Abdominal-based vs. alternative flaps: Surgical outcomes and quality of life following different techniques of autologous breast reconstruction
Lisanne Grünherz, Stella Vocke, Laura C. Siegwart, Victoria Wlach, Anna Burger, Pietro Giovanoli, Nicole Lindenblatt, Duveken B.Y. Fontein

TL;DR
This study compares surgical outcomes and quality of life for two types of breast reconstruction techniques and finds both are viable options with similar patient satisfaction.
Contribution
The study provides empirical evidence on the comparative outcomes of abdominal-based versus alternative flaps in autologous breast reconstruction.
Findings
No significant relationship was found between flap type and flap complications.
Abdominal-based flaps had more donor-site complications and secondary aesthetic surgery.
Patient satisfaction was similar between abdominal-based and alternative flap types.
Abstract
Abdominal-based flaps are considered the gold standard for autologous breast reconstruction (ABR). With the increasing number of women undergoing mastectomy, however, alternative free flaps from other regions have emerged as valuable alternatives when patients do not qualify for an abdominal-based flap. This single-center cohort study evaluates objective and subjective outcomes in patients who underwent abdominal-based versus alternative flaps for breast reconstruction. Patients who underwent ABR between 2010 and 2022 were included. Baseline patient characteristics and data on oncological and surgical treatment were collected. Since 2018, all patients received the validated BREAST-Q questionnaire evaluating satisfaction and quality of life preoperatively and at regular intervals following surgery. Multinomial logistic regression evaluated the probability of flap complications based on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1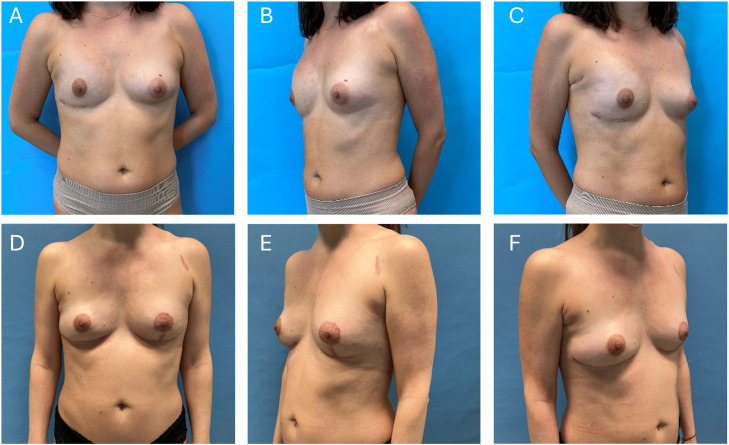 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Breast Implant and Reconstruction · Surgical site infection prevention
Introduction
Microsurgical, free flap Autologous breast reconstruction (ABR) has emerged as a very reliable option for women after mastectomy without the risk of implant-associated complications. Further advantages include a natural breast shape and feel with the unique chance to combine optimized shaping and sizing of the breast with a body contouring donor site procedure.1, 2, 3, 4 A growing body of literature has also demonstrated its positive impact on quality of life and psychosocial well-being.5
Since it was first described by Koshima in 1989, the deep inferior epigastric perforator (DIEP) flap has become the gold standard for ABR.6 Unlike traditional methods that are based on the use of the rectus abdominis muscle, the DIEP flap preserves the abdominal muscles, minimizing postoperative complications and promoting a faster recovery. A further refinement in the transfer of lower abdominal tissue is the superficial inferior epigastric artery (SIEA) flap that does not require any incision of the rectus abdominis fascia or muscle leaving these structures completely untouched.7
Considering the increasing number of women undergoing either therapeutic or risk-reducing mastectomies and subsequent reconstruction, alternative free flaps from the thigh, buttock or lower back such as the profunda artery perforator flap (PAP), transverse myocutaneous gracilis (TMG), or the superior gluteal artery perforator flap (SGAP) flap have emerged as valuable alternatives for women with insufficient abdominal donor-site tissue.8^,^9 In recent years, a 31 % increase in perforator flaps from the thigh and lower back has been reported for ABR.10 While the DIEP flap still remains the gold standard, the most suitable flap is based on an individual's anatomy as well as patient’s and surgeon’s preferences. The objective of this study was to evaluate surgical outcomes and patient satisfaction and quality of life in patients who underwent ABR with abdominal-based flaps versus alternative flap types between 2010 and 2022.
