EUS–guided fine-needle aspiration for the diagnosis of hepatic metastatic neuroendocrine tumor (with videos)
Sashuang Wang, Yating Wang, Dongqiang Zhao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
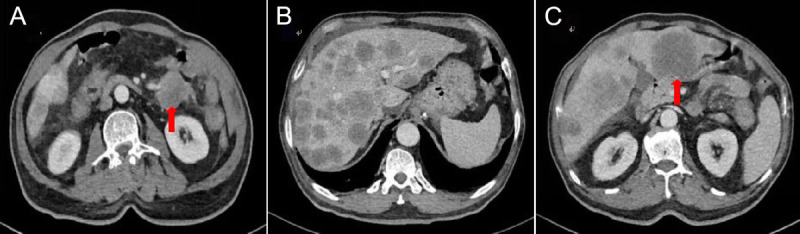 Figure 1
Figure 1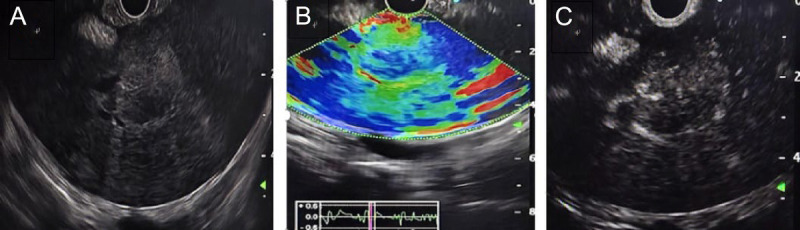 Figure 2
Figure 2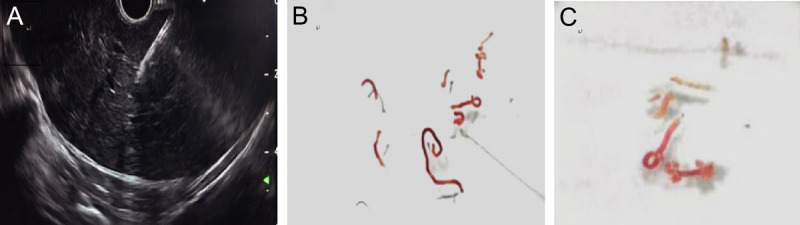 Figure 3
Figure 3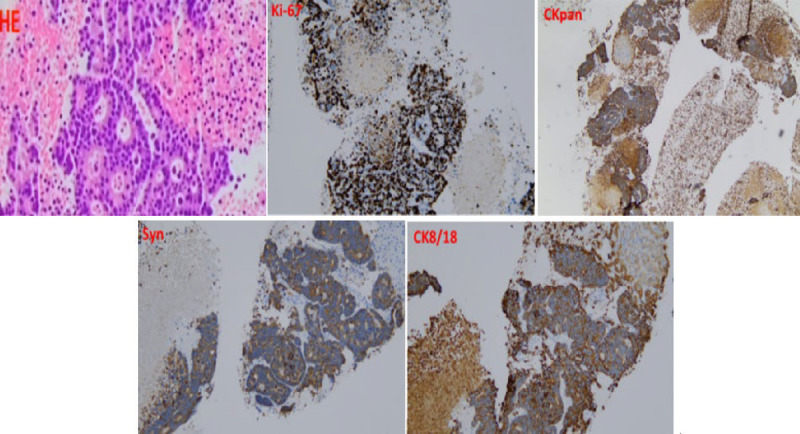 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Gastrointestinal Tumor Research and Treatment · Metastasis and carcinoma case studies
A 75-year-old male presented with postprandial bloating, nausea, vomiting, and reduced bowel movements. Contrast-enhanced abdominal computed tomography (CT) revealed diffuse heterogeneous small intestinal wall thickening with luminal narrowing in the left abdomen, along with multiple hepatic hypodense lesions, suggestive of small intestinal neoplasm with liver metastases [Figure 1]. Tumor marker tests showed CA-125 40.99 U/mL and CA-199 52.43 U/mL. To establish a definitive diagnosis, endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) was performed.^[1]^ EUS demonstrated a 2.0 × 2.0-cm hypoechoic lesion in the left hepatic lobe, characterized by hyperechoic margins and homogeneous internal echoes [Figure 2A]. Elastography demonstrated blue-green coloration [Figure 2B]. Contrast-enhanced EUS using 3 mL intravenous sulfur hexafluoride microbubbles revealed progressive enhancement starting 10 seconds post-injection, with an additional 1.0 × 0.8-cm enhancing lesion detected distally [Figure 2C, Video 1]. EUS-FNA was performed via transgastric approach using a 19G needle (COOK EchoTip Ultra), with two passes (10 actuations per pass) yielding tissue and cellular material [Figure 3, Video 2]. No postprocedural complications occurred. Histopathology (HE staining) confirmed malignant cells. Immunohistochemistry showed positivity for CK8/18, CKpan, and Syn, with a Ki-67 index of 70% [Figure 4]. A diagnosis of grade 3 neuroendocrine tumor (NET G3) was established. Given the high proliferative activity of G3 NET and evidence of metastatic disease, the patient was referred for systemic oncologic treatment.
