Impact of frailty on postoperative delirium in ICU patients aged 65 and older: a systematic review
Denise Schindele, John McDonough, Tilmann Müller-Wolff

TL;DR
This study finds that frailty in older ICU patients increases the risk of postoperative delirium and other complications.
Contribution
The paper is the first systematic review to specifically examine the link between frailty and postoperative delirium in ICU patients aged 65 and older.
Findings
Frail ICU patients aged 65 and older had higher rates of postoperative delirium compared to non-frail patients.
Frail patients experienced more complications like acute kidney injury and prolonged ventilation.
The review identified five studies with moderate quality, but noted significant methodological heterogeneity.
Abstract
The objective was to assess whether frailty is associated with an increased risk of postoperative delirium (POD) in intensive care unit (ICU) patients aged 65 years and older. A systematic review was conducted in accordance with Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. MEDLINE (via PubMed) and the Cochrane Library were searched for studies published between August 2014 and January 2025, assessing frailty with validated instruments and reporting POD during ICU stay. While the search strategy was not limited to a specific study design, only observational studies met the inclusion criteria. Study quality was appraised using the Newcastle-Ottawa Scale (NOS). Due to methodological heterogeneity, results were synthesised narratively. This review targeted the intensive care setting specifically, including studies conducted in hospital-based ICUs in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
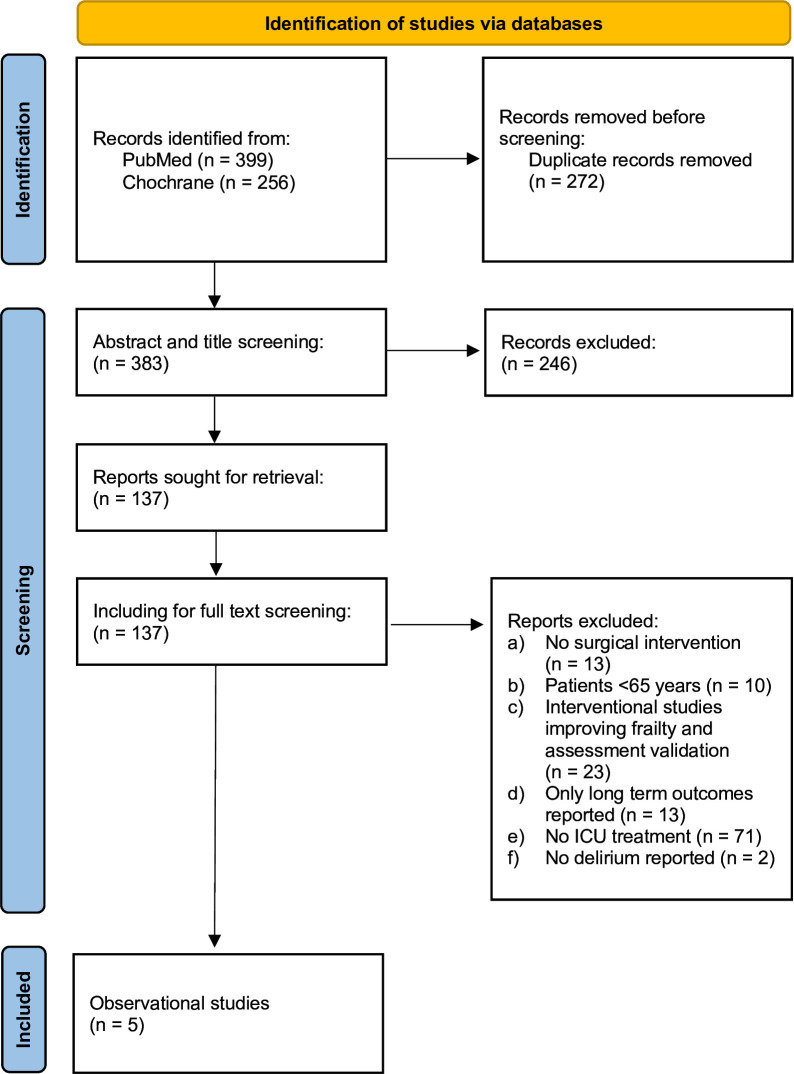 Figure 1
Figure 1| Author | n | ICU discipline | Frailty score | Delirium score | Primary outcomes | ICU complications | Follow-up |
|---|---|---|---|---|---|---|---|
| Bäck | 604 | Elective and non-elective cardiac surgery | CAF (frailty prevalence 25%) | Not reported | Mortality | AKI, need for reoperation, delirium, MV | 30 days after surgery |
| López Cuenca | 132 | Interdisciplinary ICU | FRAIL Scale (frailty prevalence 34.9%) | Not reported | Mortality | AKI, bleeding, delirium | 1 and 6 months after ICU discharge |
| Nomura | 133 | Cardiac surgery | Fried Frailty Scale (frailty prevalence 33,1%) | CAM, CAM-ICU | Delirium | Mortality, hospital LOS | 1 and 12 months after surgery |
| Lal | 96 | Cardiac surgery | EFS (frailty prevalence 10%) | Not reported | Hospital LOS | AKI, re-sternotomy, delirium | 12 months after ICU discharge |
| Cheng | 2080 | Cardiac surgery | mFI (frailty prevalence 29.5%) | CAM-ICU | Delirium | MV, mortality, hospital LOS | Not reported |
| Study | Delirium prevalence in frail patients | OR for POD (95% CI) | P value |