Material and methods
Patient collective
We conducted a single center observational study on all patients who underwent ABR at the Department of Plastic Surgery and Hand Surgery between 2010 and 2022 at the University Hospital of Zürich, Switzerland. Ethical approval was given by the Cantonal Ethics Committee of Zurich, Switzerland (Ethical approval Nr.: 2021-01591 and 2018-02058). Written informed consent was obtained from all patients. Since 2018, all patients received the BREAST-Q preoperatively as well as at 6 weeks, 6 months, 12 months, and 24 months postoperatively. Exclusion criteria for the BREAST-Q included patients who were not able to complete questionnaires due to insufficient knowledge of the German or English language, impaired psycho-intellectual abilities or any psychiatric disorder. These patients were only included for an analysis of their patient characteristics and surgery details, provided written informed consent for the use of data was given.
Medical records were analyzed with respect to patients characteristics including age, body mass index (BMI), current history of smoking, reason for mastectomy, genetic predisposition to breast cancer, irradiation, chemotherapy, history of abdominal operations, concomitant diseases, timing for breast reconstruction, flap technique, length of surgery, flap weight, flap and donor-site complications as well as refinement operations.
Statistical analysis
Statistical analysis of patients’ baseline characteristics was performed using descriptive and summary statistics to identify a central tendency. Data was analyzed using IBM SPSS Statistics Version 29 (IBM, Armonk, NY, USA), Microsoft® Excel Version 14.3.6. (Microsoft Corp., Redmond, WA, USA) and GraphPad Prism Version 7.04 (GraphPad, La Jolla, CA, USA). We performed binary and multinomial logistic regression analyses (confidence intervals [CI] were set at 95 %, p-values <0.05 were considered statistically significant) to assess the likelihood of flap and/or donor-site complications in relation to flap type. We adjusted our analyses for the following confounders: obesity, smoking and prior radiotherapy. Patients with missing data for specific variables were excluded from analyses requiring those specific variables.
Quality of life was assessed using the BREAST-Q® (German Version).11 The content and design of the questionnaire are protected by U.S. and international intellectual property laws, and use was made under a license from Memorial Sloan Kettering Cancer Center, New York, NY, USA. For further information on permitted use. Data from the BREAST-Q® questionnaires were evaluated using the designated software program Q-Score (Copyright © 2012, Memorial Sloan Kettering Cancer Center and the University of British Columbia).12 Measures were linearly converted to a 0–100 scale. Differences in BREAST-Q outcomes between patients who underwent abdominal-based flaps and alternative flaps were analyzed using independent samples T-tests for normally distributed data and the Mann-Whitney U Test for non-normally distributed data. Fisher’s exact test was performed to compare two categorical variables and Chi-square test for three or more categorical variables. Confidence intervals were set at 95 %. A p-value of <0.05 was considered statistically significant. The manuscript was checked against the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (supplemental Appendix: STROBE Checklist).
