Haemorrhagic Safety Update of CLEAR-PATH: 30 Day and 12 Month Antiplatelet Therapy After Peripheral Angioplasty
Emilien C.J. Wegerif, Manon I. Generaal, Linde J. Vijn, Rutger M. van den Bor, Peter M. van de Ven, Michiel L. Bots, Gert J. de Borst, Çağdaş Ünlü

TL;DR
This study found that antiplatelet therapy after peripheral angioplasty has low bleeding risks, mostly within the first 30 days and linked to vascular procedures.
Contribution
The study provides novel haemorrhagic safety data for antiplatelet therapy after endovascular revascularisation in peripheral arterial disease patients.
Findings
Major bleeding incidence was between 1% and 2.9% within 12 months after EVR.
Most major bleeds occurred within 30 days and were related to vascular procedures.
Combining clopidogrel and acetylsalicylic acid did not increase bleeding risks.
Abstract
Antiplatelet therapy (APT) bleeding risks after endovascular revascularisation (EVR) in peripheral arterial disease (PAD) patients are lacking. Therefore, this Dutch, multicentre, double blind, placebo controlled randomised trial aimed to determine the haemorrhagic safety of APT within 30 days and 12 months after EVR by using data from the ongoing CLEAR-PATH trial. Symptomatic PAD patients after successful EVR were randomised to clopidogrel plus placebo or acetylsalicylic acid for 12 months. The primary endpoint was major bleeding (MB) following the TIMI (Thrombolysis in Myocardial Infarction) classification within 12 months. Secondary endpoints included MB within 12 months following ISTH (International Society on Thrombosis and Haemostasis) and BARC (Bleeding Academic Research Consortium) classification, within 30 days following all classifications, and any bleeding. Analyses were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
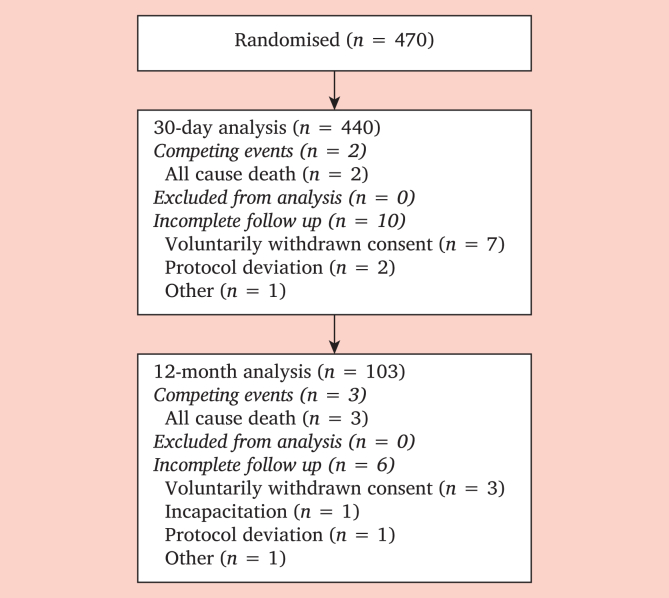 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntiplatelet Therapy and Cardiovascular Diseases · Coronary Interventions and Diagnostics · Peripheral Artery Disease Management
INTRODUCTION
When prescribing antiplatelet therapy (APT) for patients with peripheral arterial disease (PAD) after endovascular revascularisation (EVR), guidelines recommend considering the atherothrombotic risk associated with PAD, the vascular procedure, as well as the bleeding risk of the patient and the APTs.1^,^2, 3, 4, 5, 6 The latter has gained more awareness since the consequences of bleeding have become clearer due to research in the field of coronary artery disease (CAD); researchers have found a strong relationship between the severity of bleeding and risk of death.7 More specifically, major bleeding complications are associated with a mortality rate similar to myocardial infarction, with the increased risk of death primarily occurring within 30 days after the bleeding.7^,^8 Concerning PAD, insufficient literature is focusing on bleeding events, leading to a large knowledge gap; there is no validated bleeding classification system, studies have heterogeneous designs, the PAD patient mortality rate from a (major) bleeding event is unknown, common origins of bleeding events are unknown, and the APT bleeding incidence is underreported.1^,^9
The CLEAR-PATH trial was initiated to compare the efficacy and safety of clopidogrel monotherapy with clopidogrel plus acetylsalicylic acid (ASA) within 12 months after EVR.10 Due to the limited literature on bleeding events associated with APT following EVR, the safety assessment of the CLEAR-PATH protocol states only: “there is no evidence that dual APT led to a higher risk of major bleeding than mono APT”, based on even fewer and more heterogeneous literature.11, 12, 13, 14 Due to this uncertainty, additional data regarding safety of APT is warranted. For this reason, this paper presents the composition of the current CLEAR-PATH cohort, major bleeding events within 30 days and 12 months of APT use after EVR, and the location of major bleeding and its consequences, based on blinded data in the first year of enrolment.
