Inequity in Access to and Use of Digital Health Technologies in Routine Heart Failure Care: Protocol for a Scoping Review
Nicklas Vinter, Mariam Elmegaard, Lars Køber, Morten Schou, Søren Paaske Johnsen

TL;DR
This study will investigate how access to digital health tools for heart failure care varies by socioeconomic status, geography, and race, aiming to identify gaps in equitable use.
Contribution
The novelty lies in systematically mapping evidence on disparities in digital health technology access for heart failure care.
Findings
The review will identify patterns in access to digital health technologies for heart failure.
It will highlight gaps in the literature regarding socioeconomic and racial disparities.
Findings will inform strategies for equitable implementation of digital health tools.
Abstract
Heart failure (HF) is a global health challenge characterized by high mortality, morbidity, and economic burden. The development of digital health technologies offers promising tools for prevention, early detection, and management of HF, potentially improving prognoses and reducing costs. However, these innovations may also widen existing health disparities related to socioeconomic status, geography, and race/ethnicity. This scoping review will examine and map existing evidence on socioeconomic, geographic, and racial/ethnic differences in access to and use of digital health technologies for HF care in routine practice. The writing of this protocol followed the methodological framework by Arksey and O’Malley, including (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies to be included in the review; (4) charting the data; and (5) collating,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
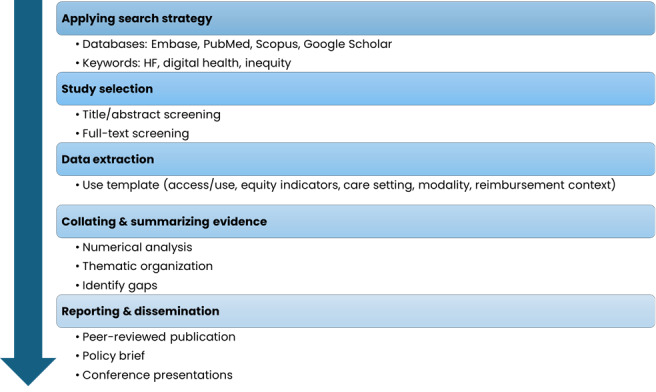 Figure 1
Figure 1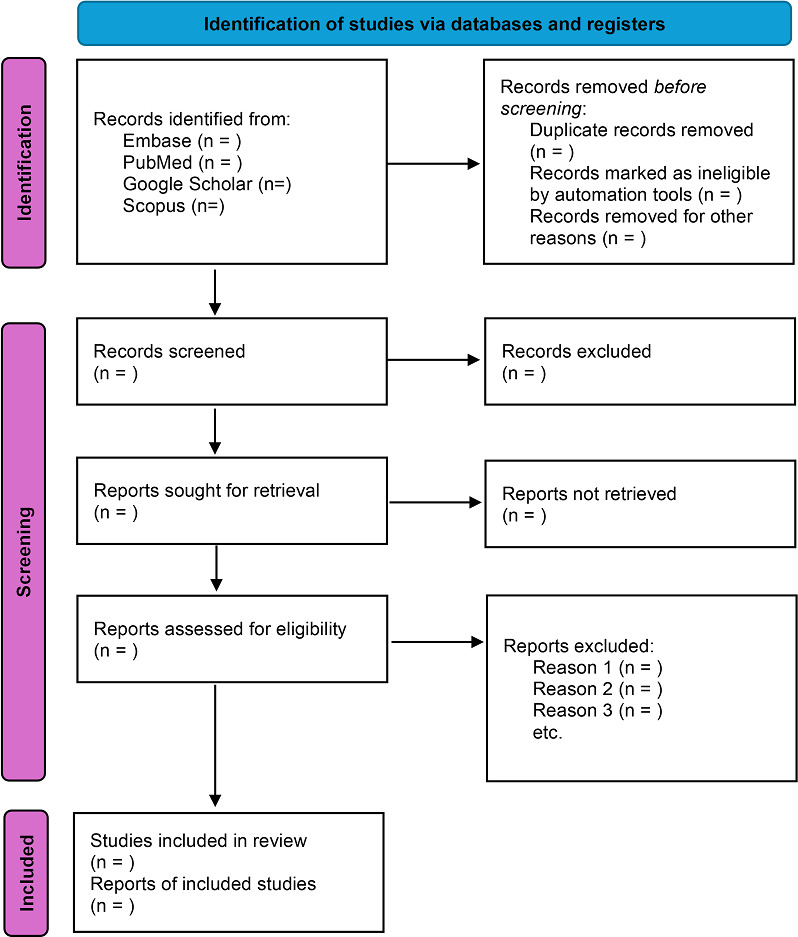 Figure 2
Figure 2| Data domain | Definition |
|---|---|
| Social determinants of health |
Insurance Income/wealth Marital status Educational attainment Neighborhood socioeconomic status Social support Employment status Health literacy |
| Geography |
Urban/rural residency Distance to hospital Administrative regions |
| Race and ethnicity |
Any group |
| Number | Topic | Database | |||
|---|---|---|---|---|---|
| Embase | PubMed | Google Scholar | Scopus | ||
| 1 |
| “heart failure”/exp OR “heart failure” | “Heart Failure” [Mesh] OR “heart failure” | “heart failure” | “heart failure” |
| 2 | Digital health intervention | (“digital intervention”/exp OR “digital intervention” OR (“digital” AND (“intervention”/exp OR “intervention”))) OR (“digital health”/exp OR “digital health”) OR (“mobile application”/exp) (“information technology device”/exp) OR (“digital technology”/exp) OR (“telehealth”/exp) OR (“mhealth”/exp) OR “mhealth” OR “mobile health” | “Telecommunications” [Mesh] OR “digital intervention” OR “digital health intervention” OR (“digital” AND “intervention”) OR “mHealth” OR “mobile health” | “digital intervention” OR “mHealth” OR “mobile health” | “digital intervention” OR (“digital” AND “intervention”) OR “mHealth” OR “mobile health” |
