EUS-guided ablation of a symptomatic renal cyst in a patient with autosomal dominant polycystic kidney disease
Jessica Arnold, Sebastian Zundler

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
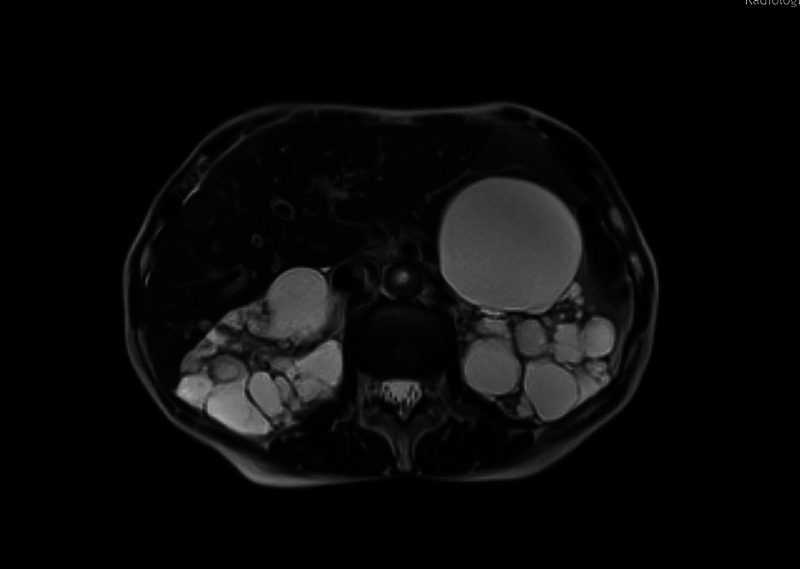 Figure 1
Figure 1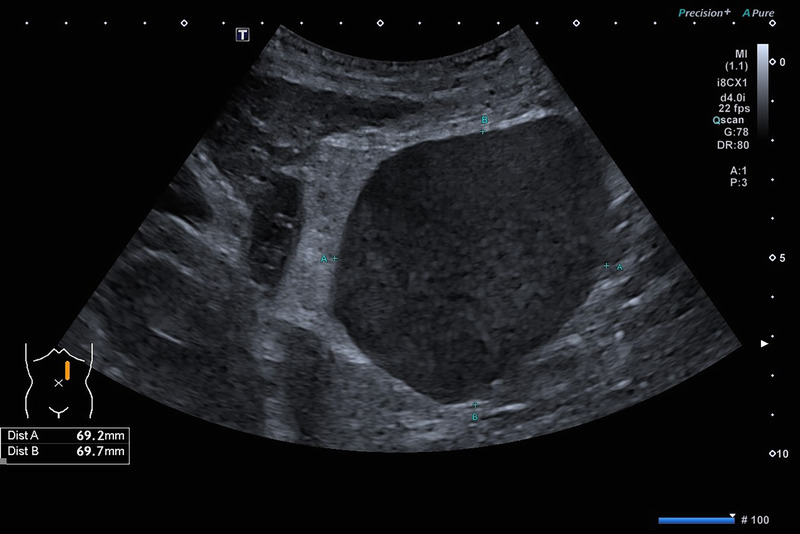 Figure 2
Figure 2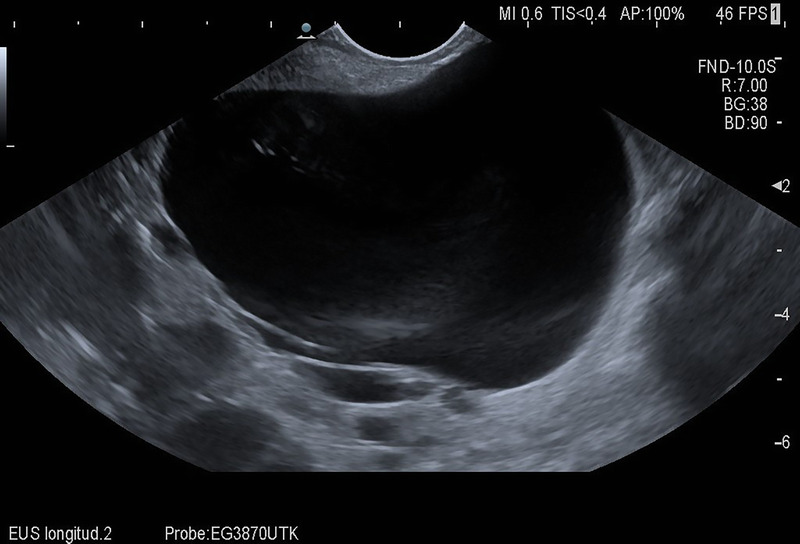 Figure 3
Figure 3 Figure 4
Figure 4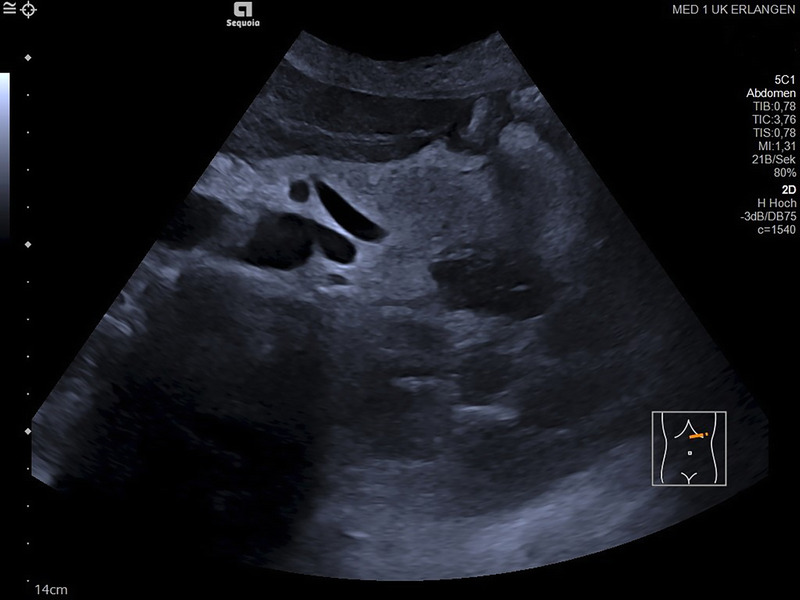 Figure 5
Figure 5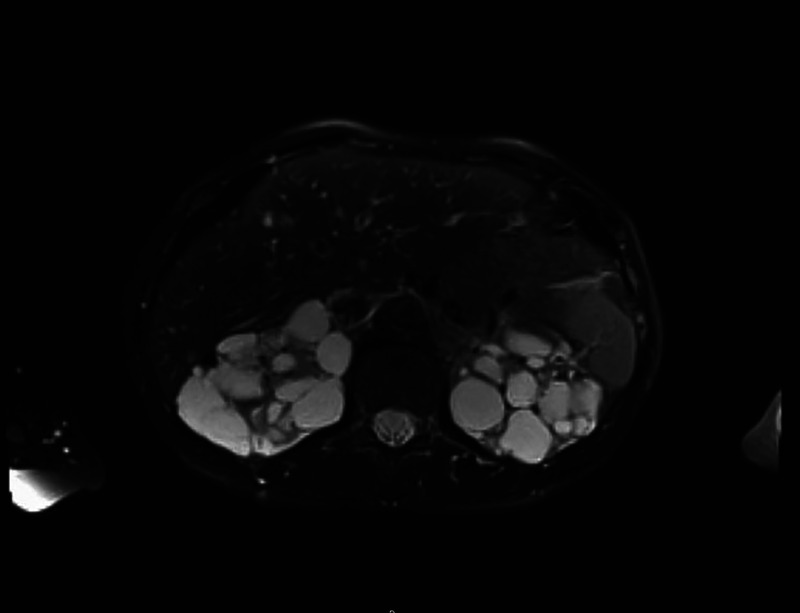 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Pancreatic and Hepatic Oncology Research · Pancreatitis Pathology and Treatment
A 66-year-old Caucasian woman with a history of autosomal dominant polycystic kidney disease (ADPKD) was referred to our center for EUS-guided drainage of a large pancreatic pseudocyst as diagnosed by magnetic resonance imaging (MRI) [Figure 1] and abdominal ultrasound [Figure 2]. She presented in reduced general condition and reported abdominal upper left quadrant pain and nausea for over 6 months. Laboratory results showed no signs of inflammation, and lipase levels were normal. Serum creatinine was mildly elevated, and the patient had mild microcytic hypochromic anemia.
EUS showed a cyst with 8-cm diameter between the pancreatic tail, spleen, and left kidney [Figure 3]. Due to its thin-walled appearance, completely anechoic texture, and the direct relation to the polycystic kidney as well as the missing history of pancreatitis, we diagnosed a symptomatic renal cyst rather than a pancreatic pseudocyst.
Because the patient was not considered a good candidate for surgery, we decided to perform EUS-guided ethanol ablation of the cyst. Thus, puncture with a 19G fine-needle aspiration (FNA) needle was performed, and 160 mL of clear, slightly yellowish fluid was aspirated [Figure 4]. Subsequently, 80 mL of 95% ethanol was instilled, left within the cyst for 10 minutes and subsequently re-aspirated.
