Interventions for Students’ Well-Being at the University of Helsinki (INSIGHT): Protocol and Preliminary Descriptive Results for a Quasi-Experimental Controlled Trial of a Social Identity Intervention and Two Active Comparators
Silja Martikainen, Oona Karhunen, Iiris Mankki, Vera Gergov, Päivi Berg, Satu Venäläinen, Elisa Rissanen, Johanna Lammintakanen, Erkki Heinonen, Anu Lehtinen, Janna Pöntinen, Henna Asikainen, Nina Katajavuori, Outi Linnaranta, Milla Räisänen, Samuli Salminen, Jari Lahti

TL;DR
This study tests a social identity intervention to reduce loneliness and improve mental health among university students, with preliminary results expected in 2026.
Contribution
The study introduces a novel social-identity group intervention (G4H) and compares it with active comparators in a quasi-experimental design.
Findings
Differences in background characteristics were observed between trial arms, indicating potential group selection bias.
The study is expected to provide insights into the effectiveness of social identity interventions for student well-being.
Primary outcomes include measures of loneliness and depression, with follow-ups planned for 1 and 3 months post-intervention.
Abstract
University students’ mental health problems are prevalent globally, which underlines the need for accessible and cost-effective mental health services in universities. Loneliness is a key risk factor for mental health problems, and it disproportionately affects students from minority backgrounds. Therefore, addressing loneliness and fostering inclusion and equality can be crucial strategies for enhancing students’ well-being. The aim of this study is to investigate a social-identity group intervention called Groups 4 Health (G4H) for university students’ well-being using both quantitative and qualitative methods. Here, we present the research protocol and report preliminary descriptive findings from the study cohort. The quantitative part of the study is a 4 parallel-arm nonrandomized controlled trial aiming to recruit 600 student participants from the University of Helsinki. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
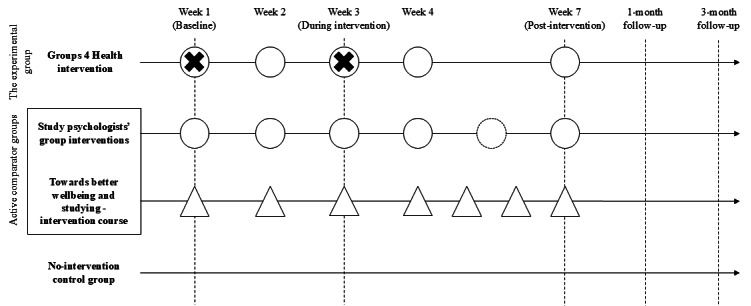 Figure 1
Figure 1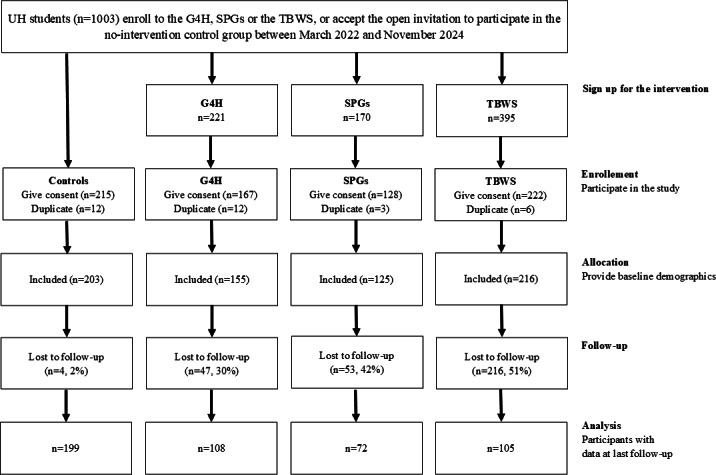 Figure 2
Figure 2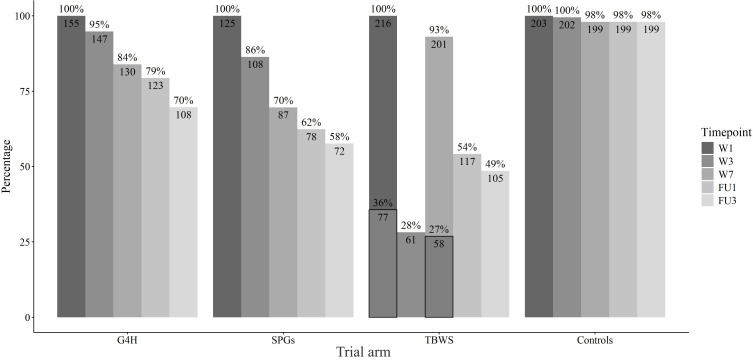 Figure 3
Figure 3| Assessment | Scales, forms, and measures | Time points and arms (1-4) | ||||||
|---|---|---|---|---|---|---|---|---|
| Week 1 | Week 2 | Week 3 | Week 4 | Week 7 | 1-month follow-up | 3-month follow-up | ||
| Primary outcome measures | ||||||||
| Loneliness | ULS-8 | 1‐4 | — | — | — | 1‐4 | 1‐4 | 1‐4 |
| Loneliness | ULS-4 | 1‐4 | — | 1‐4 | — | 1‐4 | 1‐4 | 1‐4 |
| Depression | PHQ-9 | 1‐4 | — | — | — | 1‐4 | 1‐4 | 1‐4 |
| Secondary outcome measures | ||||||||
| Active group memberships | EXITS | 1‐4 | — | 1‐4 | — | 1‐4 | 1‐4 | 1‐4 |
| Mental well-being | SWEMWBS | 1‐4 | — | — | — | 1‐4 | 1‐4 | 1‐4 |
| General well-being | GP-CORE | 1‐4 | — | — | — | 1‐4 | 1‐4 | 1‐4 |
| Anxiety | GAD-7 | 1‐4 | — | 1‐4 | 1‐4 | 1‐4 | ||
| Social anxiety | Mini-SPIN | 1‐4 | — | — | — | 1‐4 | 1‐4 | 1‐4 |
| Quality of life | EQ-5D-5L | 1‐4 | — | — | — | 1‐4 | — | 1‐4 |
| Use of social and health care services | Health service usage self-report (medications, health care appointments, hospitalization, and counseling) | 1‐4 | — | — | — | 1‐4 | — | 1‐4 |
| Time used by facilitators | Time used at planning, executing, and assessing the sessions | 1 | 1 | 1 | 1 | 1 | — | — |
| Study credits | UH | — | — | — | — | — | — | — |
| Grade point average | UH registries, 1 year before and 1 year after the intervention (arms 1‐4) | — | — | — | — | — | — | — |
| Weighted grade point average | UH registries, 1 year before and 1 year after the intervention (arms 1‐4) | — | — | — | — | — | — | — |
| Other outcome measures | ||||||||
| Identification with the intervention group | SISI | — | — | 1‐3 | — | — | — | — |
| Participants’ working alliance | WAI-SR | — | — | 1‐2 | — | — | — | — |
| Facilitators’ working alliance | WAI-SRT | — | — | 1 | — | — | — | — |
| Mood | Analog mood scale (0‐7) | 1‐4 | 1‐4 | 1‐4 | 1‐4 | 1‐4 | ||
| Fidelity to the G4H manual | G4H | 1 | 1 | 1 | 1 | 1 | — | — |
| Participant attendance | Number of sessions participated | 1 | 1 | 1 | 1 | 1 | — | — |
| Background variables | ||||||||
| Participant background | ||||||||
| Sociodemographic characteristics | Gender, birth date, mother tongue, marital status, household composition, residential situation, employment status, education, income, subjective financial situation, subjective health, subjective loneliness, and subjective minority status | 1-4 | — | — | — | — | — | — |
| Social support | SSQ3 | 1‐4 | — | — | — | — | — | — |
| Treatment motivation | SIMS | 1‐3 | — | — | — | — | — | — |
| Organized studying | 4 items from a HowULearn questionnaire [ | 1‐4 | — | — | — | — | — | — |
| Facilitators’ assessment | ||||||||
| Sociodemographic characteristics | Gender, birth date, mother tongue, marital status, household composition, residential situation, employment status, education, and income | — | — | — | — | — | — | — |
| Professional and individual characteristics | XS5 | 1 | — | — | — | — | — | — |
| Self-assessed skillfulness | TWIS | — | — | 1 | — | — | — | — |
| Characteristics | Trial arm | ||||
|---|---|---|---|---|---|
| G4H | SPGs | TBWS | Controls | ||
| Age, mean (SD; range) | 27.4 (8.0; 19-59) | 28.9 (7.1; 20-53) | 26.8 (7.0; 19-59) | 25.1 (6.6; 18-58) | <.001 |
| Missing, n | 1 | 0 | 0 | 1 | |
| Gender, n (%) | <.001 | ||||
| Woman | 110 (71) | 87 (70) | 172 (80) | 175 (86) | |