|---|---|---|---|
| Bäck | 7% | 5.0 (1.6 to 16.0) | 0.006 |
| Nomura | 48% | 6.31 (1.18 to 33.74) | 0.03 |
| López Cuenca | 11% | 0.93 (0.30 to 2.89) | 0.57 |
| Lal | 10% | 1.25 (0.92 to 1.71) | 0.161 |
| Cheng | 29.2% | 1.61 (1.23 to 2.10) | <0.01 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Intensive Care Unit Cognitive Disorders · Sepsis Diagnosis and Treatment
Introduction
Surgical interventions are common among older adults and frequently require intensive care support. In Germany alone, over 6 million patients aged 65–80 underwent surgery in 2021, and more than 400 000 required intensive care treatment.1 This growing demand reflects demographic shifts and increasing surgical complexity in ageing populations.2
There is a long history of confusion being reported in postoperative patients.3 Older patients are at heightened risk of adverse outcomes in the postoperative period.4 While advanced age itself is a known risk factor, the presence of multimorbidity, functional decline and frailty significantly contribute to perioperative vulnerability.5 Frailty, in particular, represents a multidimensional geriatric syndrome characterised by a progressive decline in physiological reserves, leading to impaired homeostasis and increased susceptibility to stressors.6
The pathophysiological burden of frailty, when combined with surgical trauma, has been linked to a higher incidence of severe complications, including postoperative delirium (POD).579 POD is a serious and potentially preventable complication in perioperative and critical care.10 It is defined as an acute neuropsychiatric syndrome characterised by fluctuating disturbances in attention, awareness and cognition, often accompanied by disorganised thinking and altered consciousness. POD is associated with adverse outcomes, including prolonged hospitalisation, increased morbidity and mortality, and long-term cognitive decline.11 Prevalence estimates in intensive care settings vary widely, ranging from 20% to 80% depending on patient population and diagnostic methods.12 The aetiology of POD is complex and multifactorial. Several risk factors are specific to the intensive care context, including sedation, sleep disruption, immobility and iatrogenic complications.
Symptoms may be overlooked or misattributed to other neuropsychiatric disorders or medication effects, contributing to underdiagnosis.12 One of the predisposing factors is increased age,12 and with the increased age, frailty is a common factor.6
Existing systematic reviews and meta-analyses have examined the association between frailty and delirium in hospitalised older adults.9 10 13 14 A recent meta-analysis by Gracie et al (2021) demonstrated that frailty was associated with more than twice the odds of developing POD (OR 2.14, 95% CI 1.43 to 3.19).
