Association of antioxidant-added highly cross-linked polyethylene on revision risk: a registry-based study of 198,073 total hip replacements from the Australian Orthopaedic Association National Joint Replacement Registry between 2014 and 2023
Peter L LEWIS, David G CAMPBELL, Peiyao DU, Helena OAKEY, Richard N de STEIGER, Paul N SMITH

TL;DR
Adding antioxidant to a type of plastic used in hip replacements may reduce the need for revision surgeries after three years, according to a study of over 198,000 cases.
Contribution
This study provides the first large-scale, registry-based evidence on the long-term performance of antioxidant-added polyethylene in hip replacements.
Findings
THR with antioxidant-added polyethylene had a 37% lower revision rate after 3 years compared to standard polyethylene.
Revisions due to loosening, wear, and fracture were lower with antioxidant-added polyethylene.
No difference was found in revisions due to dislocation or infection between the two groups.
Abstract
Adding antioxidant to highly cross-linked polyethylene (XLPE) is proposed to improve oxidation resistance and decrease wear in total hip replacements (THR), but long-term performance is unknown. We aimed to compare the revision rates of THR using cementless acetabular components where the insert was made of either XLPE with antioxidant (AOXLPE) or XLPE, using data from a large national registry. The population was THR from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) in the 10-year period 2014–2023 with modular cementless acetabular components and ceramic or metal femoral heads used for osteoarthritis. We compared primary THR using XLPE with antioxidant (AOXLPE) acetabular inserts with XLPE acetabular inserts. The outcome measured was all-cause revision. Cumulative percentage revision (CPR) was calculated using the Kaplan–Meier method, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
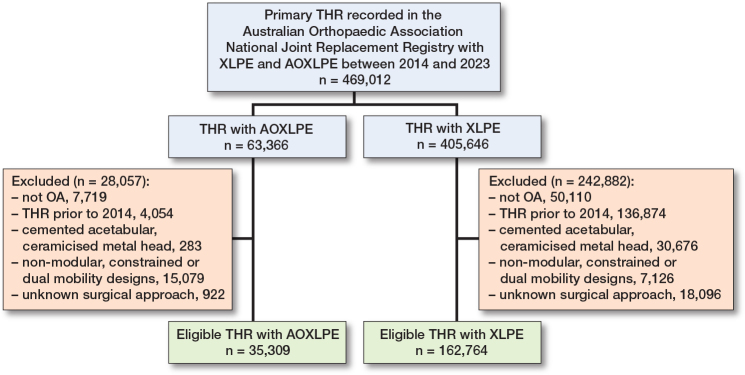 Figure 1
Figure 1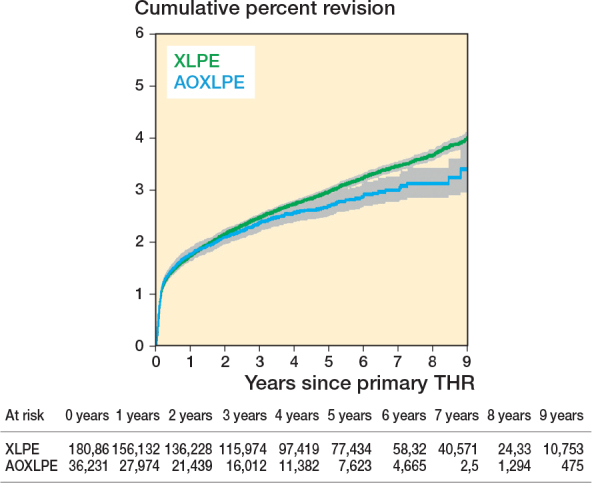 Figure 2
Figure 2| Variable | XLPE | AOXLPE | Total |
|---|---|---|---|
| Follow-up, years | |||
| Mean (SD) | 4 (2.5) | 2.9 (2.2) | 3.8 (2.5) |
| Median (IQR) | 4 (1.8–6.1) | 2.6 (1.1–4.4) | 3.6 (1.6–.9) |
| Minimum | 0 | 0 | 0 |
| Maximum | 9.9 | 9.2 | 9.9 |
| Age | |||
| Mean (SD) | 69 (10) | 68 (10) | 69 (10) |
| Median (IQR) | 70 (62–76) | 68 (61–75) | 70 (62–76) |
| Age group | |||
| < 55 | 14,584 (9.0) | 3,438 (9.7) | 18,022 (9.1) |
| 55–64 | 36,751 (23) | 8,936 (25) | 45,687 (23) |
| 65–74 | 60,402 (37) | 13,649 (39) | 74,051 (37) |
| ≥ 75 | 51,027 (31) | 9,286 (26) | 60,313 (30) |
| Sex | |||
| Male | 76,025 (47) | 16,922 (48) | 92,947 (47) |