| 3 | Health inequity | “health disparity”/exp OR “disparity in health” OR “health disparities” OR “health economic disparity” OR “health inequality” OR “health inequities” OR “health inequity” OR “health social disparity” OR “health social economic disparity” OR “health social inequality” OR “health socio-economic disparity” OR “health socioeconomic disparity” OR “health socioeconomic inequity” OR “health status disparities” OR “health status disparity” OR “health status inequality” OR “health status inequity” OR “inequality in health” OR “inequity in health” OR “socioeconomic disparities in health” OR “health disparity” | “Health Inequities” [Mesh] OR “inequity” OR “inequities” OR “disparity” OR “disparities” | “inequity” OR “disparity” | “inequity” OR “inequities” OR “disparity” OR “disparities” |
| 4 | Social determinants of health | “social determinants of health”/exp OR “social determinant” OR “social determinants” OR “social determining factor” OR “social factors determining health” OR “social health determinant” OR “social determinants of health” | “Social Determinants of Health” [Mesh] OR “social determinant of health” | “Social Determinants of Health” | “Social Determinants of Health” OR “social determinant of health” |
| 5 | Geographic variation | “geography”/exp OR “geographic factor” OR “geographic locations” OR “geography” OR “geography”/exp OR “geographic factor” OR “geographic locations” OR “geography” OR “geographic distribution”/exp OR “distribution, geographic” OR “geographical distribution” OR “geographic distribution” OR “geographic variation”/exp OR “urban area”/exp OR “built-up area” OR “built-up land” OR “urban environment” OR “urban land” OR “urbanized area” OR “urbanized environment” OR “urbanized land” OR “urbanized area” OR “urbanized environment” OR “urbanized land” OR “urban area” OR “rural area”/exp OR “agricultural area” OR “rural environment” OR “rural land” OR “rural area” | “Population” [Mesh] OR “geographic variation” OR “geography” | — | “geography” OR “geographic variation” OR “rural” OR “urban” |
| 6 | Race/ ethnicity | “ethnic group”/exp OR “ethnic and racial groups” OR “ethnic and racial minorities” OR “ethnic groups” OR “ethnic minorities” OR “ethnic minority” OR “ethnic origin” OR “ethnic population” OR “ethnic status” OR “ethno-linguistic group” OR “ethnolinguistic group” OR “ethnic group” | “Ethnicity” [Mesh] OR “ethnicity” OR “ethnic” OR “Racial Groups”[Mesh] OR “race” | — | “ethnicity” OR “ethnic” OR “race” OR “racial” |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Mobile Health and mHealth Applications · Cardiac pacing and defibrillation studies
Introduction
Heart failure (HF) is a complex clinical syndrome that represents a considerable global health burden, characterized by high mortality, morbidity, and costs [12]. The development of digital health technologies for HF is expanding, supporting primary prevention, early detection, and disease management [34], and recent reviews highlight the growing role of remote monitoring, wearable technologies, and integrated care models [5-8]. Application of digital health tools in health care services and decision-making has the potential to improve patient care and clinical outcomes and reduce health care expenditures. However, comprehensive investigations are needed to understand the broader implications, including ethical, practical, and systemic concerns, associated with implementation.