METHODS
Trial safety objectives and endpoints
The primary safety objective was to compare rates of major bleeding between clopidogrel monotherapy and clopidogrel plus ASA follosing the Thrombolysis (Table 1).10^,^15 The TIMI classification was chosen as the primary safety outcome since this is the most used bleeding classification within the field of PAD, which makes data feasible for future comparisons.16 The secondary safety objectives focused on the difference in major bleeding between clopidogrel plus ASA and clopidogrel monotherapy within 30 days and 12 months following other bleeding classifications: TIMI classification (30 day analysis only), The International Society on Thrombosis and Haemostasis (ISTH) and the Bleeding Academic Research Consortium (BARC) classification.17^,^18 For the BARC classification, class 3b or higher was considered as major. Another objective was any bleeding following the TIMI classification within 30 days and 12 months. In addition to bleeding classifications, the location and or cause of the bleeding was recorded and noted. Only blinded results were available for these analyses; therefore, no difference between clopidogrel and clopidogrel plus ASA was shown. However, the last objective was to assess whether the difference in 12 month major bleeding incidence between treatment groups remains within the pre-defined acceptable margin of 3.0%, assuming that no treatment group has a 0.0% risk.Table 1. Definitions of major and minor bleeding following the bleeding classification used in this trial. This table provides an overview of the three bleeding classifications used in this safety analysis.TIMI classificationMajor bleeding
-
1.Intracranial haemorrhage or a 5 g/dL (i.e., 3.10 mmol/L) decrease in the haemoglobin concentration, or
-
2.a 15% absolute decrease in the haematocrit. Minor bleeding
-
1.Observed blood loss: 3 g/dL (i.e., 1.86 mmol/L) decrease in the haemoglobin concentration, or
-
2.10% decrease in the haematocrit. No observed blood loss: 4 g/dL (i.e., 2.48 mmol/L) decrease in the haemoglobin concentration, or
-
3.12% decrease in the haematocrit. Minimal bleeding
-
1.Any clinically overt sign of haemorrhage (including imaging) that is associated with a <3 g/dL (i.e., 1.86 mmol/L) decrease in the haemoglobin concentration, or
-
2.<9% decrease in the haematocrit. ISTH classificationMajor bleeding
-
1.Fatal bleeding or
-
2.Symptomatic bleeding in a critical organ or location (e.g., intracranial, intraspinal, intra-ocular, retroperitoneal, intra-articular/pericardial, intramuscular including compartment syndrome);
-
3.Fall in haemoglobin level of at least 20 g/L (1.24 mmol/L) due to bleeding;
-
4.Bleeding requiring transfusion of two or more units of blood or red cells. Clinically relevant non-major bleeding
-
1.Any sign or symptoms of haemorrhage (e.g., more bleeding than would be expected) that does not meet the criteria of major bleeding following the ISTH criteria but does meet at least one of the following criteria:
-
a.Require medical interventions by a healthcare professional
-
b.Leading to hospitalisation or increased level of care
-
c.Prompting a face to face evaluation BARC classification
-
•Type 0: no bleeding
-
•Type 1: bleeding that is not actionable and does not cause the patient to seek unscheduled performance of studies, hospitalisation, or treatment by a healthcare professional; may include episodes leading to self discontinuation of medical therapy by the patient without consulting a healthcare professional
-
•Type 2: any overt, actionable sign of haemorrhage (e.g., more bleeding than would be expected for a clinical circumstance, including bleeding found by imaging alone) that does not fit the criteria for type 3, 4, or 5 but does meet at least one of the following criteria: (1) requiring non-surgical medical intervention by a healthcare professional, (2) leading to hospitalisation or increased level of care, or (3) prompting evaluation
-
•Type 3
-
○Type 3a
-
▪Overt bleeding plus haemoglobin drop of 3 to <5 g/dL∗ (i.e., 3.10 mmol/L) (provided haemoglobin drop is related to bleed)
-
▪Any transfusion with overt bleeding
-
○Type 3b
-
▪Overt bleeding plus haemoglobin drop ≥5 g/dL∗ (i.e., 3.10 mmol/L) (provided haemoglobin drop is related to bleed)
-
▪Cardiac tamponade
-
▪Bleeding requiring surgical intervention for control (excluding dental, nasal, skin, or haemorrhoid)
-
▪Bleeding requiring intravenous vasoactive agents
-
○Type 3c
-
▪Intracranial haemorrhage (does not include microbleeds or haemorrhagic transformation, does include intraspinal)
-
▪Subcategories confirmed by autopsy or imaging or lumbar puncture
-
▪Intraocular bleed compromising vision
-
•Type 4: CABG related bleeding
-
○Peri-operative intracranial bleeding within 48 hours
-
○Re-operation after closure of sternotomy for the purpose of controlling bleeding
-