| Man | 35 (23) | 28 (22) | 42 (19) | 21 (10) | |
| Other | 9 (6) | 10 (8) | 2 (1) | 7 (3) | |
| Missing, n | 1 | 0 | 0 | 0 | |
| Relationship status, n (%) | .01 | ||||
| Single | 107 (69) | 78 (63) | 119 (56) | 130 (64) | |
| In a relationship | 41 (27) | 39 (31) | 92 (43) | 68 (33) | |
| Divorced or widowed | 6 (4) | 7 (6) | 3 (1) | 5 (2) | |
| Missing, n | 1 | 1 | 2 | 0 | |
| Living situation, n (%) | .05 | ||||
| Lives alone | 79 (51) | 57 (46) | 86 (40) | 95 (47) | |
| Lives with family | 52 (34) | 52 (42) | 105 (49) | 92 (46) | |
| Lives with others | 23 (15) | 16 (13) | 23 (11) | 15 (7) | |
| Missing, n | 1 | 0 | 2 | 1 | |
| Number of children, n (%) | .54 | ||||
| 0 | 98 (88) | 101 (89) | 175 (84) | 132 (88) | |
| ≥1 | 14 (13) | 12 (11) | 33 (16) | 18 (12) | |
| Missing, n | 43 | 12 | 8 | 53 | |
| Employment, n (%) | .08 | ||||
| Unemployed | 87 (57) | 58 (46) | 113 (53) | 90 (45) | |
| Employed | 66 (43) | 67 (54) | 99 (47) | 112 (55) | |
| Missing, n | 2 | 0 | 4 | 1 | |
| Gross income, n (%) | .07 | ||||
| <9 k €/year | 85 (56) | 57 (46) | 113 (55) | 125 (62) | |
| 9–‐18 k €/year | 40 (26) | 46 (37) | 51 (25) | 49 (24) | |
| >18 k €/year | 28 (18) | 21 (17) | 43 (21) | 29 (14) | |
| Missing, n | 2 | 1 | 9 | 0 | |
| Study years in current degree, mean (SD; range) | 1.9 (1.6; 0‐8) | 4.6 (3.7; 0‐23) | 1.6 (2.3; 0‐19) | 1.8 (1.8; 0‐10) | <.001 |
| Missing, n | 6 | 2 | 11 | 0 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychological Well-being and Life Satisfaction · Identity, Memory, and Therapy · Grit, Self-Efficacy, and Motivation
Introduction
Background
University students’ mental health problems are highly prevalent globally [1]. In Finland, 36% of university students reported high levels of psychological distress and 24% reported increased loneliness in the 2021 Finnish Student Health and Well-Being Survey [2]. Anxiety and depressive symptoms at the start of university studies are often persistent and related to poorer academic performance and lower engagement [3]. The need for accessible, cost-effective mental health services in universities is substantial [4].
Loneliness (the discrepancy between one’s actual and desired social relationships) has been recognized as one of the key risk factors for numerous adverse psychological and somatic health outcomes among students and youth [5] and in various population-based samples [67].
Having positive relationships and feeling socially connected is also essential for academic performance. Loneliness, social isolation, and low social status impact intellectual achievement [8], whereas engaging in the academic environment reinforces individuals’ learning activities [9].
Mental health problems are more prevalent among many minority groups, who experience psychological symptoms more often than the rest of the population [10-12]. Several studies have also found that belonging to more than one minority group increases the risk of stressful life situations, mental health problems, and thus the need to use mental health services [1314]. Belonging to minorities may also increase the risk of social isolation. According to the School Health Promotion study [12], young people belonging to gender and sexual minorities show elevated levels of loneliness, exclusion, and difficulties in receiving help in Finland. In addition, young people with immigrant backgrounds and young people with disabilities face considerable risks of loneliness [15]. These difficulties are largely caused by minority stress, which in turn has been linked with experiences of discrimination and unequal treatment [1216].
With this background, interventions targeting loneliness and supporting social connectedness, inclusion, and equality could be a significant way to approach the student mental health crisis. The Groups 4 Health (G4H) intervention studied in this protocol aims at improving well-being by supporting individuals’ social group memberships that are compatible with their social identity [17].
G4H builds on the social identity approach to health (SIAH) [1819] and the social identity model of identity change (SIMIC) [2021]. The SIAH [1819] comprises 2 related theories, the social identity theory [22] and self-categorization theory [23], claiming that individuals’ internalized group memberships have a significant role in their sense of self and that shared identities are important for productive social interaction. Therefore, belonging to multiple social groups that align with the individual’s identity is crucial for a sense of purpose and belonging, as well as for receiving support from others [18]. The role of group memberships is further emphasized during transitional life events such as moving to another country or entering a university, which may be stressful and may also affect an individual’s access to their social groups. The SIMIC further states that during stressful and transitional life situations, well-being can be enhanced by both managing and strengthening the individual’s social group memberships before the life change (the social identity continuity pathway) and by becoming a member of new social groups that align with the individual’s identity (the social identity gain pathway) [2021].
The fact that G4H addresses major life changes and social identities makes it particularly relevant in the university context. Many students experience major changes, such as relocating to a new country or city, integrating into new communities, and leaving familiar ones behind. For minority students, finding new social groups that align with their identity can be even more challenging, emphasizing their need for support.