However, these reviews predominantly included general hospital populations or mixed surgical cohorts and did not differentiate postoperative intensive care unit (ICU) patients from other settings. As a result, the applicability of their findings to critically ill postoperative adults remains limited.
The ICU differs substantially from general wards, with factors such as mechanical ventilation, sedative exposure, haemodynamic instability and acute physiological stressors playing a key role in delirium development.12 Despite these unique risks, no systematic review has focused specifically on the relationship between frailty and POD in postoperative ICU patients aged ≥65 years. Existing evidence therefore lacks a targeted synthesis for this distinct high-risk subgroup. Addressing this gap is essential to determine whether frailty consistently predicts POD under ICU-specific conditions and to support the development of tailored preventive strategies in critical care settings.
Background
Frailty is a multidimensional geriatric syndrome that extends beyond chronological age and affects multiple physiological systems.5 6 It is characterised by diminished strength, endurance and physiological function, leading to increased vulnerability to stressors such as surgery and critical illness. Rather than reflecting a single organ dysfunction, frailty indicates a global decline in physiological reserve.6
Despite its clinical relevance, frailty remains difficult to assess in acute care contexts. In ICU settings, no universally accepted standard exists, and a wide variety of instruments are used.15 16
Many of the available frailty instruments are derived from the Fried frailty phenotype6 and the Clinical Frailty Scale (CFS).17 These tools vary in their complexity and clinical feasibility, which contributes to heterogeneity in frailty identification and risk stratification.61517
Given the variability in frailty assessment across ICU settings, a clearer understanding of how different instruments perform in postoperative critical care may support more consistent risk stratification and guide the selection of feasible tools for routine clinical practice.
Aim
The aim of this systematic review is to assess whether frailty is associated with an increased risk of POD in ICU patients aged 65 years and older.
The review addresses the question: Among postoperative ICU patients aged ≥65 years, is frailty associated with an increased risk of developing POD compared with non-frail patients?
Design and methods
patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this systematic review.
Research ethics approval
This study is a systematic review of previously published literature. No primary data were collected and no human participants were directly involved. Therefore, ethical approval was not required.
Design
A systematic literature search following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (online supplemental A)18 was conducted to identify relevant studies addressing the research question.
The protocol for the systematic review was duly registered in Open Science Framework (OSF) (registration: https://doi.org/10.17605/OSF.IO/7TWQ8). While the search strategy was not limited to a specific study design, only observational studies met the inclusion criteria.
Due to methodological differences across the included studies, particularly in the definitions and assessment of frailty and POD, we applied a narrative synthesis to summarise the findings.
Search strategy
The literature search was conducted in MEDLINE (via PubMed) and the Cochrane Library. These databases were selected because they provide the most comprehensive indexing of clinical, perioperative and critical care literature, including the majority of studies relevant to frailty and delirium. Given the highly specific focus on postoperative ICU patients aged ≥65 years, the evidence base is primarily concentrated in these core biomedical databases. To enhance completeness, the reference lists of all included studies were also screened; however, no additional eligible studies were identified. The initial search took place between August and September 2024 and was updated in January 2025. We acknowledge that the restricted database selection may have limited the scope of retrieved studies.
The search strategy was systematically developed, incorporating Medical Subject Headings terms and free-text keywords. Key terms included ‘frailty’, ‘postoperative delirium’, ‘intensive care unit’ and ‘aged’. The search strings were customised for each database and combined using Boolean operators to ensure a comprehensive yet targeted retrieval of studies. A detailed description and the complete search strings of the search strategy are provided in the search protocol (online supplemental B). All search results were imported into a reference management software (EndNote V.21.5), and duplicates were removed prior to screening. In addition, the reference lists of all included studies were systematically screened to identify further eligible publications; however, no additional studies meeting the predefined inclusion criteria were identified.