○Transfusion of ≥5 U whole blood or packed red blood cells within a 48 hour period^†^
-
○Chest tube output ≥2 L within a 24 hour period
-
• Type 5: fatal bleeding
-
○Type 5a: Probable fatal bleeding; no autopsy or imaging confirmation but clinically suspicious
-
○Type 5b: Definite fatal bleeding; overt bleeding or autopsy or imaging confirmation TIMI = Thrombolysis In Myocardial Infarction; ISTH = The International Society on Thrombosis and Haemostasis; BARC = Bleeding Academic Research Consortium.
Data monitoring
Since PAD patients are at high risk of serious adverse events,2 only trial related adverse events were registered (among which were atherothrombotic events, bleeding events, death, and peptic ulcers).10 The Clinical Trial Centre Maastricht, an independent clinical research organisation, monitored all activities as (source) data verification and verification of potentially missed trial related adverse events in samples of patients' records. For significantly missing information, all patients’ records were screened. Secondly, an adjudication committee, consisting of an independent neurologist, cardiologist, and vascular surgeon, audited all reported events.
Data analysis
The baseline characteristics and (primary and secondary) safety endpoints of all included patients in the first 1.5 year enrolment period of the ongoing CLEAR-PATH trial were summarised by mean with standard deviation (SD). Categorical variables were summarised by counts and percentages. For primary and secondary endpoint(s), counts and percentages were presented for subjects with a randomisation date (a) 12 months and (b) 30 days before the reference date (1 Feb 2024). It was assumed that the risk of major bleeding within 12 months of follow up was higher than 0.0% in both groups (clopidogrel and clopidogrel plus acetylsalicylic acid) and agreed that a difference of up to 3.0% between the two treatment groups was acceptable. Analyses were performed using R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).19 Wilson score interval was used to derive confidence intervals.20
Design
The rationale and design of the CLEAR-PATH trial were reported recently.10 In brief, the CLEAR-PATH (EudraCT number: 2021-006611-29) is an investigator initiated, randomised, placebo controlled, double blind, multicentre trial in the Netherlands that primarily compares the efficacy and safety of clopidogrel plus ASA with clopidogrel monotherapy after EVR.
Symptomatic PAD patients with planned EVR with or without thrombo-endarterectomy were included (Table 2). The main exclusion criteria were acute limb ischaemia, re-intervention within two months, or an increased risk of bleeding (i.e., coagulopathy, dialysis, liver failure). After successful EVR, patients were randomised in a 1:1 fashion to clopidogrel 75 mg plus placebo daily or clopidogrel 75 mg plus ASA 80 mg daily for up to 12 months. At each follow up (i.e., four to six weeks post-EVR, every six months, and local visits), patients were assessed for trial related endpoints such as major adverse cardiovascular events, major adverse limb events, and bleeding events.Table 2. Inclusion and exclusion criteria for CLEAR-PATH.10 This table outlines the pre-defined eligibility criteria used for screening and enrolment. The inclusion criteria reflect the target population of the CLEAR-PATH trial, while the exclusion criteria are focused on ensuring accurate selection and patient safety.Inclusion criteria
- **1.**Lesions of the iliac, femoropopliteal, and or below the knee arteries
- **2.**At least one TASC lesion
- **3.**Rutherford (1–6) classes with an indication for an endovascular revascularisation
- **4.**Proficient understanding of the consequences of enrolment by the patient
- **5.**Written informed consent by the patient
- **6.**Age ≥45 years And:
- **7.**Eligibility of lesions for;
- a.PTA or recanalisation with or without additional stenting based on prevailing guidelines, or
- **b.**Hybrid procedure with an endarterectomy of the common femoral artery and additional iliac, femoral, or tibial PTA, or
- **c.**A re-intervention within 2 months due to a phased treatment. Exclusion criteria
- **1.**Acute (limb) ischaemia
- **2.**Reported intolerance or hypersensitivity to the study medications
- **3.**Use of anticoagulant therapy (DOACs or coumarin)
- **4.**Use of NSAIDs >2 weeks which cannot be discontinued
- **5.**Patients unable to understand the consequences of enrolment in the trial
- **6.**Patients with a re-intervention due to re-stenosis or re-occlusion within 2 months
- **7.**Patients with a hybrid procedure other than endarterectomy of the common femoral artery such as femoral bypass
- **8.**Patients with coagulopathy
- **9.**Patients with a peptic ulcer confirmed by an oesophagogastroduodenoscopy in their medical history
- **10.**Patients who are pregnant, contemplating pregnancy, or nursing.