Understanding the consequences for health equity of implementing digital health technologies is essential [9]. Health inequities based on socioeconomic status, race/ethnicity, and geography remain a significant challenge in HF care. Inequities can lead to unequal health outcomes, with certain groups experiencing higher rates of hospitalization, poorer quality of life, and increased risk of adverse clinical outcomes [10-14]. While digital health innovations may offer new opportunities for care delivery, uneven access and use across population groups could exacerbate existing inequities. Recent work emphasizes the need for equity frameworks in digital health implementation [15].
Without deliberate efforts to ensure equitable implementation, the digital transformation of health care risks reinforcing or even widening inequities [1617], yet the extent and nature of evidence available in the literature regarding patients with HF remain unclear. To address this gap, we will conduct a scoping review of digital health technologies used in HF care. The objective of this scoping review is to map and synthesize what is known from existing literature about socioeconomic, geographic, and racial/ethnic differences in access to and use of digital technologies in routine clinical practice among individuals with HF. We hypothesize that individuals from underserved socioeconomic groups, rural or remote areas, or racial/ethnic minority groups have lower access to and use of digital health technologies.
Methods
Overview
The approach follows the methodological framework by Arksey and O’Malley [18] and incorporates refinements proposed by Levac et al [19] and guidance from the Joanna Briggs Institute (JBI) for scoping reviews to enhance methodological rigor [20]. We will adhere to the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) checklist when reporting the review [21]. This protocol was preregistered at Open Science Framework [22]. Figure 1 illustrates the overall workflow of the scoping review.
Overview of the scoping review workflow. HF: heart failure.
Eligibility Criteria
Textbox 1 summarizes the inclusion and exclusion criteria. We will include studies on individuals aged ≥18 years with any type of HF that report on any digital health technology. We will use the World Health Organization (WHO) definition of “digital health intervention,” which states that such an intervention involves the use of digital technology to achieve specific health-related objectives, and that it is integrated into digital health applications and information and communication technology systems [9]. Data on social determinants of health, geography, and race/ethnicity must also be present in the studies. The selection of the social determinants of health was inspired by previous studies on HF (Table 1) [23]. Any study with an observational design is eligible, because this design reflects real-world access and use patterns in routine practice. Randomized controlled trials and qualitative-only studies are excluded as they often occur in controlled settings that may mask real-world inequities. Eligible studies must provide data on access to or use of the digital health technology. We will place no restriction on the calendar year of publication. Finally, we will include only full-text articles published in English in peer-reviewed journals. The restriction is due to resource limitations for translation and to ensure methodological rigor. We acknowledge that this may introduce language and publication bias, which will be discussed as a limitation.