Inclusion and exclusion criteria
The eligibility criteria were refined as follows:
Observational studies (prospective or retrospective cohort studies) published between 2014 and 2025. (Rationale: Only observational studies are suitable for assessing associations relevant to the research question.)Patients aged ≥65 years, assessed with a validated frailty instrument (eg, Fried Frailty Scale, Edmonton Frailty Scale, FRAIL Scale Fatigue, Resistance, Ambulation, Illnesses, and Loss of weight), modified Frailty Index (mFI), CFS).Studies investigating postoperative adult patients treated in an ICU, irrespective of surgical discipline.Studies reporting POD occurring during the ICU stay, assessed using validated tools (eg, confusion assessment method (CAM), CAM-ICU) or documented clinical diagnosis. (No restrictions were applied regarding delirium assessment method.)
Exclusion criteria:
Studies not involving surgical patients (eg, medical ICU admissions).Studies including patients younger than 65 years.Interventional trials targeting frailty improvement and validation-only studies not reporting POD outcomes.Studies focusing exclusively on long-term outcomes (eg, 6-month cognitive follow-up) without postoperative ICU delirium data.Studies in which patients did not receive ICU treatment during the postoperative period.Studies that did not report delirium as an outcome.
Additional exclusions:
Abstracts, conference abstracts, qualitative studies, case reports, secondary analyses and studies not published in English or German.
Systematic reviews and meta-analyses were excluded from the primary analysis but used for contextualisation of the evidence base.
Study selection
The study selection process followed a structured approach to ensure methodological rigour. Initially, duplicate records and grey literature were removed. Subsequently, two independent reviewers (DS and TMW) screened the titles and abstracts for relevance, applying the predefined inclusion and exclusion criteria. Any discrepancies between the reviewers were resolved through discussion.
Following this, a full-text screening was conducted using the same independent review process. Studies that did not meet the eligibility criteria were excluded, with reasons for exclusion systematically documented. The final selection of studies was verified for consistency, ensuring that all included studies aligned with the review’s objectives.
Quality appraisal
Quality assessment of the included observational studies was conducted using the Newcastle-Ottawa Scale (NOS), which evaluates methodological quality across three domains: selection, comparability and outcome assessment.19 Two reviewers independently applied the NOS criteria, with disagreements resolved through discussion. No modifications to the original tool were made.
Data extraction
Data extraction was performed independently by two reviewers using a standardised extraction sheet. Extracted variables included study characteristics (author, year, country, sample size, setting), patient demographics, frailty assessment tools, POD diagnosis methods and ICU outcomes.
Synthesis
A synthesis without meta-analysis approach was used to summarise the results of the included studies. Data were categorised based on frailty assessment tools, delirium diagnosis methods and reported ICU outcomes to facilitate structured comparison.
Results
Out of 655 identified search results, five studies were included. The results are shown in the PRISMA flowchart (figure 1).18
Search results, PRISMA flow diagram. ICU, intensive care unit; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Quality appraisal
The methodological quality of the included studies was moderate, with NOS scores ranging from 5 to 7. Several potential sources of bias were identified. The representativeness of the exposed cohort varied, as some studies focused on specific patient groups, such as those undergoing cardiac surgery, which may limit the generalisability of findings to broader ICU populations. While most studies accounted for major confounders, variability in frailty assessment methods and delirium diagnostic criteria introduced heterogeneity, potentially affecting comparability. Differences in delirium diagnosis were evident, with some studies using standardised tools such as the CAM or CAM-ICU, whereas others relied on clinical judgement, leading to potential inconsistencies in outcome classification. Additionally, the follow-up periods varied, with some studies lacking long-term delirium outcome data, which may have influenced the ability to assess POD recurrence and its prolonged effects. Despite these methodological limitations, the overall study quality suggests that the findings are robust. However, caution is warranted when interpreting the results due to the heterogeneity in study designs and outcome assessment methods.