| Female | 86,739 (53) | 18,387 (52) | 105,126 (53) |
| Body mass index category | |||
| Underweight | 1,085 (0.7) | 264 (0.8) | 1,349 (0.7) |
| Normal | 30,841 (20) | 7,525 (22) | 38,366 (20) |
| Pre obese | 57,187 (36) | 12,904 (37) | 70,091 (36) |
| Obese class 1 | 41,630 (26) | 8,592 (25) | 50,222 (26) |
| Obese class 2 | 18,056 (12) | 3,699 (11) | 21,755 (11) |
| Obese class 3 | 8,678 (5.5) | 1,708 (4.9) | 10,386 (5.4) |
| ASA score | |||
| 1 | 10,911 (6.7) | 3,153 (8.9) | 14,064 (7.1) |
| 2 | 86,223 (53) | 19,386 (55) | 105,609 (53) |
| 3 | 63,108 (39) | 12,331 (35) | 75,439 (38) |
| 4 | 2,286 (1.4) | 394 (1.1) | 2,680 (1.4) |
| 5 | 12 (0) | 1 (0) | 13 (0) |
| Head size | |||
| < 32 mm | 7,711 (4.7) | 235 (0.7) | 7,946 (4.0) |
| 32 mm | 72,784 (45) | 6,584 (19) | 79,368 (40) |
| > 32 mm | 82,269 (51) | 28,490 (81) | 110,759 (56) |
| Head material | |||
| Ceramic | 88,358 (54) | 27,439 (78) | 115,797 (59) |
| Metal | 74,406 (46) | 7,870 (22) | 82,276 (41) |
| Acetabular fixation | |||
| Cementless | 162,764 (100) | 35,309 (100) | 198,073 (100) |
| Femoral fixation | |||
| Cementless | 91,947 (57) | 28,397 (80) | 120,344 (61) |
| Cemented | 70,817 (43) | 6,912 (20) | 77,729 (39) |
| Surgical approach | |||
| Anterior | 34,537 (21) | 9,737 (28) | 44,274 (22) |
| Lateral | 27,430 (17) | 4,192 (12) | 31,622 (16) |
| Posterior | 100,797 (62) | 21,380 (61) | 122,177 (62) |
| Total | 162,764 | 35,309 | 198,073 |
| Revision diagnosis | XLPE | AOXLPE | ||
|---|---|---|---|---|
| Primaries revised n (%) | % of revisions | Primaries revised n (%) | % of revisions | |
| Infection | 1,368 (0.8) | 32 | 260 (0.7) | 34 |
| Prosthesis dislocation/instability | 1,022 (0.6) | 24 | 197 (0.6) | 26 |
| Fracture | 891 (0.5) | 21 | 148 (0.4) | 19 |
| Loosening | 641 (0.4) | 15 | 93 (0.3) | 12 |
| Pain | 73 (0.0) | 1.7 | 11 (0.0) | 1.4 |
| Leg length discrepancy | 71 (0.0) | 1.6 | 23 (0.1) | 3.0 |
| Malposition | 64 (0.0) | 1.5 | 13 (0.0) | 1.7 |
| Implant breakage stem | 25 (0.0) | 0.6 | 2 (0.0) | 0.3 |
| Incorrect sizing | 25 (0.0) | 0.6 | 5 (0.0) | 0.7 |
| Implant breakage acetabular insert | 22 (0.0) | 0.5 | 2 (0.0) | 0.3 |
| Lysis | 16 (0.0) | 0.4 | ||
| Metal-related pathology | 11 (0.0) | 0.3 | ||
| Heterotopic bone | 8 (0.0) | 0.2 | 1 (0.0) | 0.1 |
| Implant breakage acetabular | 8 (0.0) | 0.2 | ||
| Wear acetabular insert | 6 (0.0) | 0.1 | 1 (0.0) | 0.1 |
| Tumor | 5 (0.0) | 0.1 | 1 (0.0) | 0.1 |
| Implant breakage head | 2 (0.0) | 0.0 | ||
| Progression of disease | 1 (0.0) | 0.0 | ||
| Wear acetabulum | 1 (0.0) | 0.0 | ||
| Wear head | 1 (0.0) | 0.0 | ||
| Other | 66 (0.0) | 1.5 | 12 (0.0) | 1.6 |
| Revisions | 4,327 (2.7) | 100 | 769 (2.2) | 100 |