- **11.**Patients requiring dialysis
- **12.**Patients with liver failure and at least one of the following criteria;
- **a.**elevated INR value, or
- **b.**portal hypertension, or
- **c.**thrombocytopenia <50x10^9^/L, or
- **d.**INR, portal tension, or platelet count is unknown TASC = TransAtlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease; PTA = percutaneous transluminal angioplasty; DOAC = direct acting oral anticoagulant; NSAID = non-steroidal anti-inflammatory drug; INR = International Normalised Ratio.
This trial was based on the intention to treat principle. Based on an estimated primary efficacy endpoint risk of 30% within one year in the clopidogrel monotherapy arm, an absolute risk reduction of 7% in the clopidogrel plus ASA arm, and 90% power, 450 primary efficacy events (1 696 patients) were required.10 These estimates were based on the limited literature regarding post-EVR PAD patients.21, 22, 23, 24 The end of study will be reached when either 450 primary endpoint events have been observed or all patients have had a primary endpoint event or have completed the 12 month follow up, whichever comes first. After grant approval in August 2021, preparation started in December 2021 (i.e., legal contracts, medication production, local approval in 14 hospitals, etc).25 The NedMec medical ethics review committee approved the CLEAR-PATH trial on 27 May 2022. The first enrolment was on 24 August 2022.
RESULTS
Baseline characteristics
From August 2022 to January 2024, 470 patients were randomised across 15 hospitals in the Netherlands. On 31 January 2024, the 12 month follow up results were available for 103 patients, and the 30 day follow up results were available for 440 patients (Fig. 1). Most patients were Caucasian (93%), ex-smokers (55%), and men (66%) with a history of hypertension (72%), hyperlipidaemia (71%), and or intermittent claudication (68%) (Table 3). The mean age was 68 years. Most patients were treated by stent placement (72%) due to stenosis (56%) in the iliac (60%) or femoropopliteal (50%) region.Figure 1. The study flowchart.Table 3. The baseline characteristics of the study population containing 470 participants. The characteristics are subdivided into six main categories.CharacteristicsTotal (n = 470)Demographics Mean age – y68.3 (±8.9) Female sex161 (34.4) Mean body mass index – kg/m^2^26.3 (±4.4)Ethnicity Caucasian408 (92.7) Black6 (1.4) Asian7 (1.6) Multiple, other, or unknown19 (4.3)Hyperlipidaemia331 (71.2)Smoking status Never smoked64 (14.0) Ex-smoker251 (54.8) Current smoker143 (31.2)Diabetes mellitus156 (33.5)eGFR <60 mL/min/1.73m^2^65 (14)Previous coronary artery disease131 (27.9)Previous myocardial infarction62 (13.2)Previous carotid artery disease34 (7.4)Previous stroke35 (7.4)Previous heart failure12 (2.6)Peripheral artery disease related history Previous amputation14 (3.0) Previous PTA (w or w/o stent)180 (38.3) Previous TEA65 (13.8) Previous thrombolysis5 (1.1) Previous leg revascularisation193 (41.1) Classification of clinical symptoms Intermittent claudication311 (67.9) Chronic limb threatening ischaemia147 (32.1)Ankle brachial index (categories) <0.462 (15.9) 0.4–0.69194 (49.6) 0.7–0.994 (24.0) >0.91 and ≤1.340 (10.3) >11 (0.3)Type of stenosis Stenosis only261 (55.5) Occlusion only101 (21.5) Both31 (6.6) Endovascular without TEA393 (83.6) Endovascular with TEA72 (15.3) Iliac region286 (61.0) Femoropopliteal region236 (50.3) Crural region48 (10.2) Multilevel procedure103 (22.2)Stent length No stent133 (28.3) Total sum ≤10 mm172 (36.6) Total sum ≥10 mm165 (35.1)Medication use Statin303 (91.5) Antihypertensive drugs305 (91.6)Data are presented as n (%) or mean ± SD. SD = standard deviation; eGFR = estimated glomerular filtration rate; PTA = percutaneous transluminal angioplasty; TEA = thromboendarterectomy; mm = millimetre.