Textbox 1.Inclusion and exclusion criteria. Inclusion criteria
- Adults (≥18 years) with any type of heart failure
- Studies reporting on digital health technologies (World Health Organization definition)
- Observational studies (cross-sectional, cohort, case-control)
- Studies that report social determinants of health, geography, or race/ethnicity
- Full-text articles published in English in peer-reviewed journals
- Any publication year
Exclusion criteria
- Randomized controlled trials, qualitative-only studies
- Conference abstracts, editorials, letters, non–peer-reviewed sources
- Non–English language publications
Search Strategy and Information Sources
A professional health care librarian was consulted to build the search strategy (Table 2). Our search strategy combines HF and digital health technology, and then either inequity, social determinants of health, geography, or race/ethnicity. Databases to be searched include Embase, PubMed, and the interdisciplinary sources Google Scholar and Scopus.
Study Selection
Two independent reviewers (NV and ME) will use a 2-step screening approach. First, all identified records will be manually screened for eligibility based on titles and abstracts. Second, the full-text reports of the qualifying abstracts will be assessed for eligibility. Finally, the 2 reviewers will screen the list of references of the selected studies. Any inconsistencies will be resolved by formal consensus, which will involve SPJ.
Collecting and Charting Data
Based on the identified literature, NV and ME will independently extract data following the data charging form: (1) authors and year of publication (2); study design and population; (3) aims of the study (4); study location and calendar period; (5) care setting (eg, inpatient, outpatient, or home-based); (6) digital health technology modality; (eg, telemonitoring, mobile app, or wearable); (7) operational definitions of “access” (availability and ability to obtain or use technology) and “use” (actual engagement or use); (8) equity indicators (income, education, race/ethnicity, geography, and insurance status); (9) reimbursement and connectivity context (insurance coverage, internet access, and device ownership); (10) primary outcome measure; (11) main findings, reported according to age, sex, socioeconomic characteristics, geographic characteristics, and race/ethnicity.
Collating, Summarizing, and Reporting the Results
We will systematically organize and present the findings.
Numerical Analysis
Reported measures of association (eg, odds ratios, risk ratios, and hazard ratios) will be tabulated and organized by age, sex, social determinants, geography, and race/ethnicity to examine patterns of inequity. Relevant measures of association may be, for example, high-income vs low-income or urban vs rural residency. We will consider differences in health outcomes as health inequities if they are systematic, avoidable, unnecessary, unfair, and unjust [24]. No meta-analysis or pooled effect estimates will be performed; findings will be summarized narratively.
Thematic Organization
Data from each identified study will be reported by type of digital intervention, which will follow the WHO classification. The WHO classification includes interventions for patients with HF (referred to as clients by the WHO), interventions for health care providers, interventions for health systems or service managers, and interventions for data services [25]. The relevance of the WHO classification system lies in its ability to link interventions with a list of health system challenges, thereby illustrating how technology may address health care needs. Furthermore, it provides easy access to results for researchers planning new randomized controlled trials. Data charting will follow the iterative process recommended by the JBI. We will first pilot the data charting form on a small sample of included studies to ensure all relevant variables (eg, equity indicators and digital modality) are captured. Next, we will refine the form by adding or adjusting fields as new concepts emerge during extraction.
Identification of Research Gaps
We will highlight areas where research is lacking or where findings are inconsistent. Stakeholder consultation will be integrated during interpretation of findings to validate relevance and identify gaps. This will involve engaging clinicians only, who will review preliminary findings and provide input on practical implications.
Methodological Appraisal
To contextualize our interpretation of inequities, we will include a structured appraisal of key methodological features using a checklist adapted from JBI guidance [20]. The appraisal will be descriptive and will not involve scoring or exclusion. The checklist will include the following domains:
Study designSample size adequacyCompleteness of equity-related reporting (eg, socioeconomic status, geography, race/ethnicity)Clarity of definitions for access and use
Findings from this appraisal will be summarized narratively to highlight major limitations and inform interpretation.