| Primary THRs | 162,764 | 35,309 | ||
| Type of evision | XLPE | AOXLPE | ||
|---|---|---|---|---|
| Primaries revised n (%) | % of revisions | Primaries revised n (%) | % of revisions | |
| Head and insert | 1,456 (0.9) | 34 | 276 (0.8) | 36 |
| Femoral component | 1,342 (0.8) | 31 | 231 (0.7) | 30 |
| Acetabular component | 645 (0.4) | 15 | 116 (0.3) | 15 |
| THR (femoral and acetabular) | 411 (0.3) | 9.5 | 81 (0.2) | 11 |
| Head only | 208 (0.1) | 4.8 | 40 (0.1) | 5.2 |
| Cement spacer | 122 (0.1) | 2.8 | 11 (0.0) | 1.4 |
| Minor components | 68 (0.0) | 1.6 | 5 (0.0) | 0.7 |
| Insert only | 48 (0.0) | 1.1 | 7 (0.0) | 0.9 |
| Removal of prostheses | 18 (0.0) | 0.4 | 1 (0.0) | 0.1 |
| Reinsertion of components | 7 (0.0) | 0.2 | ||
| Bipolar head and femoral | 2 (0.0) | 0.0 | 1 (0.0) | 0.1 |
| Revisions | 4,327 (2.7) | 100 | 769 (2.2) | 100 |
| Primary THRs | 162,764 | 35,309 | ||
| AOXLPE vs XLPE Time period | Unadjusted HR (CI) | P value | Adjusted HR (CI) | P value |
|---|---|---|---|---|
| 0–3 months | 1.01 (0.91–1.12) | 0.9 | 0.98 (0.88–1.09) | 0.7 |
| 3–6 months | 0.94 (0.73–1.21) | 0.6 | 0.91 (0.71–1.18) | 0.5 |
| 6–9 months | 1.08 (0.79–1.47) | 0.6 | 1.05 (0.77–1.43) | 0.7 |
| 9–36 months | 0.87 (0.74–1.03) | 0.1 | 0.85 (0.72–1.01) | 0.06 |
| >36 months | 0.64 (0.48–0.84) | 0.002 | 0.63 (0.47–0.83) | 0.001 |
| Reason for revision | Time period months | HR (CI) | P value | Adjusted HR (CI) | P value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Insert material | Revised | Total | 1-year | At risk | 5-year | At risk | 8-year | At risk | |||||
| Loosening | |||||||||||||
| AOXLPE | 93 | 35,309 | 0.2 (0.2–0.3) | 27,108 | 0.3 (0.3–0.4 | 6,895 | 0.4 (0.3–0.5) | 686 | 0–24 | 1.05 (0.83–1.33) | 0.7 | 0.87 (0.69–1.11) | 0.3 |
| XLPE | 641 | 162,764 | 0.2 (0.2–0.2) | 138,540 | 0.5 (0.4–0.5) | 61,601 | 0.6 (0.6–0.7) | 11,121 | > 24 | 0.28 (0.14–0.54) | < 0.001 | 0.22 (0.11–0.44) | < 0.001 |
| Wear-related causes | |||||||||||||
| AOXLPE | 96 | 35,309 | 0.2 (0.2–0.3) | 27,108 | 0.4 (0.3–0.4) | 6,895 | 0.4 (0.3–0.5) | 686 | 0–24 | 1.03 (0.82–1.30) | 0.8 | 0.86 (0.68–1.09) | 0.2 |
| XLPE | 685 | 162,764 | 0.2 (0.2–0.2) | 138,540 | 0.5 (0.5–0.5) | 61,601 | 0.7 (0.6–0.8) | 11,121 | > 24 | 0.26 (0.13–0.50) | < 0.001 | 0.21 (0.11–0.40) | < 0.001 |
| Fracture | |||||||||||||
| AOXLPE | 148 | 35,309 | 0.3 (0.3–0.4) | 27,108 | 0.5 (0.4–0.6) | 6,895 | 0.7 (0.6–1.0) | 686 | E.P. | 0.89 (0.75–1.06) | 0.2 | 0.80 (0.67–0.96) | 0.02 |
| XLPE | 891 | 162,764 | 0.4 (0.3–0.4) | 138,540 | 0.6 (0.6–0.6) | 61,601 | 0.8 (0.8–0.9) | 11,121 | |||||
| Dislocation/Instability | |||||||||||||