Small intestinal neuroendocrine tumors (SI-NETs), classified as malignant neoplasms arising from enterochromaffin cells, predominantly occur in the ileum and less frequently in the jejunum. Recent epidemiological data indicate a global rise in the incidence of these tumors. Due to the small bowel’s deep anatomical location and nonspecific early symptoms, many patients are diagnosed with distant metastases at presentation, with the liver being the most common metastatic site.^[2]^ Although EUS-FNA is a well-established technique for sampling hepatic lesions,^[3]^ its application in diagnosing liver metastases from small intestinal neuroendocrine tumors (NETs) has not been previously described. This case report documents the first use of EUS-FNA to confirm small intestinal NET hepatic metastasis, marking a significant contribution to the precise diagnosis and treatment of small intestinal neuroendocrine tumor liver metastases.
Supplementary Videos
Video 1: Multimodal EUS (elastography and contrast-enhanced imaging) delineates the location, structural features, stiffness profile, and vascular dynamics of the hepatic lesions in the left lobe;
Video 2: EUS-FNA of the target lesion was performed using a 19-gauge FNA needle. Videos are only available at the official website of the journal (www.eusjournal.com).
Acknowledgments
None.
Source of Funding
None.
Ethical Approval
The case was approved by the institutional review board.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report.
Conflict of Interest
The authors state that there are no conflicts of interest regarding this article.
Author Contributions
S. Wang conducted the literature review and was involved in drafting the manuscript and creating the video. Y. Wang was responsible for image acquisition. D. Zhao oversaw the conceptualization and supervised the project. All authors contributed to manuscript revision, read, and approved the submitted version.
Data Availability Statement
The authors confirm that the data supporting the findings of this article are available within the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Expert Committee on Endoscopic Ultrasonography of Chinese Medical Doctor Association. Chinese guideline for the clinical practice of endoscopic ultrasound-guided fine-needle aspiration/biopsy (condensed edition, 2021, Shanghai). Chin J Dig 2021;41(7):453–456.
- 2Zhang XB Fan YB Jing R, . Gastroenteropancreatic neuroendocrine neoplasms: Current development, challenges, and clinical perspectives. Mil Med Res 2024;11(1):35.38835066 10.1186/s 40779-024-00535-6PMC 11149301 · doi ↗ · pubmed ↗
- 3Sun C Zhao X Shi L, . Distinct ways to perform a liver biopsy: The core technique setups and updated understanding of these modalities. Endosc Ultrasound 2023;12(6):437–444.38948122 10.1097/eus.0000000000000035 PMC 11213587 · doi ↗ · pubmed ↗