Routine jejunostomy feeding after esophagectomy reduces early weight loss: a cohort study
Jessica Yan-Seen Ng, Catherine Jenn Yi Cheang, Alexander W. Phillips

TL;DR
Using jejunostomy feeding after esophagectomy helps reduce early weight loss, especially in patients who had chemotherapy.
Contribution
The study shows that routine jejunostomy feeding significantly reduces early weight loss after esophagectomy.
Findings
Jejunostomy-fed patients had significantly less weight loss at 2, 6, and 12 weeks postoperatively.
Patients who had neoadjuvant chemotherapy showed the most benefit from jejunostomy feeding at 3 months.
Median hospital stay was shorter for patients with jejunostomy feeding.
Abstract
Jejunostomy feeding tubes are commonly used during esophagectomy to provide postoperative nutritional support, but their impact on clinical outcomes remains uncertain. This retrospective study included 507 patients who underwent esophagectomy for esophageal cancer at the Northern Oesophagogastric Unit between 2012 and 2014 and 2016–2019. Routine postoperative jejunostomy feeding was introduced in 2015. Outcomes measured were percentage weight change at 2, 6, 12, and 24 weeks postoperatively, length of hospital stay, weight loss in patients with major complications (Clavien-Dindo > 3), and long-term survival. Of the 507 patients, 290 received routine jejunostomy feeding and 217 did not. Jejunostomy-fed patients experienced significantly less weight loss at all measured time points, with weight loss at 2 weeks of 3.22% versus 7.24% (p < 0.001), at 6 weeks of 3.28% versus 8.30% (p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
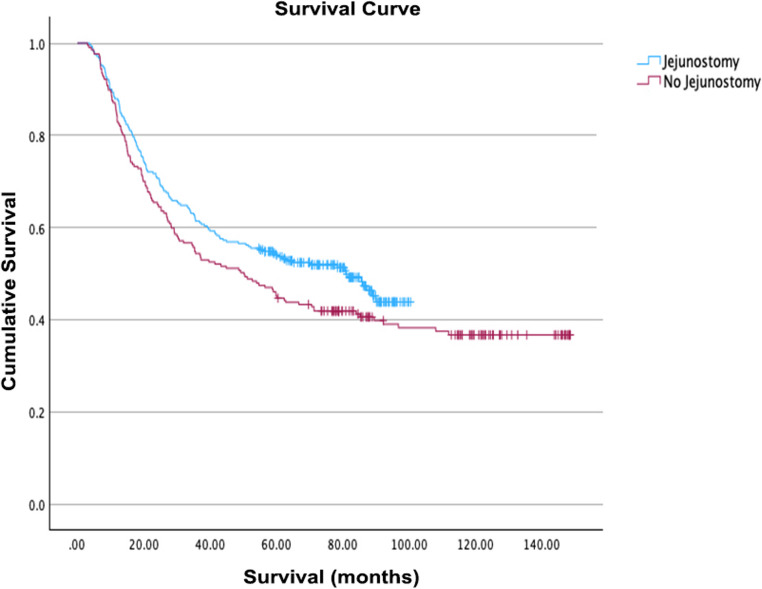 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Enhanced Recovery After Surgery · Esophageal and GI Pathology
Introduction
Esophageal cancer treatment primarily involves surgical resection, often combined with neoadjuvant therapy, particularly in advanced stages. During esophagectomy, jejunostomy feeding tubes are frequently inserted to provide early postoperative nutritional support. While these tubes are intended to maintain nutrition and mitigate the effects of complications, their use may also be associated with increased morbidity.
Evidence suggests that early nutritional support through jejunostomy feeding can enhance recovery following major abdominal surgery [1]. Despite tailored dietary plans, patients commonly experience poor nutrition postoperatively, highlighting the need for additional supplementary feeding methods [2]. Home enteral nutrition via jejunostomy has been shown to enhance nutritional status, reduce fatigue, and lower the risk of postoperative pneumonia, contributing to overall improvements in quality of life for patients recovering from esophagectomy [3]. Many patients present with significant weight loss and malnutrition both at diagnosis and after treatment, and maintaining adequate nutrition is essential in reducing the risk of postoperative complications, lowering reoperation rates, and improving long-term survival.
Malnutrition negatively impacts treatment outcomes for patients with esophageal cancer after esophagectomy and is often worsened by chemotherapy and radiotherapy [4]. Consequently, strategies to ensure adequate nutritional intake are crucial. Jejunostomy feeding can provide a reliable means of nutrition, particularly for patients who develop postoperative complications, thereby helping to reduce the risk of complications and promote recovery [5].
This study evaluates the impact of routine postoperative jejunostomy feeding on weight loss in patients who have undergone esophagectomy, aiming to determine its effectiveness in mitigating the nutritional challenges faced during recovery.