| AOXLPE | 197 | 35,309 | 0.4 (0.4–0.5) | 2,7108 | 0.7 (0.6–0.8) | 6,895 | 0.8 (0.7–0.9) | 686 | E.P. | 1.00 (0.86–1.17) | 1 | 1.14 (0.97–1.34) | 0.1 |
| XLPE | 1,022 | 162,764 | 0.4 (0.4–0.5) | 138,540 | 0.7 (0.7–0.8) | 61,601 | 0.8 (0.8–0.9) | 11,121 | |||||
| Infection | |||||||||||||
| AOXLPE | 260 | 35,309 | 0.7 (0.6–0.8) | 27108 | 0.8 (0.7–1.0) | 6,895 | 0.9 (0.8–1.0) | 686 | E.P. | 0.95 (0.83–1.08) | 0.4 | 0.97 (0.84–1.11) | 0.7 |
| XLPE | 1,368 | 162,764 | 0.7 (0.6–0.7) | 138540 | 0.9 (0.9–1.0) | 61,601 | 1.0 (1.0–1.1) | 11,121 | |||||
| Prosthesis factor | Time period months | HR (CI) | P value | Adjusted HR (CI) | P value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Insert material | Revised | Total | 1-year | At risk | 5-year | At risk | 8-year | At risk | |||||
| Head size < 32 mm | |||||||||||||
| AOXLPE | 10 | 235 | 3.5 (1.7–6.8) | 171 | 10 | 2 | E.P. | 1.11 (1.04–1.18) | 0.001 | 1.11 (1.04–1.18) | 0.002 | ||
| XLPE | 271 | 7,711 | 2.3 (2.0–2.6) | 6,876 | 3.7 ( 3.3–4.2) | 3,626 | 4.3 (3.8–4.9) | 858 | |||||
| Head size 32 mm | |||||||||||||
| AOXLPE | 158 | 6,584 | 1.8 (1.5–2.2) | 5,224 | 3.0 (2.5–3.5) | 1,271 | 3.3 (2.7–4.1) | 131 | E.P. | 1.61 (0.86–3.03) | 0.1 | 1.91 (1.01–3.60) | 0.04 |
| XLPE | 1,893 | 72,784 | 1.6 (1.5–1.7) | 64,515 | 2.8 (2.7–2.9) | 32,297 | 3.4 (3.2–3.6) | 6,018 | |||||
| Head size > 32 mm | |||||||||||||
| AOXLPE | 601 | 28,490 | 1.7 (1.5–1.9) | 21,713 | 2.6 (2 .4–2.8) | 5,614 | 3.0 (2.7–3.3) | 553 | 0–3 | 0.96 (0.85–1.09) | 0.5 | 0.95 (0.84–1.08) | 0.4 |
| XLPE | 2,163 | 82,269 | 1.8 (1.7–1.9) | 67,149 | 3.0 (2.9–3.2) | 25,678 | 3.9 (3.7–4.1) | 4,245 | 3–18 | 0.92 (0.77–1.09) | 0.3 | 0.91 (0.76–1.08) | 0.3 |
| Ceramic head | |||||||||||||
| AOXLPE | 540 | 27,439 | 1.5 (1.4–1.7) | 21,124 | 2.4 (2.2–2.7) | 5,517 | 2.8 (2.5–3.2) | 569 | E.P. | 0.86 (0.78–0.94) | 0.001 | 0.82 (0.75–0.91) | <0.001 |
| XLPE | 2,231 | 88,358 | 1.7 (1.6–1.8) | 73,293 | 2.9 (2.8–3.0) | 29,123 | 3.5 (3.4–3.7) | 4,678 | |||||
| Metal head | |||||||||||||
| AOXLPE | 229 | 7,870 | 2.4 (2.1–2.8) | 5,984 | 3.5 (3.1–4.0) | 1,378 | 3.8 3.2–4.5) | 117 | 0–3 | 1.48 (1.24,1.76) | < 0.001 | 1.39 (1.16–1.66) | < 0.001 |
| XLPE | 2,096 | 74,406 | 1.8 (1.7–1.9) | 65,247 | 3.0 (2.9–3.1) | 32,478 | 3.8 (3.6–4.0) | 6,443 | > 3 | 0.98 (0.79,1.22) | 0.9 | 0.93 (0.74–1.15) | 0.5 |
| Femur cementless | |||||||||||||
| AOXLPE | 598 | 28,397 | 1.7 (1.6–1.9) | 21810 | 2.5 (2.3–2.8) | 5,810 | 2.9 (2.6–3.2) | 607 | E.P. | 0.82 (0.75–0.90) | < 0.001 | 0.84 (0.76–0.92) | < 0.001 |
| XLPE | 2,690 | 91,947 | 1.9 (1.8–2.0) | 78,434 | 3.2 (3.1,–3.4) | 35,431 | 3.9 (3.7–4.1) | 6,242 | |||||
| Femur cemented | |||||||||||||