This protocol provides a unique opportunity to study the G4H in the university context with a multimethod approach that integrates both quantitative and qualitative methods. By implementing this approach, we aim to capture not only the effectiveness of the G4H intervention and the participant- or facilitator-related factors that moderate the effectiveness, but also the perspectives of minority students participating in the intervention, which is an aspect that has been overlooked in previous research. The inclusion of qualitative methods is crucial, as it allows us to gain deeper insights into the experiences and potential challenges faced by these students, enriching our understanding of the intervention’s impact.
Additionally, neither the cost-effectiveness of the intervention nor its effectiveness on academic performance has been explored in previous studies. Both of these analyses are essential for assessing its suitability and adaptability in promoting student well-being. Furthermore, to our knowledge, the effectiveness of the G4H has been assessed only in Australia in studies organized by the developers of the intervention. These represent clear gaps in the existing literature that this protocol aims to address.
Aim and Objectives
The aim of this study is to investigate the effectiveness of the G4H intervention for university students’ well-being using both quantitative and qualitative methods. Our study includes 2 active comparators: intervention groups facilitated by the University of Helsinki (UH) study psychologists and an online intervention course focused on well-being and study skills. A control group of students who are not participating in any active well-being services at UH is also included.
Our first objective is to investigate the effectiveness and cost-effectiveness of the G4H intervention in (1) supporting well-being (most importantly by reducing loneliness and depression) and (2) supporting academic performance among university students. The second objective is to explore which factors moderate or mediate the effectiveness of the interventions. The third objective is to focus on the G4H intervention’s inclusiveness and the capacity of the G4H intervention to promote equality via qualitative methods.
Our research questions (RQs) are as follows:
RQ1: How effective is the G4H intervention in reducing loneliness and depression and in supporting university students’ well-being compared with the 2 active comparators and the control group? (objective 1)RQ2: Does the G4H intervention support academic performance compared with the active comparators and the control group? (objective 1)RQ3: Is G4H cost-effective compared with the 2 active comparators and the control group? (objective 1)RQ4: How do factors related to the participant, facilitator, or intervention fidelity mediate or moderate the effectiveness of the intervention? (objective 2)RQ5: What are the challenges and opportunities related to inclusion and equality in the G4H intervention? (objective 3)
Compared with the no-intervention control group, we hypothesize that all active interventions reduce students’ loneliness and depression (RQ1) and improve students’ academic performance (RQ2). However, participants in the G4H intervention will experience a more long-term reduction in loneliness than those in the other active intervention groups [24]. We hypothesize that treatment alliance [2526] and higher fidelity to the G4H manual mediate the interventions’ outcomes (RQ4). Regarding facilitators’ characteristics, we hypothesize that their greater self-rated skills and enjoyment in therapeutic work as well as agreeableness, openness, and engagement in personality traits and interpersonal relating will be positively associated with treatment alliances and intervention outcomes; and, conversely, greater difficulties and negative feelings in therapy work will be negatively associated with treatment alliances and outcomes [27-29]. Regarding motivation (RQ4), we set our hypotheses based on the self-determination theory [30] and the integral model of treatment motivation [31]. We hypothesize that autonomous motivation to participate in the intervention predicts greater engagement and increased effectiveness, whereas controlled motivation predicts lower engagement and effectiveness. We further hypothesize that engagement partially mediates the relationship between motivation and intervention effectiveness. No preliminary hypotheses are posed regarding RQs 3 and 5.
Methods
Trial Design
We conduct a parallel arm nonrandomized controlled trial with a 1:1 allocation ratio. We compare 3 intervention arms to a no-intervention control group as follows:
Arm 1: The experimental group, G4H.Arm 2: Active comparator group 1, the study psychologists’ group interventions (SPGs)Arm 3: Active comparator group 2, toward better well-being and studying intervention (TBWS).Arm 4: No-intervention control group.
The study design and timeline are presented in Figure 1. The study follows the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines.
Trial arms, intervention schedule, and points of assessment. The dashed vertical lines indicate points of assessment. A circle with a dashed outline indicates an optional meeting. △: online meeting; ○: live or online meeting; X: Groups 4 Health facilitators’ assessments.
Interventions
Overview
The interventions in each active trial arm represent courses provided by UH for students who are seeking help to improve their overall well-being and study skills. Additionally, a control group consisting of students receiving no intervention is included. Participation in the study and in the interventions is voluntary, and participants can withdraw from participating at any point without any negative consequences.
Arm 1: G4H (The Experimental Group)
G4H is a manualized group intervention that targets social group memberships with the aim of improving well-being [17], as discussed in the introduction.
The G4H intervention consists of five 90-minute sessions that aim to provide participants with the knowledge and skills they need to effectively manage their social group memberships and identities. Each of the 5 intervention sessions pertains to 1 module. Each module integrates exercises and discussions from the G4H workbook targeting various aspects of group dynamics as outlined in the SIAH and SIMIC frameworks. In brief, the first module “schooling” provides psychoeducation about the importance of social group memberships for health; the second module “scoping” supports the participants in exploring their social identities and networks; the third module “sourcing” aims at strengthening the social identities that are valued by the participant; the fourth module “scaffolding” supports making a social action plan to establish new valued group memberships; and finally, the fifth module “sustaining” aims at revisiting the intervention, discussing any potential difficulties, and encouraging the maintenance of group memberships [17]. A detailed description of the modules can be found in the G4H manual [32].
At the UH, the G4H group size can vary between 4 and 9 university students. The groups are mostly organized face-to-face, although some groups meet entirely remotely. The students earn 2 European Credit Transfer and Accumulation System (ECTS) credits for completing the G4H intervention.
G4H groups at the UH are facilitated by 2 psychology students carefully trained for the intervention and mentored by experienced clinical psychologists. Psychology students interested in facilitating the G4H intervention can sign up for G4H facilitator training. During the 2-month training course, facilitators are introduced to the intervention literature (approximately 15 h) and attend lectures on the background theory, structure, and content of the intervention (approximately 6 h). In the more practical part of the training, the facilitators practice how to deliver the intervention and gain first-hand experience of participating in the intervention by conducting the intervention with each other. Finally, after the practice meetings, each pair facilitates one 5-session G4H intervention for a group of UH students. Additional reflection meetings are held with a clinically experienced psychologist (J Lahti), where the facilitators share their experiences and any problems or questions they may have encountered. During the training, facilitators keep a learning diary, which supports further introspection and reflection. The student facilitators earn 2.5 ECTS credits for completing the intervention training.
The effectiveness of G4H has been studied earlier in Australia. In a nonrandomized controlled study, G4H (n=83) significantly improved well-being and social connectedness of young adults after the intervention and in 6-month follow-up relative to the control group (n=75). In a randomized controlled trial by Haslam and colleagues [33], G4H (n=66) decreased loneliness and social anxiety and increased group memberships significantly more than treatment as usual (n=54) [17]. In a randomized noninferiority trial by Cruwys and colleagues [24], G4H (n=84) was compared with cognitive behavioral therapy (CBT; n=90). Both interventions were equally effective in reducing loneliness by the end of the intervention period. However, the G4H group demonstrated a maintained reduction in loneliness during the follow-up. Both interventions significantly reduced depressive symptoms, with no significant differences between G4H and CBT [24]. In all 3 controlled studies on the effects of G4H, the inclusion criteria were low mood and loneliness.