Results
We included 183 patients who underwent ABR between 2010 and 2022. Baseline characteristics of patients included in this study are depicted in Table 1. Of the 146 patients received an abdominal-based free flap, while in 37 patients the free flap was harvested from alternative donor-sites (thigh, gluteal, others). Both immediate and delayed reconstructions (122 and 98 respectively) as well as unilateral and bilateral (146 and 37 respectively) reconstructions were included in this study. In this study, abdominal-based flaps included DIEP (n = 152), MS-TRAM (n = 20), SIEA (n = 5), and TRAM (n = 1) flaps, whilst alternative flap types consisted of TMG (n = 19), PAP (n = 15), SGAP (n = 2), IGAP (n = 1), and PMT (n = 5). Figure 1 depicts an abdominal-based flap type (DIEP) and Figure 2 an alternative flap (PAP-flap) type. Mean age of patients included in this study was 49.3 years (SD 9.1) for abdominal-based flaps and 47.1 years (SD 11.1) for alternative flap types and did not show a statistically significant difference. Descriptive analysis of breast cancer characteristics, including primary or recurrent disease, therapeutic or risk-reducing mastectomy and genetic predisposition showed an equal distribution between the groups. There was also no difference regarding relevant risk factors. As expected, a lower BMI was noted in patients who received an alternative free flap (22.2 kg/m^2^ ± 3.3 vs. 25.6 kg/m^2^ ± 3.6, p < 0.0001). In most patients (N = 122) an immediate ABR was performed in a two-team approach with the gynecologist. The alternative flaps also had a significantly lower flap weight when compared with the abdominal-based group (320 g ± 160 g vs. 585 g ± 222 g, p < 0.0001).Table 1. Baseline characteristics of patients included in this study.Table 1. VariableAbdominal-basedAlternativep-valueN%N%Patients14637Flaps17842 TRAM1<1 MS-TRAM2011 DIEP15285 SIEA53 TMG1945 PAP1535 SGAP25 IGAP12 PMT512Age [years], mean (SD)49.39.1047.111.100.20Age [years] <200000 20–4017121130 40–60113772259 >601611411BMI [kg/m^2^], mean (SD)25.63.622.23.30.0001BMI [kg/m^2^] 15–19.932821 20–24.962422568 25–29.9584038 30–34.9221500 ≥351<113Breast cancer Primary disease119823086 Recurrent disease2114514Risk factors Diabetes mellitus43130.9 Obesity (BMI ≥ 30 kg/m^2^)2316130.04 Active smoker322210270.52 Preoperative chemotherapy765217460.58 Preoperative radiotherapy553712320.7Flaps17842 Unilateral1147832860.36 Bilateral3222514Breast reconstruction Immediate985524570.86 Delayed80451843Flap weight [g], mean (SD)5852123201600.0001Operation time [min], mean (SD) Unilateral392102366**900.19 Bilateral572219612**1140.36BMI, body mass index; SD, standard deviation.Figure 1(A-C) Preoperative photographs of a 62-year-old woman with a local recurrence of a breast carcinoma to the right breast. (D-F) 16 months after right-sided nipple-sparing mastectomy plus autologous breast reconstruction with a DIEP flap. Refinements included removal of the skin island of the DIEP flap in the inframammary fold and a left sided mastopexy.Figure 1. Figure 2(A-C) Preoperative pictures of a 37-year-old woman with capsular contracture after immediate implant-based reconstruction after nipple-sparing mastectomy of her right breast. (D-F) 12 months after autologous breast reconstruction with a PAP flap and mastopexy of the left breast. During the further course the skin island of the PAP flap, located in the submammary fold, was removed. At the same time bilateral lipofilling was performed.Figure 2
Flap complications
Seven abdominal-based flaps and one alternative flap suffered partial necrosis. Complete flap loss was noted in 5 patients (2.7 %) (three abdominal-based (2 %) and two other flap types (5.4 %), p = 0.469). We performed both adjusted and unadjusted multinomial logistic regression analyses to evaluate the probability of flap complications (partial or complete flap loss) based on the type of flap used. No relationship between the type of free flap and the odds of flap complications (partial or complete flap loss) could be ascertained. Unadjusted analyses revealed an odds ratio of 1.711 (95 % CI: 0.203–14.393, p = 0.621) for partial flap loss in abdominal-based flaps and 0.367 (95 % CI: 0.059–2.284, p = 0.282) for complete flap loss. Correcting for possible confounders (preoperative radiotherapy, obesity, smoking status and timing of reconstruction) did not alter the results (Table 2).Table 2. Odds ratios of flap complications and revisional surgery in patients who underwent abdominal-based versus other free flaps.Table 2. VariablePartial flap loss (n = 8)Complete flap loss (n = 5)Complications requiring revisional surgery (n = 35)Odds RatioConfidence Interval (95 %)p-valueOdds RatioConfidence Interval (95 %)p-valueOdds RatioConfidence Interval (95 %)p-valueUnadjusted analysesFlap typeabdominal-based (ref)1.001.001.00other free flaps1.710.203–14.3930.6210.370.059–2.2840.2820.1960.045–0.8570.030Adjusted analysesFlap typeabdominal-based (ref)1.001.001.00other free flaps1.780.203–15.5480.6030.290.041–2.0590.220.2260.051–1.0040.051TimingImmediate (ref)1.001.001.00Delayed2.500.407–15.3770.3221.520.231–9.9430.670.7940.331–1.9010.604Prior radiotherapyNo (ref)1.001.001.00Yes2.020.390–10.5040.401n/an/an/a1.5140.620–3.6950.363ObesityNo (ref)1.001.001.00Yes0.780.085–7.0890.8223.350.304–36.8560.322.0640.769–5.5360.150Smoking statusNon-smoker (ref)1.001.001.00Smoker1.180.221–6.3330.8452.870.423–19.4250.280.7680.287–2.0590.60n/a, not applicable.