Safety endpoints
The primary safety endpoint occurred in two of 103 (1.9%, 95% Wilson confidence interval [CI] 0.5–6.8) patients (Table 4). Major bleeding within 12 month follow up following BARC and ISTH was found in one (1.0%) and three (2.9%) of a total of 103 patients, respectively. Competing events were registered for three of 103 (2.9%) patients for each classification and concerned only with all cause death. In total, six of 103 (5.8%) patients prematurely ended follow up without any specific type of bleeding for all three classifications. Reasons for premature end of study were loss of follow up, voluntary withdrawal consent, incapacitation, and protocol deviation. With a maximum rate of 2.9% for major bleeding events within 12 months of follow up, and the assumption that the risk of major bleeding events in both groups was greater than 0.0%, the maximum possible difference between the groups was 2.8%.Table 4. Primary and secondary safety endpoints. A. presents data on the number of events of the primary and secondary endpoints, competing events, and incomplete follow up of the 440 participants in the 30 days of follow up group. B. presents data on the number of events of the primary and secondary endpoints, competing events, and incomplete follow up of the 103 participants in the 12 month follow up group.ABN (%) patients randomised at least 30 days before reference date (n = 440)N (%) patients randomised at least 12 months before reference date (n = 103)Safety endpointsEventsCompeting event or incomplete FUEventsCompeting event or incomplete FUMajor bleeding following TIMI classification4 (0.9)2 (0.5)/10 (2.3)2 (1.9)3 (2.9)/6 (5.8)Major bleeding following BARC classification∗3 (0.7)2 (0.5)/10 (2.3)1 (1.0)3 (2.9)/6 (5.8)Major bleeding following ISTH classification6 (1.4)2 (0.5)/10 (2.3)3 (2.9)3 (2.9)/6 (5.8)Any bleeding following TIMI classification12 (2.7)2 (0.5)/10 (2.3)7 (6.8)3 (2.9)/6 (5.8)TIMI = Thrombolysis In Myocardial Infarction classification; ISTH = The International Society on Thrombosis and Haemostasis classification; BARC = Bleeding Academic Research Consortium classification; FU = follow up.∗3b or higher is considered as major bleeding.
Major bleeding rates within 30 days of follow up following the TIMI, BARC, and ISTH classifications were 0.9% (four of 440), 0.7% (three of 440), and 1.4% (six of 440), respectively (Table 4). The numbers of competing events and incomplete follow ups were low. Any bleeding within 30 days of follow up was found in 12 of 440 (2.7%) patients. Any bleeding within 12 months of follow up following TIMI classification was found in seven of 103 (6.8%) patients. Considering all registered major bleeding events, except for one event (major bleeding due to a gastric ulcer), all major bleeding events happened in the first 30 days and were mostly related to a vascular intervention (Table 5). Two bleeding events were followed by death within 30 days, of which one was a cardiovascular death and one non-cardiovascular death.Table 5. An overview of patients with major bleeding. If a bleeding event was considered major following one of the three bleeding classification, the event is mentioned in the table below. Per major bleeding event, the table shows the timing of the event since the endovascular revascularisation, whether the bleeding event was major or minor following the classification, what the location or cause of the bleeding event was, and the impact of the event.Patient12 mo FU analysesDays after EVRTIMIISTHBARC∗Cause and location of bleedingImpactP1Y6MajorMajor3bHaematuriaHospitalisation; full recoveryP2N25MajorMajor3bPost-procedural bleeding at procedure siteProlonged hospitalisation; recoveringP3N0MajorMajor3bPost-procedural bleeding at procedure siteCardiovascular death, 13 days after eventP4N25MajorMajor3aDiverticular haemorrhageNon-cardiovascular death, 29 days after eventP5Y49MajorMajor3aDuodenal haemorrhage due to ulcerHospitalisation; full recoveryP6Y3MinimalMajor3aHaemoglobin fall of unknown aetiologyTemporary extra care via outpatient clinic; recovery unknownP7N0MinimalMajor2Post-procedural bleeding at procedure siteTemporary extra care including additional intervention; recovery unknownP = patient; mo = months; FU = follow up; EVR = endovascular revascularisation; TIMI = Thrombolysis In Myocardial Infarction classification; ISTH = The International Society on Thrombosis and Haemostasis classification; BARC = Bleeding Academic Research Consortium classification.∗3b or higher is considered as major bleeding.