Arm 2: SPGs (Active Comparator 1)
The UH study psychology team organizes group interventions for various challenges related to studying for bachelor’s and master’s students. The SPGs offer client-centered peer support facilitated mostly by 2 study psychologists (some individual sessions may have only 1 facilitator). The recurring themes in the SPGs include challenges with attention, independent studying, scientific writing, and support for re-entering the studies after a break. The structure of the different thematic groups is similar—short presentations, group discussions, practices, and homework. These groups are implemented mostly as face-to-face meetings; however, in some groups, part of the meetings are conducted face-to-face and part as remote meetings. One group typically lasts for a study period and comprises five to six 90‐105 minute sessions. The typical group size ranges from 10 to 12 students. The interventions have potential in supporting study skills and the challenges of initiating study tasks, identifying and normalizing unpleasant thoughts and emotions related to studying, and acknowledging the role of one’s individual situation and well-being in study planning. The study psychologists’ work is bound by the legal and ethical requirements for licensed psychologists in Finland, overseen by the National Supervisory Authority for Welfare and Health (Valvira).
Arm 3: TBWS (Active Comparator 2)
TBWS is an optional, 7-week online intervention course available for all UH students that aims to foster well-being and study skills. The course protocol has been described in detail earlier by Asikainen and Katajavuori [34]. The course is based on the principles of acceptance and commitment therapy [35] and aims to promote psychological flexibility. In addition, it aims to support study skills such as time management. The course takes place on an online learning platform (Moodle), and the students earn 3 ECTS credits for completing it. This course progresses weekly and has 6 central themes, including an introduction to the themes, individual work in practicing psychological flexibility and study skills, and weekly peer group discussions. The peer group work is an important part of the intervention and lasts throughout the course. In the peer groups, there are about 5 students in each group, and the groups remain the same throughout the course. Acceptance and commitment therapy–based interventions have been shown to support well-being among university students [36], and previous studies have suggested that this course can improve students’ well-being and studying in several ways [3738]. Thus, participating students have the potential to benefit from this intervention in terms of increased well-being.
Arm 4: The No-Intervention Control Group
The control group consists of students who are currently not taking part in any group interventions for study skills or psychological well-being at the UH. The participants in the control group may, however, take part in other social and mental health services than those provided by the UH, and this is not restricted during their participation in the study. The recruitment and data collection among the control group are scheduled to take place simultaneously with the active intervention groups: the participants are recruited at the same time, and they answer the questionnaires at the same pace as the active interventions progress during the academic year.
The interventions studied in this protocol have been developed for educational contexts and thus are expected to be well-suited for the university context. As discussed earlier, the G4H builds on SIAH and SIMIC, particularly aiming at supporting well-being during transitions in life, such as entering a university [21]. In addition, both the SPGs and the TBWS courses have been specifically developed by experts within the UH for supporting university students’ well-being and academic ability.
Participants
Setting and Timeline
The study is conducted in an academic setting among UH students in Finland. The recruitment has progressed as follows: for the RQ1-RQ3, the recruitment for the first data freeze ended at the end of 2024, and for RQ5, the recruitment ends by the end of the year 2025. For the more explorative objective 2 (RQ4) on the factors that mediate or moderate intervention effectiveness, we assume that a larger sample is required, and recruitment continues longer (current ethical approval allows data collection until the end of 2028). We completed the first data freeze in March 2025 for the RQ1 to RQ3 and will complete the data collection of the qualitative data for the RQ5 by December 2026.
The quantitative data collection started in March 2022 for the G4H and the SPGs. From October 2022, the data collection from all 3 interventions and the no-intervention control group has taken place simultaneously. The intervention schedule and points of assessment are illustrated in Figure 1. It should be noted that data on health care and social service use, as well as the participants’ minority status and readiness to attend the intervention, were gathered only from students who participated starting from March 2023 for the no-intervention control group and from September 2023 for the active intervention arms. The research ethics committee was informed about these added outcome measures, and a new ethical approval was obtained from the committee before data collection started.
In the collection of qualitative data, participant observation is conducted in the meetings of the G4H group and interviews with facilitators (n=9) and intervention participants (n=11) at the end of the intervention period. In addition, the follow-up interviews with intervention participants will be conducted 12 months after the first interview (2024‐2026). Additionally, focus groups with young people belonging to minorities (n=19 participants) are arranged to discuss G4H in terms of equality and inclusion during the data collection period (2023‐2025).
Sample Size
For RQ1-RQ3, the target minimum sample for the quantitative study is 600 participants, distributed evenly across 4 groups (150 participants per group). Since comparable previous studies with a similar group of participants using the same outcome measures are not available, it was not possible to make exact a priori sample size calculations. However, based on an estimation with the G*Power software (version 3.1) [39] on a repeated measures analysis of variance design with between-groups factors, this target sample size would yield at least 95% power for the detection of small effect sizes (f=0.20) as defined by Cohen [40] when considering multiple comparisons and a 35% attrition rate. Previous studies with different designs investigating the G4H intervention have demonstrated significant treatment effects with smaller samples ranging from 66 [33] to 84 [24] participants in the G4H group, supporting the expectation that our larger sample will be sufficient to detect meaningful treatment effects, or lack thereof.
Recruitment
The UH student well-being services are available to all students at the university, and there are no exclusion criteria for the study. All the students willing to participate are included regardless of their level of loneliness, state of psychological well-being, or stage of studies. Students are recruited for the active intervention groups and no-intervention group by email, website, and social media advertisements circulated by the UH media and communications services, communications services at the faculties, student health services, and student organizations. The students are not randomly assigned to the intervention groups and can sign up for a course of their choice. The facilitators of the G4H intervention are also invited to participate in the study during the G4H facilitator training. All facilitators willing to participate are included in the study. Taking part in relevant concomitant care is not prohibited during the intervention study. The participating students or facilitators are not blinded to the study protocol.
Quantitative Methods
To collect the quantitative data, we use paper-and-pencil and electronic versions of the questionnaires. Those in the active intervention groups fill out the questionnaires before or after the intervention sessions if the questionnaires are provided electronically and during the session if the questionnaires are provided on paper. Those in the no-intervention group fill out the questionnaires based on the email reminders of the electronic data collection system (time interval between reminders is the same as the interval between sessions in the active intervention groups).
Electronic data collection is implemented in the Research Electronic Data Capture (REDCap) system (Vanderbilt University) [41], provided by the UH for collecting sensitive research data electronically. In the case of the TBWS intervention, data collection from time points before and immediately after the intervention is partly integrated into the online course platform, and the students can respond either via the course platform or via the REDCap system, while data collection from week 3 and the 1- and 3-month follow-ups is implemented only in the REDCap.
Before the analysis phase, the data validity is confirmed via range checks, missing value checks, and outlier detection. Potentially erroneous data are checked against the paper and electronic forms, and other necessary sources, and corrected if needed. All modifications are documented.