Donor-site morbidity
Of the 33 patients (22.6 %) who underwent abdominal-based free flaps and 2 patients (5.4 %) who had alternative flaps required surgical revision of the donor site (p = 0.018). Most common donor-site complications for abdominal-based flaps included seroma (n = 15), bulging (n = 3), and wound-breakdown (n = 2). Logistic regression analyses were performed to assess the likelihood of donor-site complications requiring revision surgery based on the type of flap used. Abdominal-based flaps were associated with more donor-site complications requiring surgical revision (OR 0.196 (95 % CI 0.045–0.857, p = 0.03) when compared to alternative flaps. After adjusting for possible confounders, the results just did not reach statistical significance. None of the possible confounders showed a statistically significant effect on the risk of donor-site complications (Table 2).
Refinement surgery
The analysis of touch-up procedures showed that 45.2 % of patients (n = 66) in the abdominal-based free flap group and 45.9 % of patients (n = 17) in the alternative free flap group received additional lipofilling of the reconstructed breast (p = 0.94) (Supplementary Table 1). Regarding other flap types, both TMG und PAP flaps showed similar numbers of lipofilling sessions (TMG vs PAP: 9 (56.3 %) vs. 6 patients (46.2 %), Pearson chi-squared p = 0.588). The number of sessions ranged from 1 to 4 with a mean of 1.5 sessions in both groups. Other touch-up procedures, including nipple reconstruction, scar correction and liposuction, were slightly more common in patients after an abdominal-based free flap breast reconstruction. Symmetrization surgery of the contralateral breast was performed in 51 abdominal-based flap patients (36.1 %) and in 11 (33.4 %) alternative flap patients (p = 0.759). Regarding donor-sites, we observed more aesthetic corrections of the abdominal donor-site than other donor sites (26.7 % vs. 5.4 %, p = 0.004).
Patient-reported outcome measures
BREAST-Q Questionnaires were sent preoperatively and at regular intervals after the surgery. Twenty-one patients completed at least one postoperative BREAST-Q Questionnaire (13 abdominal-based flaps and eight alternative flaps). Our results did not show any differences in the domains ‘satisfaction with outcomes’ and ‘satisfaction with breasts’ between patients who underwent abdominal-based breast reconstruction and patients who had alternative flaps. Well-being domains (psychosocial, sexual, and physical) also did not show differences in scores between the abovementioned groups (Table 3). Patient numbers were too small to evaluate differences between subgroups of patients.Table 3. Satisfaction and quality of life results in patients with abdominal versus other free flap types.Table 3. Adjusted analysesAbdominal-based (n = 13)Other free flaps (n = 10)p-valuemeanSDmeanSDSatisfaction with breasts63.3119.0069.2515.110.463Satisfaction with outcome71.8323.1980.5015.320.366Satisfaction with nipples60.4435.2543,0037,320.48*Psychological well-being77.2322.6979.2521.690.916⁎⁎physical well-being (chest)69.2313.4875.1315.920.50⁎⁎Sexual well-being54.6424.9163.5723.740.425⁎⁎Satisfaction with information67.3121.3172.0017.120.456⁎⁎Satisfaction with surgeon81.6218.0492.6314.090.185⁎⁎SD, standard deviation.⁎independent samples T-Test.⁎⁎Mann-Whitney U Test.