| AOXLPE | 171 | 6,912 | 1.9 (1.6–2.2) | 5,298 | 3.3 (2.8–3.9) | 1,085 | 4.0 (3.0–5.2) | 79 | E.P. | 1.23 (1.05–1.44) | 0.01 | 1.26 (1.08–1.48) | 0.004 |
| XLPE | 1,637 | 70,817 | 1.5 (1.4–1.6) | 60,106 | 2.6 (2.5,–2.7) | 34,622 | 3,4 (3.2–3.6) | 4,879 | |||||
| Anterior approach | |||||||||||||
| AOXLPE | 161 | 9,737 | 1.3 (1.1–1.6) | 7,696 | 1.9 (1.6–2.3) | 2,268 | 2.4 (1.9–3.1) | 220 | E.P. | 0.70 (0.60–0.83) | < 0.001 | 0.68 (0.58–0.81) | < 0.001 |
| XLPE | 853 | 34,537 | 1.6 (1.5–1.8) | 28,039 | 2. 9(2.7–3.1) | 10,514 | 3.8 (3.5–4.2) | 1,658 | |||||
| Lateral approach | |||||||||||||
| AOXLPE | 94 | 4,192 | 1.7 (1.3–2.2) | 3,377 | 2.6 (2.1–3.2) | 1,090 | 3.0 (2.3–3.9) | 139 | E.P. | 0.85 (0.69–.05) | 0.1 | 0.84 (0.68–1.04) | 0.1 |
| XLPE | 839 | 27,430 | 1.9 (1.7–2.0) | 24,551 | 3,2 (3.0–3.4) | 13,665 | 3.8 (3.5–4.1) | 3,001 | |||||
| Posterior approach | |||||||||||||
| AOXLPE | 514 | 21,380 | 1.9 (1.7–2.1) | 16035 | 3.1 (2.8–3.4) | 3537 | 3.3 ( 3.0–3.7) | 327 | E.P. | 1.07 (0.97–1.18) | 0.2 | 1.03 (0.94–1.14) | 0.5 |
| XLPE | 2,635 | 100,797 | 1.7 (1.7–1.8) | 85,950 | 2.9 (2.8–3.0) | 37,422 | 3.6 (3.5–3.8) | 6,462 | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments
Total hip replacement (THR) is a successful treatment for severe osteoarthritis [1], and survivorship has improved since highly cross-linked polyethylene (XLPE) was introduced [2,3]. However, cross-linking by irradiation creates free radicals that can remain in the material [4] and cause oxidative degeneration of polyethylene [5]. Thermal treatments to improve oxidative stability lower mechanical strength [4]. Adding antioxidant to polyethylene (AOXLPE) may mitigate oxidation without lowering the mechanical properties [4], and also decrease oxidation-induced inflammatory response in the periprosthetic tissues [6]. Despite the theoretical advantages of AOXLPE, the clinical benefit is unclear.
Radiographic studies comparing XLPE with and without antioxidant have shown lower femoral head penetration measured at 5–7 years, but no difference has been found for revision rates or patient outcome scores [7-9]. Meta-analyses have revealed similar femoral head penetration findings when comparing AOXLPE with either “standard” polyethylene (ultra-high molecular weight polyethylene-UHMWPE) or XLPE, but all-cause revision has less frequently been studied and the results have been mixed [10-12]. It is suggested that larger studies with longer follow-up are required to show potential differences [5,12].
The aim of this study was to compare the revision rates of THR using cementless acetabular components where the insert was made of either AOXLPE or XLPE, using data from a large national registry.