Participant retention is promoted by reminding the participants during the group meetings to fill out the questionnaires. All participants receive up to 5 reminder messages from the electronic data collection system if they do not complete the necessary questionnaires on time. Retention is also promoted by the possibility of receiving written feedback on the questionnaire results after participation. Participating students also receive movie tickets as compensation for completing all follow-up questionnaires. Adherence to the G4H intervention is monitored by documenting the number of sessions in which each student participated.
All the quantitative methods used are presented in Table 1, which also includes the measurement time points and study arms from which the data are collected. Multimedia Appendix 1 includes a table that describes the unabbreviated titles of each scale, scale details, and information on their reliability and validity. Most measures have demonstrated at least acceptable internal consistency (Cronbach α≥0.70) and convergent validity with other similar measures. The few exceptions with lower Cronbach α are either very short scales (4 items) or include a specific subscale that performs poorly.
Primary Outcomes
The primary outcomes are loneliness and depression (refer to Table 1 and Multimedia Appendix 1 for details). Based on previous evidence, the G4H intervention has at least equal potential to promote well-being in these areas as CBT [24].
Secondary Outcomes
The secondary outcomes are active group memberships, mental well-being, general well-being, anxiety, social anxiety, academic performance, health-related quality of life, use of social and health care services, intervention costs, and cost-effectiveness of the intervention (refer to Table 1 and Multimedia Appendix 1 for details).
To assess participants’ academic performance, data will be retrieved from the UH student register (Sisu student information system). Academic performance is determined by 3 outcome variables: overall accumulated study credits, the grade point average (GPA) of the study credits and the weighted GPA. When determining the weighted GPA, only completed studies that have been assessed on a numeric scale (from 1 to 5) are considered, as some courses accumulate study credits but are graded only as passed or failed. Weighted GPA is determined by the grades of each course weighted by the number of credits gained for it. The academic performance data are collected from 2 time periods: a 1-year period before and a 1-year period after starting the assigned intervention (baseline, week 1).
Cost-effectiveness analyses will apply a societal perspective by including intervention costs as well as university students’ health and social services costs. For the cost-effectiveness analyses, the facilitators will provide information on the time used for planning, executing, and assessing the sessions to evaluate the costs of the G4H intervention. Furthermore, the students in all trial arms fill out 2 questionnaires before the intervention, immediately after the intervention, and at 3-month follow-up (Table 1). The questionnaires measure health-related quality of life and self-reported use of health and social services (Table 1). The use of health and social services will be monetarized using Finnish national unit costs [62].
Other Outcomes
Other outcome measures include the participant’s identification with the intervention group, attendance, and mood, as well as facilitators’ fidelity to the intervention manual, and both the participant’s and facilitator’s evaluations of the working alliance (Table 1 and Multimedia Appendix 1). These measures are used to examine their potential in moderating or mediating the effectiveness of the intervention. Fidelity to the intervention manual is measured with a questionnaire detailing how well the facilitators covered the core themes of each intervention session. Each facilitator pair fills in the questionnaire immediately after each intervention session. This questionnaire is the same as used by the previous study that assessed program adherence to the G4H [33] .
Background Variables
In addition to the outcome measures described above, survey data on the participants’ background are gathered to account for them in the analyses and to examine their potential in moderating or mediating the effectiveness of the intervention (Table 1 and Multimedia Appendix 1). The participant background questionnaire includes questions on sociodemographic characteristics (refer to Table 1 for details), experienced social support, organized studying, and situational intrinsic and extrinsic motivation. Readiness to attend the intervention is enquired by a set of readiness rulers adapted from Miller and Rollnick [56]. Furthermore, data are gathered from the UH registries, including information on study rights (faculty, degree programs, and fields of study) and their starting years, active and passive registration, and completed degrees.
Facilitators’ Characteristics
To investigate how facilitators’ individual professional and personal characteristics may predict the intervention process and effectiveness, G4H facilitators complete self-report measures both before and during the interventions (Table 1 and Multimedia Appendix 1). Before initiating the intervention, facilitators complete questionnaires related to personality traits, attachment style, and self-experiences in close personal relationships. After the third session, the facilitators report experiences of their current skillfulness, difficulties, and emotions in group work.
Statistical Analyses
We will conduct our analysis following the intention-to-treat principle, including all participants regardless of whether they completed the intervention.
The change in the outcome variables over time will be analyzed with linear mixed-model analyses due to the hierarchical data structure. Information criteria are used to assess model fit and determine the appropriate model structure. Mixed effects models can also be fitted for participants with missing data from one or more time points. If needed, other appropriate imputation methods, such as multivariate imputation by chained equations [63], will be used. For this reason, the number of participants included in the analyses is likely to be higher than the number of participants providing data at the last follow-up.
We will explore with logistic regression analyses whether background characteristics and baseline psychiatric symptoms predict study dropout, and necessary means to account for any systematically missing data will be taken. We aim to show that the missing observations of the outcome variable, due to dropout, are conditionally independent from the observed values of the outcome variable given our model for dropping out from the study. If needed, inverse propensity score weighting is carried out so that the treatment effects are conditionally independent from the treatment group assignments and from differing dropout rates given the propensity scores. We consider individuals’ selection into different study groups (arms) under the stable unit treatment value assumption based on their background characteristics, given that we have access to an extensive dataset. The selection of individuals into groups is accounted for by making the estimators double robust, which is a well-known approach to adjust for selection into groups based on background characteristics in model-based estimates [6465]. This ensures that our results are unbiased and consistent estimators of the treatment effects. Potential effects of the COVID-19 pandemic on the stability and change in students’ well-being will be inspected and considered in the analyses if necessary.
All models will be inspected for normality of residuals, homoscedasticity, and multicollinearity. The outcome variables will be transformed to attain normality if needed. Appropriate interaction terms are added for further subgroup analyses. Potential mediator (eg, therapeutic alliance, motivation, and model fidelity) and moderator (eg, participant and facilitators' background) effects will be inspected in additional mediation and moderation analyses.
In the case of missing questionnaire items, within-person imputation is carried out for responses when less than 50% of the answers are missing per scale (the within-person average of the existing items is imputed to the missing responses). We acknowledge that this procedure may decrease the within-person variation in the data. However, as we discuss later, the prevalence of item nonresponse in the dataset is low.
We will take appropriate measures to balance between Type I and Type II error in the reporting of analyses results. If needed, we will use methods to account for multiple testing such as false discovery rate or new eigenvalue-based methods that provide a more accurate adjustment for nonindependence among tests [66].