Discussion
This study focuses on differences in surgical and quality-of-life outcomes in patients who underwent abdominal-based versus alternative flaps for ABR. Flap complications were similar for both abdominal-based and alternative flap types, although donor-site morbidity was higher in abdominal-based flaps. Patient-satisfaction, however, did not differ based on the type of free flap used.
In this study, we aimed to evaluate the BREAST-Q outcomes between patients based on flap type. Our results showed similar levels of patient-satisfaction and well-being throughout various domains of the BREAST-Q. Especially with respect to psychosocial and sexual well-being, our findings reflect that both abdominal-based and alternative flap types are acceptable options that can meet patients’ expectations. This finding likely reflects optimal patient selection and individualized surgical planning. The appropriate flap type should be chosen based on a patient’s body shape and composition, donor site availability, patient preferences and overall reconstructive goals.10^,^13^,^14 Consequently, when a patient’s functional and aesthetic needs are met, both abdominal-based and alternative flap types, when properly selected and executed, can result in similarly high satisfaction levels across all domains addressed by the BREAST-Q. Although not all patients completed a 24-month follow-up questionnaire, the time after surgery was long enough for complete healing and adaptation, during which patients were able to adapt to their reconstruction outcomes and long-term benefits to become apparent, regardless of flap type.
We observed a higher number of patients undergoing surgical revision of the abdominal donor-site. This is in line with Weitgasser et al. who found an increased donor-site morbidity of 23 % after double DIEP flap harvest compared with 16 % after double TMG for ABR.15 In contrast to the aforementioned study, however, other authors reported a significantly lower rate of abdominal donor-site complications in comparison with the thigh after PAP flap harvest.16^,^17 Aesthetic correction of the donor-site, however, was almost twice as high as after PAP flap harvest.16 Although, focus on improving the donor-site after DIEP flap harvest has steadily grown, aesthetically unpleasant scars as well as abdominal wall weakness are still observed in up to 30 % of the patients.15^,^18, 19, 20, 21 In 2020, we proposed an algorithm to reduce donor site morbidity and improve the aesthetic appearance of the abdominal scar, including meticulous donor site closure and careful perforator selection based on preoperative CT angiography and surgical evaluation.21 We believe that proper patient selection, considering patients with a normal to slightly elevated BMI, a local fat deposition in the lower abdomen and abdominal skin redundancy for DIEP flap harvest, are important aspects to optimize donor-site morbidity.
Women with a remarkably lower BMI tend to undergo ABR with an alternative free flap.22^,^23 Not surprisingly, this results in a lower overall flap weight, which is reflected in our results and was also observed in other studies.15^,^16 In this context, Weichman et al. showed that this flap weight was sufficient to provide body-appropriate breast volume in the low BMI patient collective.22
Interestingly, there was no difference in the number of touch-up procedures, particularly number of lipofilling sessions after using an abdominal-based versus alternative free flap for ABR. To the best of our knowledge, we only found one study comparing the number of touch-up procedures after different techniques of ABR. In contrast to our results, they reported a higher number of lipofilling sessions after ABR with TMG flaps compared with DIEP flaps, which might be attributed atrophy of the gracilis muscle and consecutive shrinkage of the flap.15 Furthermore, the choice of free flap is determined not only by available donor tissue and body composition, but also by the inherent advantages of different flap types. The DIEP flap’s versatility in inset techniques allows surgeons to optimize aesthetic outcomes through various shaping methods.1^,^2^,^24^,^25 Similarly, other flap types offer their own unique advantages and can achieve comparable outcomes when chosen for the appropriate patient, suggesting that the comparable numbers of refinement procedures reflect appropriate flap selection rather than limitations in any particular technique.