Methods
Study design
We used data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). The AOANJRR commenced data collection on September 1, 1999, achieving complete national implementation by mid-2002. The registry obtains an almost complete dataset (98.8%) of hip, knee, and shoulder replacement performed in Australia [13]. AOANJRR data is externally validated against patient-level data provided by all Australian state and territory health departments. Data is also matched bi-annually with the Australian Government’s National Death Index (NDI) to obtain information on the date of death. The study was conducted using the STROBE (Strengthening Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Participants
The population for this study consisted of all primary THR procedures over the 10-year period from 1 January 2014 until the end of December 2023. All-polyethylene cups and non-modular components were excluded. We included THRs with the initial diagnosis of osteoarthritis, with cementless acetabular shells, mixed ceramic or metal femoral heads, and only “modern” components, defined as those that were used in Australia in 2023. Dual mobility and constrained inserts were excluded.
Exposure
The exposure of interest was the material of the acetabular insert. Acetabular inserts made of AOXLPE were compared with inserts made of XLPE. AOXLPE included XLPE with antioxidant (commonly Vitamin E) added either by blending or diffusion. XLPE was defined as UHMWPE irradiated by high dose (≥50 kGy) gamma or electron beam radiation. Figure 1 displays a flow diagram showing inclusions/exclusions.
Patient flow diagram.
Outcome
The outcome measured was the cumulative percentage revision (CPR) for any reason. CPR was calculated for THR using AOXLPE or XLPE by the Kaplan–Meier method. Cox proportional hazards models were used to compare revision rates, with the assumption of proportional hazards checked by testing for a significant interaction between each covariate and the log of time. Rates and ratios are reported with 95% confidence intervals (CI). The 2 groups were additionally compared adjusting for age, sex, head size, head material, femoral fixation and surgical approach.
Statistics
The registry achieves an almost complete capture of hip, knee, and shoulder replacement procedures in Australia—98.8% completeness [13]. Consequently, approximately 1.2% of procedures (both primary and revisions) are not recorded. Of these missing joint replacement procedures, a small proportion 0.03% (i.e., ~2.5% of 1.2%) are expected to be revision procedures rather than primary procedures. This equates to approximately 59 missing revisions procedures (50 XLPE and 9 AOXLPE) from the current data set. These missing procedures are likely to be missing completely at random (MCAR) and given their small proportion and the survival analysis approach used, this is expected to have a negligible impact on the validity or precision of the study’s findings.
As collection of surgical approach information began in 2015, surgical approach for the first year of the study period was missing (for 19,018 procedures). The unadjusted and adjusted analyses were conducted excluding procedures with unknown surgical approach so that these analyses were comparable (i.e., complete case analyses were undertaken).
Comparisons were made between the 2 groups for revisions for loosening, revisions for “wear-related causes” (which included loosening, insert wear, osteolysis, and breakage of acetabular insert), revisions for fracture, revisions for infection, and revisions for dislocation. Sub-analyses were carried out stratifying by age group, femoral head size and type, femoral fixation, and surgical approach. Statistical analysis was performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Ethics, data sharing plan, funding, use of AI, and disclosures
The AOANJRR is approved by the Commonwealth of Australia as a federal quality assurance activity under section 124X of the Health Insurance Act, 1973. All AOANJRR studies are conducted in accordance with ethical principles of research (the Helsinki Declaration II). Registration was not required. No study funding was received. The AOANJRR is funded by the Australian Federal Government Department of Health and Aged Care. AI tools were not used.
The authors declare no potential conflicts of interest. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.45181
Results
There were 469,012 eligible THR with either XLPE or AOXLPE inserts. After exclusions for diagnoses other than osteoarthritis, procedures prior to 2014, or those that used either cemented acetabular components, ceramicized metal heads, non-modular, constrained, or dual mobility designs, and those with an unknown surgical approach, there were 198,073 THR procedures with 35,309 AOXLPE and 162,764 XLPE inserts included in the study (see Figure 1). There were 769 and 4,327 revisions of THR with AOXLPE and XLPE inserts respectively. Demographic and prosthesis factors are summarized in Table 1. While mean ages, sex distribution, and BMI were similar for the 2 groups, there were inequalities in prosthesis factors. The AOXLPE group had a higher proportion with ceramic heads (77% vs 52%), head size > 32 mm (81% vs 49%), and cementless femoral components (81% vs 56%).
AOXLPE use increased to 30% of hip procedures in 2023, with shorter median follow-up for this group. The acetabular components which used AOXLPE or XLPE inserts are indicated in Appendix Table 1A.
The reasons for revision for the 2 groups are presented in Table 2 while Table 3 lists the revision procedures.
Outcome
There was no early difference between the 2 groups in the rate of all-cause revision but after 3 years THR using AOXLPE inserts had a lower revision rate than THR using XLPE (Figure 2). The unadjusted and adjusted comparisons (adjusting for age, sex, head size, head material, femoral fixation, and surgical approach) were similar, with the unadjusted HR becoming significant after 3 years (HR 0.64, CI 0.48–0.84) P = 0.002 as did the adjusted HR 0.63 (CI 0.47–0.83) P = 0.001 (Table 4).