Cost-Effectiveness
We will conduct 3-month follow-up cost-utility and cost-effectiveness analyses. The cost-utility analysis will use EQ-5D-5L–based quality-adjusted life-years as the effectiveness outcome measure [5067]. The cost-effectiveness analysis will use both primary outcomes of the effectiveness study, namely loneliness measured with the 8-item University of California Los Angeles Loneliness Scale [42] and depression measured with the Patient Health Questionnaire [44] (Table 1 and Multimedia Appendix 1) as the effectiveness outcome measure. The analyses will use a societal perspective by including the intervention costs and costs of students’ health and social service use. The analyses will be conducted with the intention-to-treat principle. The missing outcome measures will be imputed with multiple imputation methods [68]. We will estimate incremental net health benefits between interventions. The estimation of the incremental net health benefits and 95% CIs will be used for statistical methods (eg, ordinary least squares regressions) [69]. We will perform multiple 1-way sensitivity analyses to test the robustness of the economic evaluation results. The results of sensitivity analyses will be presented in a tornado diagram. If interventions show effectiveness, we will conduct decision-analytical modeling of long-term cost-utility and cost-effectiveness beyond 3-month follow-up data.
Qualitative Methods
We explore inclusion and equality, with respect to G4H using three qualitative data collection methods: (1) participant observation, (2) interviews with G4H participants and facilitators, and (3) focus groups with young people who belong to minorities. The aim is to examine challenges and possibilities in the G4H intervention regarding social inclusion and equality and whether G4H promotes long-term social inclusion and equality among the participants. The focus groups target young people belonging to sexual and gender minorities, young people with immigrant backgrounds, and young people with disabilities. These groups represent youth minorities with a considerable risk of loneliness [15]. To date, research on their experiences with different services is lacking [1270-72undefinedundefined]. These groups are also underrepresented in higher education [27374].
The participant observation focuses on the interaction and the practices undertaken in the groups to gain knowledge about how the groups work, what kinds of issues they deal with, and especially how inclusion and equality are accomplished in the groups (are there minority participants, can participants influence the themes dealt with in the groups, or is inclusion and equality taken into account in some other ways in the groups). Following the ethnographic research tradition, the researcher takes part in the activities of the groups instead of observing them from the outside. Depending on their preferences, the study participants (both facilitators and participants in the groups) will be interviewed in a group, in pairs, or individually, in facilities located outside the university (eg, in a study room of a local library).
In the focus groups, young people belonging to minorities are asked to comment on the design or description of G4H in terms of equality and inclusion, with the goal of enhancing inclusivity by listening to their views on the interventions and accumulating knowledge on the fit between the interventions and their specific needs. All the interviews will be tape-recorded and transcribed for analysis.
To ensure the validity of qualitative findings, data triangulation is used via collecting 3 different types of data: focus group interviews, intervention participant interviews, and facilitator interviews. Setting these different data into a dialogue enables a multifaceted understanding of intervention effectiveness, inclusion, and equity. The analyses of qualitative data draw on minority stress theory [75] and intersectional theory [7677].
The analyses are conducted by following reflexive thematic analysis [7879]. Reflexive thematic analysis is conducted by following 6 steps that move from familiarization with data, coding, formulating, and refining themes to writing the report in alignment with the key principles of the approach, highlighting reflexivity and in-depth attention to nuance in participants’ meaning-making. If several analysts are involved in the analysis, the goal is to engage in discussion throughout each step of the analysis, to refine the analysis with the help of various analysts’ viewpoints. This approach, therefore, acknowledges that analysts’ interpretations of the data may differ, which is why transparency and a close consideration of the subjectivity of interpretation are highlighted. The first steps of the analysis may be conducted with the help of software (such as ATLAS.ti 24; Lumivero), but the actual analysis requires repeated rounds of reading of the whole dataset by the analysts. The emphasis on researcher reflexivity in this analytical approach further enhances the validity of interpretations and helps ensure that the findings reflect the multiplicity of participants’ viewpoints and accurately portray repetitive patterns in the data.
Ethical Considerations
Overview
The study protocol was approved by the Research Ethics Committee in the Humanities and Social and Behavioural Sciences at the UH, Finland (Statements: 15/2022, 32/2023, 10/2025). The ethical board will be informed in case of important protocol modifications. Written informed consent to participate in the study is obtained from all participants and facilitators. The participants are informed about the study via an information sheet and a data protection notice detailing the research protocol, data management, and participants’ rights following the General Data Protection Regulation (GDPR) of the European Union. The consent form can be signed electronically or on paper. Electronic consent forms are delivered via an email from the REDCap system before the first intervention session or at a corresponding time point for the control group. Paper consent forms are delivered during the first meeting of each active intervention. The participants are also told that they may be contacted about potential ancillary studies. The participants are informed that they can withdraw from the study at any point without any consequences. The participants receive movie tickets as compensation for participating. A data monitoring committee has not been appointed as there is no suspicion of harm caused by the interventions studied in this trial to the participants.
Privacy and Confidentiality
The access to the data collection systems is restricted to assigned data managers. The questionnaire data collected on paper are transferred to REDCap by a data manager. Paper data are stored in a secure locked facility with restricted access provided by the Faculty of Medicine at the UH. All the data are downloaded from the data collection system and backed up on secure UH servers with restricted and password-protected access. Upon download, the data are pseudonymized via ID codes, and data that include personal identifiers are stored separately. All identifiers enabling linkage to the university records are removed from the data during the pseudonymization process. No such data that could risk reidentification of the participants is shared outside the research group.
The participants’ identifiers are not shared outside the research group at the UH. Other pseudonymized research data may be shared with selected research partners for further research. A research collaboration agreement and a data sharing and processing agreement, which specifies the secure management and use of the data, will be made.
The consent form including identifiers will be destroyed 10 years after the end of the research project. Pseudonymized data will be kept for later, compatible scientific research in accordance with the requirements of the GDPR. The data will be stored at a secure UH server and kept protected so that only those who need the data can access them. Before the data can be used for later, compatible scientific research, the controller will ensure that the new use of data is compatible with the initial purpose in accordance with the requirements of the GDPR. Participants will receive a new data protection notice on the new use of the research data, unless the controller can no longer identify the participants from the data.
Participants’ safety
We will do everything we can to ensure the safety of the participants. We do recognize that some topics discussed during the sessions, such as challenging group memberships and difficulties related to academic stress, may cause distress (by activating existing anxieties). The group sessions are designed to create a supportive environment where students feel secure and comfortable to express concerns to the facilitators. Each intervention has clear protocols on providing further support to the students if needed, and the training of the facilitators or course organizers includes plans to mitigate risks to the safety of the participants. Moreover, anonymous feedback is collected after all the interventions to tackle potential issues for the subsequent courses.
In the G4H course, potential challenges are addressed during the facilitator training and the mentoring sessions. Facilitators are instructed to consult with the course supervisor, J. Lahti, a clinical psychologist and licensed trainer-level psychotherapist, if they have any concerns about a participant’s well-being. Additionally, they are provided with resources for further support, including contacts within the university’s counseling services and public health care, which can be shared with participants if needed.
In the TBWS course, students are also provided resources for further support, including contacts within the university’s counseling services and public health care. After assessing their well-being in the beginning of the course, all students get feedback and are instructed to seek this additional support if they get worried about their well-being. In addition, students get detailed instructions for peer group discussions instructing them to focus on the course themes and how the learned aspects can support their studying rather than discussing their personal health issues. Students are also requested to contact course teachers if they become concerned about their own or a peer’s well-being.