Results
The project is funded. Data collection is expected to begin by the beginning of 2026. A PRISMA 2020 flow diagram will be included in the final review to illustrate the study selection process. Figure 2 shows a blank version of the flowchart, which will be updated once screening and inclusion are completed.
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) flowchart.
Discussion
Anticipated Main Findings
This scoping review will map existing evidence on socioeconomic, geographic, and racial/ethnic differences in access to and use of digital health technologies for HF care. By synthesizing patterns across observational studies, the review aims to identify where inequities may exist and highlight gaps in the literature. The findings will inform future research and guide strategies for equitable implementation of digital health solutions in routine practice.
Future Directions
The review will identify patterns and gaps in the evidence base, informing the design of future studies and interventions aimed at reducing inequities in digital health adoption. Findings may also support policymakers and health care organizations in developing strategies to ensure equitable access to digital technologies for HF care.
Limitations
A key limitation of this review is the restriction to English-language, peer-reviewed full texts, which may introduce language and publication bias. The restriction is particularly relevant for equity-focused reviews, and future research should consider multilingual searches and inclusion of gray literature to minimize bias.
Dissemination Plan
Results will be disseminated through a peer-reviewed publication, policy briefs, and presentations at conferences and stakeholder meetings, ensuring accessibility to researchers, clinicians, and decision-makers.
Conclusion
The review will synthesize evidence on disparities in digital health adoption for HF care, offering insights to inform policy, practice, and research agendas aimed at reducing inequities. Findings will highlight gaps in current knowledge and support the design of interventions that promote inclusive digital health strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bragazzi NL Zhong W Shu J et al Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017 Eur J Prev Cardiol Dec 292021281516821690 doi 10.1093/eurjpc/zwaa 147Medline 33571994 · doi ↗ · pubmed ↗
- 2Virani SS Alonso A Aparicio HJ et al Heart disease and stroke statistics-2021 update: a report from the American Heart Association Circulation Feb 2320211438 e 254e 743doi 10.1161/CIR.0000000000000950 Medline 33501848 PMC 13036842 · doi ↗ · pubmed ↗
- 3Cowie MR Mc Beath KCC Angermann CE The digital future of heart failure care Curr Heart Fail Rep Jun 2022193109113 doi 10.1007/s 11897-022-00547-0Medline 35441250 PMC 9017407 · doi ↗ · pubmed ↗
- 4Farwati M Riaz H Tang WHW Digital health applications in heart failure: a critical appraisal of literature Curr Treat Options Cardiovasc Med 202123212 doi 10.1007/s 11936-020-00885-z Medline 33488049 PMC 7812033 · doi ↗ · pubmed ↗
- 5Azizi Z Broadwin C Islam S et al Digital health interventions for heart failure management in underserved rural areas of the United States: a systematic review of randomized trials J Am Heart Assoc 01162024132 e 030956 doi 10.1161/JAHA.123.030956 Medline 38226517 PMC 10926837 · doi ↗ · pubmed ↗
- 6Noci F Capodici A Nuti S Passino C Emdin M Giannoni A Wearable technologies to predict and prevent and heart failure hospitalizations: a systematic review Eur Heart J Digit Health Sep 202565868877 doi 10.1093/ehjdh/ztaf 079Medline 40984981 PMC 12450522 · doi ↗ · pubmed ↗
- 7Kallas D Sandhu N Gandilo C et al Use of digital health technology in heart failure and diabetes: a scoping review J Cardiovasc Transl Res Jun 2023163526540 doi 10.1007/s 12265-022-10273-6Medline 35639339 PMC 9153219 · doi ↗ · pubmed ↗
- 8Zwack CC Haghani M Hollings M et al The evolution of digital health technologies in cardiovascular disease research NPJ Digit Med 0132023611 doi 10.1038/s 41746-022-00734-2Medline 36596833 PMC 9808768 · doi ↗ · pubmed ↗