DISCUSSION
This safety report contains blinded data from the first 470 patients enrolled in the CLEAR-PATH trial. At baseline, two thirds of the patients had intermittent claudication, and one third had chronic limb threatening ischaemia (CLTI). Based on the current data, approximately 1.9% of patients experienced major bleeding within 12 months after EVR. The major bleeding events occurred with one exception within the first 30 days after EVR and were mostly related to vascular procedures. Despite these data, the start of APT after EVR must not be delayed, given that the risk of atherothrombotic events is significantly higher during this period.10 Importantly, with a maximum difference of 2.8% in major bleeding risk within 12 months between dual APT (clopidogrel plus acetylsalicylic acid, DAPT) and mono APT (clopidogrel), the difference is below the pre-specified threshold of 3.0%. These results indicate that APT with either DAPT or single antiplatelet therapy (SAPT) is safe, and therefore, DAPT for up to 12 months does not lead to a clinically relevant increased risk of major bleeding.
The most commonly given antithrombotic therapy for patients with PAD is APT (more specifically, ASA or clopidogrel monotherapy), vitamin K antagonist, and ASA plus low dose rivaroxaban or clopidogrel.1^,^2, 3, 4, 5, 6 A meta-analysis of ATT in PAD patients based on randomised controlled trials (RCTs) showed that for the ATTs described above, an increased risk of major bleeding in patients with vitamin K antagonist and ASA plus low dose rivaroxaban compared with ASA.16 The absolute weighted incidences of major bleeding were 2.5% (range 0.0–4.2%, eight RCTs) for ASA, 1.6% (0.00–1.6%, two RCTs) for clopidogrel, 3.4% (range 0.0–8.3%, six RCTs) for ASA plus clopidogrel, 3.6% (0.0–4.3%, three RCTs) for ASA plus low dose rivaroxaban, and 8.1% (one RCT) for vitamin K antagonist (Supplementary Table S1).16 However, heterogeneous study designs (i.e., follow up duration and pre- or post-intervention) and different (non-validated) bleeding classifications make definitive conclusions impossible.16
Focusing on post-procedural bleeding, the VOYAGER trial found a statistically significantly increased incidence of major bleeding in the subgroup that received ASA plus low dose rivaroxaban (absolute risk of 2.3%) compared with ASA monotherapy (absolute risk of 1.5%) after EVR, following the TIMI classification within 28 months.26 The EUCLID trial compared clopidogrel with ticagrelor in symptomatic PAD patients and reported on post-procedural bleeds. EUCLID found a major bleeding incidence of 7.8% and any bleeding incidence of 15.7% within 30 months after EVR, following the ISTH classification.27 Comparable findings with CLEAR-PATH were the definition of major bleeding: most experienced a haemoglobin decrease of ≥2 g/dL (1.24 mmol/L) without the need for blood transfusion, and both studies showed low fatal bleeding or bleeding in a critical location (0.4% in EUCLID, 0.0% in CLEAR-PATH). In the studies, approximately half of the post-procedural bleeding events were found in the first seven days, which was comparable with the current findings.
Differences in (non-validated) bleeding classifications must be considered when comparing trials, since they lead to different results (Table 4). The ISTH classification is likely to report the highest incidence of major bleeding since the decrease in haemoglobin level is relatively small.15^,^17 The BARC classification does not define major bleeding; however, when 3b is considered as major, as in CLEAR-PATH and VOYAGER, the decrease in haemoglobin level corresponds to the TIMI classification.10^,^15^,^18 BARC class 3b or greater contains more components than the TIMI classification and is therefore likely to report higher major bleeding incidences.15^,^18^,^26 Accurate bleeding classification validated for PAD patients is lacking but of interest to predict outcomes and compare APT among studies.