In the SPGs, psychological safety is promoted by discussing the group’s rules during the initial meeting. Students have the option to anonymously inform the facilitators, via a note, about any specific concerns or needs they would like the facilitators to be aware of. Study psychologists guide group discussions and intervene in potential challenging situations. If concerns arise, the psychologist offers discussion support to the student. Additionally, students have the opportunity for individual guidance from the study psychologist, who can assist them in contacting health care services if necessary. Students are encouraged to provide anonymous feedback to identify any potential weaknesses of the intervention.
We are aware that the young people invited to participate in the study about inclusion and equality might be in vulnerable positions. Our research team has extensive experience in conducting qualitative interviews with young people in vulnerable positions or who belong to minorities, such as LGBTIQ+ young people (lesbian, gay, bisexual, transgender, intersex, queer, and other), young people with diverse ethnic backgrounds, and young people not in employment, education, or training. The interviewers aim at sensitivity in their interaction with the interviewees and, for instance, provide the interviewees with room for regulating the depth and detail in which they discuss their experiences and emotions. The interviews and focus groups have been carefully designed to avoid placing excessive mental strain on participants. Participants are free to decide for themselves how much detail they wish to share about their own experiences and what they wish to reveal about their minority identities and related experiences. In addition, the use of peer facilitators in the focus groups promotes a sense of security and confidentiality, as well as peer support.
The opportunity to talk about one’s experiences with the G4H intervention and the opportunity to be respectfully heard can be empowering for the interviewed young people. In addition, sharing one’s thoughts and experiences of observed practices can alleviate stress and provide a sense of social support. On the other hand, talking about potential negative aspects, or remembering and describing possible experiences and observations of discrimination, or talking about experiencing limitations related to gender identity, sexual orientation, ethnicity, or ability can cause minor, short-term discomfort. However, according to our evaluation, this is highly unlikely to exceed the discomfort caused by the challenges and small annoyances of normal everyday life. The participants will be offered an opportunity to talk about the feelings caused by the interview afterwards with the interviewer or the researcher responsible for the entire research project. They will also be provided with contact information for services that provide support for young people, and if necessary, the interviewer will help them find relevant services in their hometown. If the young person wishes to, they will be given a chance to read the transcript of the interview, that is, the transcribed text of the audio recording.
Results
Study Status
Figure 2 illustrates the number of participants from the start of the study in March 2022 until the first data freeze in March 2025.
Study recruitment flow chart. Duplicate participants had already participated in the study (either in the same trial arm or in another arm). Controls: no-intervention control group; G4H: Groups 4 Health; SPG: study psychologists’ group interventions; TBWS: toward better well-being and studying intervention; UH: University of Helsinki.
A high proportion of the university students enrolled in the interventions decided to participate in the study. The minimum target sample size (n=150) was attained for the G4H (n=155), TBWS (n=216), and control group (n=203). For the SPGs, the target sample size was not attained (n=125).
The anticipated study completion date for all data collection is by the end of the year 2028. Analyses for RQ1 and RQ3 are anticipated to take place in years 2025 and 2026, analyses for RQ2 in years 2026 to 2027, and analyses for RQ4 and RQ5 in years 2026 to 2028. First results from the study are anticipated to be published in the year 2026.
Attrition
Figure 3 illustrates the attrition rates by trial arms by the first data freeze in March 2025. The percentages do not accurately indicate the number of study dropouts, as all surveys are sent to participants regardless of nonresponse to previous surveys, allowing them to re-enter the study. The attrition rate has exceeded the anticipated 35% in the SPGs and TBWS. For the TBWS, the bars with black outlines represent the responses to the REDCap survey. The low response rate at the week 3 assessment (during intervention) is due to the survey only being available in REDCap and not integrated into the online course platform as in week 1 and week 7. Based on the attrition rate, we took action to increase retention, including adding incentives for the participants (a movie ticket for completing the surveys).
Attrition rates by trial arms. For TBWS, the smaller percentages at W1 and W7 denote the percentage of answers collected via REDCap. FU1: 1-month follow-up; FU3: 3-month follow-up; G4H: Groups 4 Health, SPG: Study psychologists’ group intervention; TBWS: toward better well-being and studying intervention, Controls: no-intervention control group, UH: University of Helsinki; W1: week 1; W3: week 3; W7: week 7.
Participant Descriptive Statistics
Table 2 illustrates the participants’ characteristics of the current sample at baseline by trial arm. In all groups, most participants are women (87/125, 70%‐175/203, 86%), not in a relationship (119/214, 56%‐107/154, 69%), and childless (175/208, 84%‐101/113, 89%). The age medians are lower than the age means (median_G4H_ 25, IQR 22-29 y, median_SPGs_ 27, IQR 25-31 y, median_TBWS_ 24, IQR 22-31 y, and median_Control_ 23 y, IQR 21-27 y).
To determine whether the participants in the trial arms differed from one another in terms of background characteristics, we performed chi-square tests for categorical variables and Kruskal-Wallis tests for continuous variables (based on visual inspection, neither followed a normal distribution) (Table 2). Trial arms differed in age (Kruskal-Wallis χ^2^3=40.7, P<.001), gender (χ^2^6=5.4, P<.001), relationship status (χ^2^6=15.8, P=.02), living situation (χ^2^6=12.6, P=.05), and study years in current degree (Kruskal-Wallis χ^2^3=125.7, P<.001). These observations highlight the need to address group selection bias.
Missing Values Analyses
Item nonresponse (ie, a participant does not respond to an item within a questionnaire) was observed with missing data pattern plots across all groups. First, we examined the outcome variables which are assessed at all time points except week 3: loneliness, depression, mental well-being, general well-being, anxiety, social anxiety, multiple group memberships, and mood. Structural missingness (not all questionnaires were administered to all TBWS participants) was not included. Across all time points (excluding week 3), 94% (2174/2317) of survey responses were complete, 5% (105/2317) included a single missing item, and 2% (38/2317) included multiple missing items. Regarding the shorter survey taken at week 3 that includes the assessment of group memberships, mood, identification with the intervention group, loneliness, and working alliance, 96% (499/518) of responses were complete, 3% (16/518) included a single missing item, and 1% (3/518) included multiple missing items (0‐7 missing items per survey). The level of missingness within given survey responses appears acceptable, especially when considering the length of the longer surveys (55 items, approximately 15‐23 min).
Missingness was more prevalent for the selected background variables (Table 2). Of all survey responses of these selected variables, 79% (581/732) of responses were complete, 19% (141/732) included a single missing item, and 1% (10/732) included multiple missing items. Most often, participants left their number of children unreported. This may be due to a misunderstanding where some childless participants skipped this question instead of reporting zero. However, as the overall missingness in the selected background variables is 3% (172/5856), it is still within acceptable limits (<5%).
Discussion
Overview
Psychological ill-being and loneliness are highly prevalent among university students, often leading to long-lasting negative effects on mental health, social connectedness, and academic performance. To address this growing issue, accessible and preventive services at universities are needed. We investigate the effectiveness of the G4H intervention for university students’ well-being using both quantitative and qualitative methods including 2 active comparators.