Cumulative percentage revision of primary total hip replacement by bearing surface.
Further analyses showed that there were lower rates of revision for loosening (after 2 years), wear-related causes (also after 2 years), and fracture for THR with AOXLPE inserts. There were no differences when comparing the groups for revisions for dislocation/instability or revisions for infection (Table 5).
In sub-analyses that compared AOXLPE with XLPE inserts by prosthesis factors, a higher revision rate was found for the AOXLPE group with femoral head sizes ≤ 32 mm, while a lower revision rate was seen with AOXLPE for head size > 32mm after 1.5 years. Procedures using ceramic femoral heads had a lower revision rate with AOXLPE than with XLPE inserts, while metal femoral heads used with AOXLPE inserts had a higher revision rate until 3 months when compared with XLPE. Cemented femoral fixation was associated with a higher revision rate with AOXLPE inserts, while cementless femoral fixation had a lower revision rate with AOXLPE inserts. The anterior surgical approach had a lower revision rate using AOXLPE inserts, but there were no between-group differences with the lateral or posterior approaches (Table 6).
Sensitivity analysis
As data for surgical approach was incomplete, a sensitivity analysis was conducted in which those procedures with unknown surgical approaches formed another categorical level. The results of these analyses were similar to the analyses that excluded those with unknown surgical approach (Appendix Table 2A). There were no material changes in significance or HR that would affect the interpretation of the results.
Discussion
We aimed to compare the revision rates of THR using cementless acetabular components where the insert was made of either XLPE or AOXLPE, using data from AOANJRR.
We found that THR using AOXLPE acetabular inserts had a lower all-cause revision rate than XLPE inserts after 3 years. This was consistent for both the crude and multiply adjusted comparisons. Not only does AOXLPE appear to be safe to use, but this finding gives indirect support to the concept that antioxidant may improve the wear-resistance of XLPE.
Revisions for loosening, wear-related causes, and fracture were lower with AOXLPE inserts. While early loosening may be due to a failure to gain initial fixation, revisions for late loosening, as well as wear-related causes and fracture, may be consequences of polyethylene wear and osteolysis. In addition, procedures using larger diameter and ceramic femoral heads, cementless femoral fixation, and the anterior surgical approach showed lower revision rates with AOXLPE. These prosthesis and technique features are commonly selected for higher demand patients, where wear-related performance differences can be more readily detected.
While we found differences in revision rates, with many favoring AOXLPE, these findings were not universal, and the magnitude of difference was often small. Additionally, the analyses of cemented femoral stems and procedures using metal femoral heads showed lower revision rates with XLPE inserts. Selection of lower cost options (such as XLPE, cemented femoral fixation, and metal heads) are more common for older, less active patients, where revisions are more likely due to non-wear-related reasons. This indicates the differences found in overall revision may not be totally due to the insert but, in part, to the femoral or acetabular components used as well.
Previous comparisons of AOXLPE and XLPE have been conflicting, with some revealing promising in vivo wear results for AOXLPE [6,14] measured by femoral head penetration [8,15], while others have shown no difference in overall migration [7] or migration after the bedding-in period [16]. Our results contrast with previous clinical trials. A multicenter study comparing 520 hips with AOXLPE inserts with 457 hips with XLPE showed similar revision rates at 7 years [9], while another comparing AOXLPE monoblock cups with a similar cup of UHMWPE found a 98% 6-year survival for both groups [15]. These studies were designed to compare polyethylene wear, but both were underpowered regarding revision rates. Two meta-analyses that reported THR revision results revealed no difference between AOXLPE and XLPE [17,18], while another showed AOXLPE liners lowered the revision risk at 5–7 years, but this finding was disproportionately influenced by a single study [12].
Registry studies have discerned a difference in revision rate when comparing XLPE with UHMWPE [2,19,20], but have provided limited evidence regarding AOXLPE.
Our findings differ from a Finnish registry study, which found 94% survival of hips using AOXLPE at 7 years, while their moderately cross-linked comparison group was comparable at 93% [21]. Their 2 groups also had similar survivorship when analyzed for wear-related reasons for revision. Kjaergaard et al. compared polyethylene inserts in Demark, finding fewer polyethylene-related revisions for THR using AOXLPE but a higher all-cause revision rate for the first 3 months, largely for femoral loosening and periprosthetic fracture and attributed this to the femoral components used [22]. Compared with our study, these studies had shorter follow-up, smaller study populations and were both restricted to products from a single manufacturer with limited choices of femoral and acetabular components. While restricting inserts may have been intended to limit confounding, it reduces the ability to generalize findings for entire groups.