No study was excluded from the systematic review on the basis of its quality (online supplemental C). The table 1 reports the evaluation of selection, comparability and outcome domains. Higher scores indicate higher methodological quality. Follow-up periods and adequacy of outcome assessment are reflected in the corresponding NOS domains.
Study selection and characteristics
Table 1 presents the main characteristics and the extracted data of the included studies, including sample size, surgical discipline, frailty and delirium assessment methods, primary outcomes, follow-up periods and reported ICU-related complications. A comprehensive version of this table, including additional variables such as study design, age criteria and country, is provided in the supplementary material (online supplemental D). In table 1 frailty prevalence refers exclusively to patients classified as frail according to the respective assessment tool. Prefrail individuals were not included in these proportions. A detailed breakdown of frailty categories is provided in the section ‘Frailty Assessment Tools and Prevalence’.
The five included studies showed similar demographic patterns, with patients typically aged 73–78 years and predominantly male (68–84%). Most cohorts consisted of individuals undergoing major cardiac surgery.2023
Frailty assessment tools and prevalence
The included studies employed a variety of validated tools to assess frailty, reflecting diverse approaches tailored to the multifaceted nature of the condition.2024 In the study by Bäck et al21 604 patients were assessed using the comprehensive assessment of frailty, a multifaceted tool that integrates physical performance tests (eg, gait speed and grip strength) with clinical evaluations of comorbidities and nutritional status. This instrument integrates objective metrics and clinician judgement to classify patients as non-frail, prefrail or frail. In their study, 25% of the patients were classified as frail and 30% as prefrail.21
Nomura et al23 employed the Fried Frailty Scale in 133 patients, a tool that assesses frailty across five domains: unintentional weight loss, weakness, exhaustion, slowness and low physical activity. Patients were categorised as non-frail, prefrail or frail based on their cumulative scores. The Fried Frailty Scale is predicated on a phenotypic model of frailty, emphasising physical capabilities. In this study, 33.1% of the patients were classified as frail and 55.6% as prefrail.23
The FRAIL Scale, used by López Cuenca et al24 in 132 patients, uses five simple criteria: fatigue, resistance, ambulation, illness and weight loss. This instrument categorises individuals as robust (0 points), prefrail (1–2 points) or frail (3–5 points), thereby providing a straightforward and expeditious assessment method. The study reported that 34.9% of the ICU patients were classified as frail and 16.7% as prefrail.24
Lal et al22 applied the Edmonton Frail Scale (EFS) in 96 patients, which evaluates frailty across multiple domains, including cognitive function, physical performance, medication use and social support. The EFS offers a comprehensive yet efficient assessment suitable for non-specialists, who can use it to classify patients as non-frail, prefrail or frail based on their scores. In the present cohort, 10% of the patients were categorised as frail and 23% as prefrail.22
In the only retrospective study by Cheng et al20 2080 patients were screened by the adopted mFI, a tool based on a deficit accumulation model. This index integrates 11 health-related factors, including comorbidities and functional status, to calculate a cumulative score. Patients were grouped into two categories: non-frail (mFI 0–2) or frail (mFI ≥3). This approach underscores a more comprehensive, multidimensional perspective. Among the 2080 participants, 29.5% were identified as frail.20
Incidence of POD
The included studies examined the incidence of POD in relation to frailty, with varying associations.2024
In the study by Bäck et al21 POD was identified through clinical assessment. No validated instrument was used. The incidence of POD was found to be 7% in patients with frailty compared with 3% in patients without frailty. The analysis revealed a relationship between frailty and an elevated risk of POD, with an OR of 5.0 (95% CI 1.6 to 16.0; p=0.006).21
Nomura et al23 employed the CAM and the adapted version for intensive care units, the CAM-ICU, to diagnose POD, reporting an incidence of 48% in frail and prefrail patients, compared with 13% in non-frail patients. The adjusted OR for POD in frail patients was 6.31 (95% CI 1.18 to 33.74; p=0.03).23
López Cuenca et al24 identified delirium through routine clinical documentation by the ICU team, without the use of a structured delirium screening tool such as CAM or CAM-ICU, and without a formal validation procedure. The incidence of POD was documented to be 11% in patients categorised as frail and 12% in those designated as non-frail. No relationship was found between frailty and delirium (OR 0.93, 95% CI 0.30 to 2.89, p=0.57).