No immediate complications occurred, systemic ethanol levels remained negative, and the abdominal pain and nausea fully resolved. On follow-up abdominal ultrasound 3 days later, the cyst was no longer visible [Figure 5]. Similarly, 4 weeks later, MRI confirmed a complete regression of the cyst [Figure 6].
This is one of the first reports of EUS-guided ethanol ablation of a renal cyst. Previously, percutaneous ethanol ablation of hepatic and renal cysts has been described to be safe and effective.^[1–3]^ Consistently, in our patient, this approach achieved full resolution of the cyst along with immediate symptom relief. Thus, endotherapy of symptomatic renal cysts may be considered on a case-by-case basis depending on accessibility and fitness for surgery.
Ethical Approval
Not applicable.
Informed Consent
Patient consent for publication was obtained.
Source of Funding
None.
Conflicts of Interest
None
Author Contributions
Both authors contributed to the study conception and design. Intervention was performed by Sebastian Zundler, follow-up care was co-ordinated by Jessica Arnold. The authors jointly wrote the manuscript and approved the final version.
Data Availability Statement
None
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee S Seo DW Paik WH, . Ethanol lavage of huge hepatic cysts by using EUS guidance and a percutaneous approach. Gastrointest Endosc 2014;80(6):1014–1021. doi:10.1016/j.gie.2014.03.037.24890421 · doi ↗ · pubmed ↗
- 2Singh I Mehrotra G. Selective ablation of symptomatic dominant renal cysts using 99% ethanol in adult polycystic kidney disease. Urology 2006;68(3):482–487. doi:10.1016/j.urology.2006.03.080.17010722 · doi ↗ · pubmed ↗
- 3Mohsen T Gomha MA. Treatment of symptomatic simple renal cysts by percutaneous aspiration and ethanol sclerotherapy. BJU Int 2005;96(9):1369–1372. doi:10.1111/j.1464-410X.2005.05851.x.16287460 · doi ↗ · pubmed ↗