Strengths
The strengths of our study are the large patient cohort, inclusion of all variants of the 2 polyethylene types, used with contemporary components, with medium-term follow-up of the protheses of interest, and analyses adjusting for possible confounding factors, when used in a community setting.
Limitations
We have used all-cause revision as the outcome measure, and there are some reasons for revision that are unrelated to the type of polyethylene used. Sub-analyses were consequently performed selecting specific reasons for revision that have a closer relationship to polyethylene wear. Unfortunately, we had too few procedures for prosthesis-specific analyses. Additionally, we have grouped the acetabular inserts into 2 polyethylene categories, and there may be performance differences within each group. Furthermore, the median follow-up duration for the AOXLPE group (2.6 years) was shorter than for the XLPE group (4.3 years) and it is likely that wear-related differences may become more evident with longer follow-up.
Conclusion
While there was no early difference, THR with AOXLPE acetabular inserts had a lower revision rate after 3 years than THR with XLPE. This suggests a possible clinical benefit using AOXLPE but the difference may, in part, be related to the associated femoral or acetabular components.
Supplementary data
Supplementary Tables 1–2 and a DAG are available on the article page, doi: 10.2340/17453674.2025.45181
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Learmonth I D, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet 2007; 370: 1508-19. doi: 10.1016/S 0140-6736(07)60457-7.17964352 · doi ↗ · pubmed ↗
- 2de Steiger R, Lorimer M, Graves S E. Cross-linked polyethylene for total hip arthroplasty markedly reduces revision surgery at 16 years. J Bone Joint Surg Am 2018; 100: 1281-8. doi: 10.2106/jbjs.17.01221.30063590 · doi ↗ · pubmed ↗
- 3Shen C, Tang Z H, Hu J Z, Zou G Y, Xiao R C, Yan D X. Does cross-linked polyethylene decrease the revision rate of total hip arthroplasty compared with conventional polyethylene? A meta-analysis. Orthop Traumatol Surg Res 2014; 100: 745-50. doi: 10.1016/j.otsr.2014.07.015.25281549 · doi ↗ · pubmed ↗
- 4Spece H, Yarbrough R V, Kurtz S M. In vivo performance of vitamin E stabilized polyethylene implants for total hip arthroplasty: a review. J Arthroplasty 2023; 38: 970-9. doi: 10.1016/j.arth.2022.11.010.36481286 · doi ↗ · pubmed ↗
- 5Lambert B, Neut D, van der Veen H C, Bulstra S K. Effects of vitamin E incorporation in polyethylene on oxidative degradation, wear rates, immune response, and infections in total joint arthroplasty: a review of the current literature. Int Orthop 2019; 43: 1549-57. doi: 10.1007/s 00264-018-4237-8.30470866 · doi ↗ · pubmed ↗
- 6Massaccesi L, Ragone V, Papini N, Goi G, Corsi Romanelli M M, Galliera E. Effects of vitamin E-stabilized ultra high molecular weight polyethylene on oxidative stress response and osteoimmunological response in human osteoblast. Front Endocrinol (Lausanne) 2019; 10: 203. doi: 10.3389/fendo.2019.00203.31001202 PMC 6457167 · doi ↗ · pubmed ↗
- 7Kjaergaard K, Ding M, Jensen C, Bragdon C, Malchau H, Andreasen C M, et al. Vitamin E-doped total hip arthroplasty liners show similar head penetration to highly cross-linked polyethylene at five years: a multi-arm randomized controlled trial. Bone Joint J 2020; 102-B: 1303-1310. doi: 10.1302/0301-620X.102B 10.BJJ-2020-0138.R 1.32993343 PMC 7517722 · doi ↗ · pubmed ↗
- 8Busch A, Jager M, Klebingat S, Baghdadi J, Florkemeier T, Hutter F, et al. Vitamin E-blended highly cross-linked polyethylene liners in total hip arthroplasty: a randomized, multicenter trial using virtual CAD-based wear analysis at 5-year follow-up. Arch Orthop Trauma Surg 2020; 140: 1859-66. doi: 10.1007/s 00402-020-03358-x.32048017 · doi ↗ · pubmed ↗