In the study by Lal et al,22 the CAM-ICU was used to diagnose delirium. The incidence was 10% in frail patients, 14% in vulnerable patients and 5% in non-frail patients. While frail patients exhibited a higher incidence of delirium, the association between frailty and delirium was not statistically significant (OR: 1.25, 95% CI 0.92 to 1.71, p=0.161).22
Cheng et al20 employed the CAM-ICU, augmented by nursing notes, to diagnose delirium. The prevalence of delirium was 29.2% in patients with frailty and 16.4% in patients without frailty. Frailty was associated with POD, with an adjusted OR of 1.61 (95% CI 1.23 to 2.10).20
Overall, the findings indicate a consistent trend of increased POD among frail patients. However, variations in delirium diagnostic methods, study designs and patient populations may contribute to differences in reported POD incidence. Table 2 summarises the ORs and CIs for POD in frail patients compared with non-frail individuals.
ICU-related outcomes
Furthermore, the five studies examined several postoperative complications in addition to POD.2024 Frail patients demonstrated higher rates of acute kidney injury (AKI),21 22 24 prolonged mechanical ventilation20 21 and reoperation due to bleeding or other causes compared with non-frail patients.21 22 24 Frail patients also have a higher mortality rate and a prolonged hospitalisation compared with non-frail patients.2024
Discussion
This review suggests that frailty may be associated with an increased risk of POD in ICU patients aged 65 years and older. Reported POD incidence ranged from 7% to 48%, with frail individuals consistently showing higher rates. In addition, frailty was linked to complications such as AKI, prolonged mechanical ventilation and reoperation.
Substantial methodological heterogeneity was identified due to differences in population, frailty measures, delirium assessments and follow-up periods across the studies. Frailty was assessed using various instruments, ranging from phenotype-based tools (eg, Fried Frailty Scale) to multidimensional models (eg, Edmonton Frailty Scale) and delirium was diagnosed using different approaches, including validated instruments (CAM, CAM-ICU) and unstructured clinical assessments. These inconsistencies likely contributed to variation in outcomes and complicated direct comparisons. Across the included studies, frailty was operationalised using diverse tools, including the Fried Frailty Scale, FRAIL Scale, Edmonton Frailty Scale, mFI and the CAF, reflecting the absence of a uniform frailty construct in ICU research. This variability affects comparability across studies and highlights the broader challenge of establishing consensus on frailty measurement in critical care populations.25 26
The findings are broadly consistent with previous research showing that frailty contributes to adverse ICU outcomes, including delirium, prolonged length of stay and mortality.52731
Although the association between frailty and POD is well supported in general hospital populations, most previous studies did not specifically investigate ICU cohorts, highlighting the need for research focused on critically ill patients.7 9 13 14 32
This review identified only five eligible ICU studies.2024
Four were conducted in cardiac surgery populations,2023 which limits the generalisability of the findings to broader surgical populations. Only one study included an interdisciplinary ICU cohort,24 indicating that evidence for non-cardiac surgical patients remains sparse.
Cardiac surgery-related factors (eg, extracorporeal circulation) may influence delirium risk differently from other specialties,33 further restricting external validity.