Principal Findings
We hypothesize that all the active interventions will improve students’ well-being and that the decrease in loneliness will be more pronounced for the participants of the G4H group, in line with earlier studies [17243337]. We also anticipate valuable qualitative insights into the experiences of minority students. The multimethod approach will provide a comprehensive understanding of the intervention’s effectiveness and the contextual factors influencing its impact.
Strengths and Limitations
A key strength of this study is its multifaceted approach, which allows for a comprehensive exploration of existing student well-being interventions at the UH. By involving multiple collaborators, each with unique research interests and expertise, the study can address a wide range of critical questions related to the interventions’ impact. This collaborative framework enables the examination of various mediators and moderators, as well as the integration of both qualitative and quantitative methods. This perspective not only enriches the understanding of students’ well-being but also ensures that these phenomena are not oversimplified. The multimethod design of the study allows participants to express their thoughts and experiences in more depth, enhancing participant engagement and potentially leading to richer data.
Furthermore, the qualitative insights gained from this approach will provide a better understanding of the intervention’s effectiveness—or lack thereof—from the perspective of minority students. This insight is crucial for further developing the G4H intervention in terms of inclusion and equality. Moreover, the study is particularly relevant from an implementation point of view, as it will ensure the suitability and effectiveness of the method in Finland, addressing the significant need for early-stage support within the service system.
This study also has some limitations. The comparator arms (SPGs and TBWS) differ from the G4H slightly in terms of intensity (G4H: 5 sessions, TBWS: 6 sessions, and SPGs: 5‐7 sessions) and delivery methods. This variability complicates direct comparisons between these groups and the G4H intervention, potentially introducing confounding factors that could influence the study’s outcomes. Additionally, the varying data collection methods may introduce mode effects or measurement bias, as well as structural missingness, impacting the reliability and comparability of the data. To mitigate these concerns, we will conduct sensitivity analyses and discuss the implications of these methodological differences in our results.
Furthermore, the lack of exclusion criteria and the nonrandomized design of the protocol may introduce potential biases regarding group composition. However, allowing students to choose which intervention they participate in respects their autonomy and aligns with ethical research practices. This nonrandomized design increases the ecological validity of our findings by capturing the experiences of students in a real-world educational environment, which is important for making informed decisions that can improve services at both individual and population levels [80]. Ecological validity was further increased by including all students in the interventions and in the study. We will implement strategies to address potential selection bias, including collecting detailed demographic and baseline data and using inverse propensity score weighting using double robust estimators, if necessary.
Due to the absence of comparable previous research with the same study population, a priori sample size calculations were not conducted. This represents a limitation, as underpowered samples may fail to detect treatment effects, while overpowered samples may lead to unnecessary use of resources. Nonetheless, the existing literature indicates that significant treatment effects can be observed with smaller sample sizes in different populations [1724]. Given the complexity of our analysis plan, which includes mixed model analyses and potential (double robust) inverse propensity score weighting, we believe it was justified to aim for a larger target sample size in this study.
We did not appoint an independent data monitoring committee, as this is a naturalistic trial without randomization, and it investigates interventions that focus on psychosocial well-being rather than alleviating psychiatric pathologies. Moreover, there were no clinical inclusion criteria, and as the participants were university students, most showed rather low levels of psychological distress. Therefore, we anticipated minimal risk of harm from the interventions, a decision that was also accepted by the ethical review board of the study. However, we recognize that the presence of such a committee could have enhanced the integrity and trustworthiness of the data collection process.
The study protocol was registered retrospectively. This lack of prospective registration may affect the perceived transparency and credibility of the work. However, in this protocol paper, we have aimed to enhance transparency by providing a comprehensive and detailed description of the study design and methodology before analyzing and publishing the results.
Future Directions
These results can be expected to be generalizable across Finnish higher education, but caution is needed when extending the results beyond the higher education context or to institutions in other countries. Future studies should investigate the implementation and effectiveness of these interventions in different contexts, including other educational institutions in Finland and internationally, to enhance the understanding of their applicability and impact.
Dissemination
The trial results will be published in peer-reviewed scientific journals and scientific conferences. We follow the authorship eligibility guidelines of the International Committee of Medical Journal Editors [81]. We do not intend to use professional writers.
Conclusions
If proven effective, the interventions outlined in this protocol could be implemented in universities nationwide and have a significant impact in improving university students’ well-being in both the short and long term, fostering positive mental health and supporting academic success and future career paths. These models may also be applicable in other settings, such as basic and secondary education, and in workplace environments. Ultimately, this research aims to support inclusion and equality in youth well-being services.
Supplementary material
10.2196/79319Multimedia Appendix 1Details of all questionnaires and scales used in the study, including information on number of items, subscales, scoring, reliability, and validity.
10.2196/79319Checklist 1SPIRIT checklist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sheldon E Simmonds-Buckley M Bone C et al Prevalence and risk factors for mental health problems in university undergraduate students: a systematic review with meta-analysis J Affect Disord 05152021287282292 doi 10.1016/j.jad.2021.03.054Medline 33812241 · doi ↗ · pubmed ↗
- 2Parikka S Holm N Koskela T Ikonen J Kilpeläinen H Health and well-being survey of higher education students 2021: research implementation and methods [Article in Finnish]National Institute for Health and Welfare THL 2022 UR Lhttps://www.julkari.fi/server/api/core/bitstreams/1086 b 6c 3-2eab-4b 20-a 020-22942305 f 9c 2/content Accessed 31-12-2025
- 3Duffy A Keown-Stoneman C Goodday S et al Predictors of mental health and academic outcomes in first-year university students: identifying prevention and early-intervention targets BJ Psych Open 058202063 e 46doi 10.1192/bjo.2020.24Medline 32381150 PMC 7331085 · doi ↗ · pubmed ↗
- 4Auerbach RP Mortier P Bruffaerts R et al WHO World Mental Health Surveys International College Student Project: prevalence and distribution of mental disorders J Abnorm Psychol Oct 20181277623638 doi 10.1037/abn 0000362 Medline 30211576 PMC 6193834 · doi ↗ · pubmed ↗
- 5Goosby BJ Bellatorre A Walsemann KM Cheadle JE Adolescent loneliness and health in early adulthood Sociol Inq Nov 12013834505536 doi 10.1111/soin.12018 Medline 24187387 PMC 3810978 · doi ↗ · pubmed ↗
- 6Hawkley LC Cacioppo JT Loneliness matters: a theoretical and empirical review of consequences and mechanisms Ann Behav Med Oct 2010402218227 doi 10.1007/s 12160-010-9210-8Medline 20652462 PMC 3874845 · doi ↗ · pubmed ↗
- 7Holt-Lunstad J Smith TB Layton JB Social relationships and mortality risk: a meta-analytic review P Lo S Med 0727201077 e 1000316 doi 10.1371/journal.pmed.1000316 Medline 20668659 PMC 2910600 · doi ↗ · pubmed ↗
- 8Walton GM Cohen GL A brief social-belonging intervention improves academic and health outcomes of minority students Science Mar 182011331602314471451 doi 10.1126/science.1198364 Medline 21415354 · doi ↗ · pubmed ↗