The results of our study need to be contextualized with the limitations arising from our relatively small sample size of patients who received alternative free flaps. In our study, 146 patients received an abdominal-based flan versus 37 alternative flap types. Consequently, the higher use of abdominal-based flaps may bias the comparative power of complication rates and PROMs, especially as response-rates to the questionnaires in this study were relatively low. For this reason, the results of the BREAST-Q are exploratory at most. A strength of this study, however, is the prospectively collected BREAST-Q, which was sent to patients preoperatively as well as postoperatively at various time intervals after surgery, potentiating more generalizable results once longer follow-up becomes available.
To conclude, although the DIEP flap is commonly referred to as the gold standard for breast reconstruction, both abdominal-based and alternative free flap types are viable treatment options in ABR and several variables need to be taken into account when selecting the appropriate free flap. The choice of free flap should ideally take into account multiple other factors, such as patient-preference, surgeon preference and experience, body composition and the availability of an acceptable donor-site as well as potential contraindications for an abdominal-based flap.10^,^13^,^26^,^27 Patients who are involved in a shared decision-making process are more likely to have better health outcomes and more satisfaction with their care.28^,^29 Understanding and discussing patient-preferences, expectations and surgical treatment options is imperative and plays a significant role in treatment decisions.30 Our findings underline the importance of integrating shared decision-making between patient and surgeon into the choice of flap type, aiming to provide more personalized, high-quality patient care.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical approval
Ethical approval was given by the Cantonal Ethics Committee of Zurich, Switzerland (Ethical approval No.: 2021-01591 and 2018-02058).
Declaration of competing interest
Nicole Lindenblatt acts as consultant and scientific advisor for Medical Microinstruments (MMI). All other authors have no financial interests/personal relationships to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Razzano S.Marongiu F.Wade R.Figus A.Optimizing DIEP Flap Insetting for Immediate Unilateral Breast Reconstruction: A Prospective Cohort Study of Patient-Reported Aesthetic Outcomes Plast Reconstr Surg 1432019261 e 270e 10.1097/PRS.000000000000527730688877 · doi ↗ · pubmed ↗
- 2Morelli Coppola M.Schaffer C.Jaber G.J.Sapino G.di Summa P.G.Maximizing Aesthetic Outcomes in Delayed Breast Reconstruction: the Be.A.U.T-I.F.U.L. DIEP((R)) Step-by-Step Inset Technique Aesthetic Plast Surg 492025195919623962323010.1007/s 00266-024-04502-3PMC 12031832 · doi ↗ · pubmed ↗
- 3Fischer J.P.Nelson J.A.Cleveland E.Breast reconstruction modality outcome study: a comparison of expander/implants and free flaps in select patients Plast Reconstr Surg 13120139289342362907410.1097/PRS.0b 013e 3182865977 · doi ↗ · pubmed ↗
- 4Kadhum M.Symonette C.Javed MU.Inset techniques for the DIEP flap - what improves aesthetic outcomes?Acta Chir Plast 66202410153870423110.48095/ccachp 202410 · doi ↗ · pubmed ↗
- 5Yueh J.H.Slavin S.A.Adesiyun T.Patient satisfaction in postmastectomy breast reconstruction: a comparative evaluation of DIEP, TRAM, latissimus flap, and implant techniques Plast Reconstr Surg 1252010158515952051708010.1097/PRS.0b 013e 3181 cb 6351 · doi ↗ · pubmed ↗
- 6Koshima I.Soeda S.Inferior epigastric artery skin flaps without rectus abdominis muscle Br J Plast Surg 421989645648260539910.1016/0007-1226(89)90075-1 · doi ↗ · pubmed ↗
- 7Grunherz L.Wolter A.Andree C.Autologous Breast Reconstruction with SIEA Flaps: An Alternative in Selected Cases Aesthetic Plast Surg 4420202993063181134110.1007/s 00266-019-01554-8 · doi ↗ · pubmed ↗
- 8Jonczyk M.M.Jean J.Graham R.Chatterjee A.Surgical trends in breast cancer: a rise in novel operative treatment options over a 12 year analysis Breast Cancer Res Treat 17320192672743036187310.1007/s 10549-018-5018-1PMC 6486837 · doi ↗ · pubmed ↗