign, chronic course. We note that our patient’s lesions were noticeably less brown and more hypertrophic than is typically described in the literature, which may in part be explained by his phenotype being atypical for this disease. Cutaneous plasmacytosis has been reported with a male-to-female ratio of 1:0.6, at a mean and median age of 37 years (range: 20-62 years).3
Plasmacytosis should be differentiated from a multitude of other plasma cell disorders. Syphilis can be excluded by negative treponemal immunohistochemistry and rapid plasma reagin tests. A plasma cell variant of multicentric Castleman’s disease is characterized by sheets of plasma cells within lymph nodes, often associated with systemic symptoms like fever and organ dysfunction secondary to hypercytokinemia. Multicentric Castleman’s disease’s constellation of findings were absent in our patient’s presentation. POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes) and AESOP (adenopathy and extensive skin patch overlying a plasmacytoma) syndromes can be ruled out by the absence of their characteristic findings, including polyneuropathy, organomegaly, endocrinopathy, bone involvement, and life-threatening progression. Similarly, the distribution pattern excludes other benign mucocutaneous plasma cell disorders, such as plasma cell gingivitis, plasma cell cheilitis, Zoon’s balanitis, and Zoon’s vulvitis. The etiology of cutaneous plasmacytosis remains undefined. Some speculate that upstream signaling molecules may influence interleukin-6 activity, which drives B-cell differentiation into plasma cells, in a manner similar to cytokine effects observed in Castleman disease.4
Treatment outcomes tend to be disappointing, as observed in our patient. Reported therapies are extensive and include systemic, intralesional, and topical corticosteroids; topical tacrolimus; antibiotics; systemic chemotherapies such as melphalan; anti-CD20 antibody therapy; prednisone–cyclophosphamide combination therapy; radiotherapy; psoralen and UV-A light; and thalidomide.5, 6, 7, 8, 9
Plasmacytosis is an extremely rare disease with little known about its causes or effective treatments. Identification of additional cases may help further characterize this unusual process. We present this unique occurrence in the hope that its contribution to the epidemiological literature may aid in the future delineation and definition of this elusive disease.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yashiro A.A kind of plasmacytosis: primary cutaneous plasmacytoma[In Japanese]Jpn J Dermatol 861976910
- 2Kitamura K.Tamura N.Hatano H.Toyama K.Mikata A.Watanabe S.A case of plasmacytosis with multiple peculiar eruption J Dermatol 71980341349700968410.1111/j.1346-8138.1980.tb 01981.x · doi ↗ · pubmed ↗
- 3Uhara H.Saida T.Ikegawa S.Primary cutaneous plasmacytosis: report of three cases and review of the literature Dermatology 1891994251255794947710.1159/000246848 · doi ↗ · pubmed ↗
- 4Kodama A.Tani M.Hori K.Systemic and cutaneous plasmacytosis with multiple skin lesions and polyclonal hypergammaglobulinemia: significant serum interleukin-6 levels Br J Dermatol 12719924953163769510.1111/j.1365-2133.1992.tb 14827.x · doi ↗ · pubmed ↗
- 5Miura H.Itami S.Yoshikawa K.Treatment of facial lesion of cutaneous plasmacytosis with tacrolimus ointment J Am Acad Dermatol 39200319519610.1016/s 0190-9622(03)00860-014639422 · doi ↗ · pubmed ↗
- 6Carey W.P.Rico M.J.Nierodzik M.Sidhu G.Systemic plasmacytosis with cutaneous manifestations in a white man: successful therapy with cyclophosphamide/prednisone J Am Acad Dermatol 381998629631955580710.1016/s 0190-9622(98)70131-8 · doi ↗ · pubmed ↗
- 7Yamamoto T.Soejima K.Katayama I.Nishioka K.Intralesional steroid-therapy-induced reduction of plasma interleukin-6 and improvement of cutaneous plasmacytosis Dermatology 1901995242244759939010.1159/000246698 · doi ↗ · pubmed ↗
- 8Kaneda M.Kuroda K.Fujita M.Shinkai H.Successful treatment with topical PUVA of nodular cutaneous plasmacytosis associated with alopecia of the scalp Clin Exp Dermatol 2119963603649136157 · pubmed ↗