Recent evidence from a multicentre study by Dólera Moreno et al34 indicates that frailty is also associated with adverse outcomes in predominantly medical ICU populations. This suggests that the prognostic relevance of frailty may differ between surgical and medical ICU settings due to their distinct clinical pathways.34
Recent findings from Molina Lobo et al35 further indicate that frailty and even prefrailty may be prognostically relevant across mixed ICU populations of all ages. Although not specific to postoperative patients, these findings reinforce that frailty is not confined to older adults and support population-specific analyses.35 The meta-analysis conducted by Gracie et al36 reported a more than twofold increased odds of POD in frail patients. Their pooled analysis of nine studies demonstrated that frail patients had more than twice the odds of developing POD compared with non-frail patients (OR=2.14, 95% CI 1.43 to 3.19). Importantly, this analysis also highlighted the relatively low heterogeneity (I²=5.5), suggesting robust findings despite variations in frailty and delirium assessment tools.36 These results are broadly consistent with the findings of the present review, although important methodological differences between both analyses must be considered. While the meta-analysis by Gracie et al36 included nine studies, several of these were not eligible for our review, which applied stricter criteria requiring postoperative ICU admission, validated frailty assessment and delirium occurring during the ICU stay. These differences explain the smaller number of included studies and reflect the narrower clinical focus of the present review. Studies in mixed-age ICU populations37 38 also reported higher delirium rates among frail patients, although population differences limit comparability with postoperative cohorts.
In interpreting these findings, several methodological limitations should be considered. First, the number of eligible studies was small (n=5), limiting generalisability and reducing the robustness of conclusions. Second, the predominance of cardiac surgery cohorts constrains applicability to other surgical ICU populations. Third, substantial heterogeneity in frailty instruments, delirium assessment methods and follow-up periods precluded quantitative synthesis.
Moreover, none of the included studies applied the CFS, despite its widespread use in intensive care medicine as a validated and clinically established frailty measure.25 This absence limits comparability with the broader ICU frailty literature and may have contributed to variation in frailty classification across studies.
In addition, only two of the included studies evaluated delirium as a predefined primary endpoint. In contrast, the studies by Bäck et al21 and Lal et al22 assessed delirium as a secondary outcome using systematic clinical or tool-based assessments, whereas López Cuenca et al24 documented delirium solely as a routine clinical complication without a structured screening procedure. The absence of predefined delirium endpoints in three studies reduces statistical power and increases the risk of outcome misclassification, thereby limiting the strength of conclusions regarding the association between frailty and POD. Fourth, methodological quality was moderate (NOS scores 5–7), with limited adjustment for important confounders such as baseline cognitive impairment, anticholinergic burden, premedication and comorbidity burden. Finally, differences in study design and reporting may have introduced residual confounding. Together, these limitations indicate that the evidence base remains preliminary and should be interpreted with caution.
Another important source of potential bias relates to baseline cognitive impairment. Dementia and preoperative cognitive decline are strong predictors of delirium and may confound the association between frailty and POD if not adequately assessed or adjusted for. Several frailty instruments, particularly multidimensional measures, partially capture cognitive components, which may increase their predictive value for delirium but also blur the distinction between frailty and pre-existing cognitive deficits.39 40 Future studies should therefore include standardised preoperative cognitive assessments to improve comparability and reduce misclassification.
In addition, pharmacological and clinical factors such as anticholinergic burden, premedication (eg, benzodiazepines or sedatives) and comorbidities may influence delirium risk and could act as confounders, as previously demonstrated in studies identifying anticholinergic load and sedative exposure as established delirium risk factors41 and comorbidity burden as a contributor to delirium vulnerability.29 Most included studies provided limited reporting or adjustment for these variables, which may have contributed to residual confounding. Standardised documentation of medication profiles and comorbidity burden would strengthen the interpretability of future research.
Overall, this review suggests that frailty may represent a clinically relevant marker for increased POD risk in postoperative ICU patients aged ≥65 years. Recognising frailty as a potential vulnerability factor may support closer monitoring and targeted supportive measures, although evidence for frailty-specific interventions remains limited. Future studies should include broader surgical populations, apply standardised frailty and delirium assessments, and evaluate whether tailored interventions can reduce POD risk in frail ICU patients.