This safety update has a few limitations. The trial was powered for its efficacy endpoint, which did not include major bleeding. Consequently, some relevant factors for bleeding events are missing, such as the sheath size and the vascular closure devices used, which is of interest since most bleeding events found in this analysis were found in the first 30 days. This safety analysis has a substantial proportion of missing data due to competing events and incomplete follow up. Moreover, following the CLEAR-PATH protocol, APT starts one day after EVR; therefore, post-procedural bleeding is not always associated with the APT.10
The CLEAR-PATH trial is on target, and the last patient is predicted to be enrolled in 2026 with the trial ending in 2027. Since the start of the CLEAR-PATH in 2023, limited literature has been published on APT in PAD patients following EVR. Moreover, a new guideline has recently affirmed this research gap and highlighted the importance of research in this specific area.1
Conclusion
CLEAR-PATH is an ongoing prospective trial building a unique, large, well phenotyped PAD cohort. The incidence of major bleeding under APT after EVR in PAD patients differed per classification, but was overall low, most seemed to occur in the first 30 days and were related to vascular procedures. The APT regimens used in CLEAR-PATH did not raise haemorrhagic safety concerns; therefore, this study continues per protocol.
Funding
The CLEAR-10.13039/100005624PATH study is funded by an independent grant provider 10.13039/501100001826ZonMw (dossier number: 80-84800-98-44023).
Conflict of interest
The authors have no (potential) conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Twine C.P.Kakkos S.K.Aboyans V.Baumgartner I.Behrendt C.A.Bellmunt-Montoya S.Editor's Choice – European Society for Vascular Surgery (ESVS) 2023 clinical practice guidelines on antithrombotic therapy for vascular diseases Eur J Vasc Endovasc Surg 6520236276893701927410.1016/j.ejvs.2023.03.042 · doi ↗ · pubmed ↗
- 2Aboyans V.Ricco J.B.Bartelink M.E.L.Björck M.Brodmann M.Cohnert T.Editor's Choice – 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS)Eur J Vasc Endovasc Surg 5520183053682885159610.1016/j.ejvs.2017.07.018 · doi ↗ · pubmed ↗
- 3Conte M.S.Bradbury A.W.Kolh P.White J.V.Dick F.Fitridge R.Global vascular guidelines on the management of chronic limb-threatening ischemia Eur J Vasc Endovasc Surg 581s 2019 S 1S 109.e 333118233410.1016/j.ejvs.2019.05.006PMC 8369495 · doi ↗ · pubmed ↗
- 4Gerhard-Herman M.D.Gornik H.L.Barrett C.Barshes N.R.Corriere M.A.Drachman D.E.2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary Vasc Med 222017 Np 1Np 432849471010.1177/1358863 X 17701592 · doi ↗ · pubmed ↗
- 5Gottsäter A.The European Society for Vascular Surgery (ESVS) 2023 clinical practice guidelines on antithrombotic therapy for vascular diseases: an indispensable resource in vascular care Eur J Vasc Endovasc Surg 6520236216223694848410.1016/j.ejvs.2023.03.032 · doi ↗ · pubmed ↗
- 6Nordanstig J.Behrendt C.A.Baumgartner I.Belch J.Bäck M.Fitridge R.Editor's Choice – European Society for Vascular Surgery (ESVS) 2024 clinical practice guidelines on the management of asymptomatic lower limb peripheral arterial disease and intermittent claudication Eur J Vasc Endovasc Surg 6720249963794980010.1016/j.ejvs.2023.08.067 · doi ↗ · pubmed ↗
- 7Eikelboom J.W.Mehta S.R.Anand S.S.Xie C.Fox K.A.Yusuf S.Adverse impact of bleeding on prognosis in patients with acute coronary syndromes Circulation 11420067747821690876910.1161/CIRCULATIONAHA.106.612812 · doi ↗ · pubmed ↗
- 8Mehran R.Pocock S.J.Stone G.W.Clayton T.C.Dangas G.D.Feit F.Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes: a risk model from the ACUITY trial Eur Heart J 302009145714661935169110.1093/eurheartj/ehp 110PMC 2695951 · doi ↗ · pubmed ↗