Conclusion
Frailty is a potential risk factor of POD in ICU patients aged 65 years and older. Across the included studies, frail individuals tended to exhibit higher rates of POD and postoperative complications; however, the strength of this association varied between studies.
In clinical practice, frailty may serve as one component within a broader, multifactorial delirium risk assessment, helping to identify older ICU patients who may benefit from enhanced monitoring and non-pharmacological preventive strategies. However, the current evidence does not allow firm recommendations regarding specific interventions.
Future studies should include more diverse surgical populations, apply standardised and validated frailty and delirium assessment tools and evaluate whether targeted perioperative interventions can mitigate POD risk in frail patients. Improved methodological consistency will be essential to strengthen the evidence base and support the development of robust clinical recommendations.
Implications and recommendations for practice
Early identification: Frailty screening may be integrated into preoperative and ICU workflows, where feasible, to help identify older patients who could benefit from closer monitoring regarding delirium risk.Multidisciplinary collaboration: A multidisciplinary approach involving geriatricians, intensivists and general and advanced nursing staff may support more comprehensive care for frail ICU patients, acknowledging the complexity of their clinical needs.Standardisation: The use of standardised and validated frailty and delirium assessment tools could improve comparability across studies and strengthen the evidence base for future clinical decision-making.Targeted prevention strategies: Enhanced delirium monitoring, multimodal pain management and supportive interventions to maintain cognitive and physical activity may contribute to reducing POD risk in frail older adults, although further research is required to determine their effectiveness in ICU settings.
Supplementary material
10.1136/bmjopen-2025-108249online supplemental file 1
10.1136/bmjopen-2025-108249online supplemental file 2
10.1136/bmjopen-2025-108249online supplemental file 3
10.1136/bmjopen-2025-108249online supplemental file 4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Statistisches bundesamt Gesundheit. fallpauschalenbezogene krankenhausstatistik (drg-statistik) operationen und prozeduren der vollstationären patientinnen und patienten in krankenhäusern (4-steller)2021 Availablehttps://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Krankenhaeuser/Publikationen/Downloads-Krankenhaeuser/operationen-prozeduren-5231401217014.pdf?__blob=publication File
- 2Jung C Bruno RR Wernly B et al Frailty as a Prognostic Indicator in Intensive Care Dtsch Arztebl Int 20201176687310.3238/arztebl.2020.066833357351 PMC 7838379 · doi ↗ · pubmed ↗
- 3Osterbrink J Mayer H Fiedler C et al Incidence and prevalence of postoperative acute confusion in heart surgery patients after coronary artery bypass and heart valve replacement surgeries Pflege 2002151788910.1024/1012-5302.15.4.17812244827 · doi ↗ · pubmed ↗
- 4Wobith M Acikgöz A Grosser K et al Preoperative cognitive function in very old patients : Influence on the complication rate and length of hospitalization Chirurg 201990930510.1007/s 00104-019-01028-231468065 · doi ↗ · pubmed ↗
- 5Peri-interventional outcome study in the elderly in Europe: A 30-day prospective cohort study Eur J Anaesthesiol 20223919820910.1097/EJA.000000000000163934799496 PMC 8815832 · doi ↗ · pubmed ↗
- 6Fried LP Tangen CM Walston J et al Frailty in Older Adults: Evidence for a Phenotype The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 200156 M 1465710.1093/gerona/56.3.M 14611253156 · doi ↗ · pubmed ↗
- 7Gong S Qian D Riazi S et al Association Between the FRAIL Scale and Postoperative Complications in Older Surgical Patients: A Systematic Review and Meta-Analysis Anesth Analg 20231362516110.1213/ANE.000000000000627236638509 PMC 9812423 · doi ↗ · pubmed ↗
- 8Mazzola P Tassistro E Di Santo S et al The relationship between frailty and delirium: insights from the 2017 Delirium Day study Age Ageing 2021501593910.1093/ageing/afab 04233792656 · doi ↗ · pubmed ↗