Method and materials
Patient population
A retrospective review of patients who underwent esophagectomy for esophageal cancer between January 2012 to December 2014 and January 2016 to December 2019 at the Northern Oesophagogastric Unit, Newcastle Upon Tyne was performed. The year 2015 was excluded as a transition period when routine jejunostomy feeding was being introduced, to avoid bias and ensure clear comparison between cohorts. Routine post-operative feeding via jejunostomy, including overnight feeding upon discharge, was introduced in 2015; since then, all patients undergoing esophagectomy have received a jejunostomy feeding tube as part of standard care. All patients had a feeding jejunostomy placed prior to 2015; however, these tubes were not routinely used for discharge feeding but were intended as a precautionary measure in case patients experienced difficulties during adjuvant chemotherapy. We sought to investigate long term outcomes through review of electronic medical records and an existing patient database.
Staging and treatment
Initial staging comprised of endoscopy with biopsy, endoscopic ultrasonography, and positron emission tomography scans. Neoadjuvant therapy followed by esophagectomy was indicated for patients with histologically proven, advanced, resectable malignancy without distant metastases (cT1, N1-3, M0 or cT2-3, N0-3, M0) and/or those with tumors of questionable resectability (cT4). The types of esophagectomy performed during the study periods (2012–2014 and 2016–2019) included two-stage (Ivor Lewis) and three-stage (McKeown) procedures, both with stapled anastomoses. Feeding jejunostomy was placed approximately 20–30 cm distal to the duodenojejunal flexure using a Witzel tunnel technique. Omentopexy was performed to secure the jejunostomy to the abdominal [6]. There were no significant differences in patient selection criteria or variations in nutritional support protocols beyond the use of jejunostomy feeding during these time periods. Patients with metastatic disease, non-resectable tumors at exploratory surgery were excluded. Patients with T2N0 disease or earlier received surgery alone unless otherwise indicated. Patients with early disease amenable to endoscopic mucosal resection were excluded.
Neoadjuvant therapies and operative treatment
Multiple neoadjuvant regimens were employed based on the standard of care and available clinical trials at the time of treatment. The majority of patients received epirubicin, cisplatin, and either fluorouracil or capecitabine (ECF/ECX - MAGIC regimen). FLOT (Fluorouracil, Leucovorin, Oxaliplatin, and Docetaxel) was increasingly used as a neoadjuvant regimen after 2017. Esophagectomy was performed within 8 weeks after completion of neoadjuvant therapy using a conventional approach.
Outcomes
Primary outcomes measured included percentage weight change at 2 weeks, 6 weeks, 3 months, and 6 months compared to initial weight at diagnosis, with subgroup analyses based on different types of multimodal cancer therapy used. Secondary outcomes investigated included length of hospital stay, weight loss in patients with complications greater than Clavien-Dindo 3, and long-term survival duration.
Follow-up and definition of recurrence
All patients were followed up at outpatient clinics at 3- to 6-month intervals for the first 2 years, then every 6 months to annually up until 5 years. Recurrence was diagnosed based on clinical suspicion and confirmed with either CT imaging or endoscopy.
Statistical analysis
Continuous variables were compared using t-tests for equality of means. Categorical variables were compared using Fisher’s exact test. A P-value of < 0.05 was considered statistically significant. Analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY).
Results
Patient characteristics
This study included 507 patients who underwent esophagectomy for cancer between January 2012 and December 2014, and January 2016 and December 2019 at the Northern Oesophagogastric Unit, Newcastle Upon Tyne. Of these, 290 patients received routine postoperative feeding through a jejunostomy, which was introduced in 2015, while the remaining 217 patients did not receive routine jejunostomy feeding. Patient characteristics are summarized in Table 1.
Table 1. Patient demographicsNo Jejunostomy (n) = 217With jejunostomy (n) = 290Significance (p)Age at surgery64.6 ± 9.865.6 ± 8.50.247Male Gender (%)74.2 (161/217)76.2 (221/290)0.603 (Pearson’s chi)Ivor Lewis (%)96.3 (209/217)91.7 (266/290)McKeown (%)3.7 (8/217)8.3 (24/290) Co-morbidities (n) Cardiac disease921370.281(Fishers)Respiratory disease39470.633(Fishers)Diabetes Mellitus22460.066(Fishers)Renal disease12120.528 (Fishers)Liver disease221.000 (Fishers) Treatment combination (n) NAC* + Surgery + AC33530.166 (Pearson Chi)NAC* + Surgery110118Surgery + AC24Surgery only72115 Histology (n) Adenocarcinoma1602140.148 (Pearson chi)Adenosquamous33Squamous cell carcinoma4467High grade dysplasia75Others30 Site of cancer (n) Upper esophagus260.043 (Pearson chi)Middle esophagus2857Lower esophagus150166Gastro-esophageal junction3659 T stage (n) T06250.006 (Pearson chi)T14481T23642T3110128T41611 N Stage (n) N01031520.611 (Pearson chi)N15367N23840N32230**NAC* Neoadjuvant chemotherapy, **AC Adjuvant chemotherapy
Weight change post-surgery
Overall, patients who received jejunostomy feeding consistently demonstrated less weight loss compared to those without jejunostomy feeding across all time points and treatment groups. (Table 2) This difference was most pronounced in the first 6 months postoperatively (Tables 3 and 4).
Table 2(Results): primary outcomes: mean weight loss in kilogramsMean weight loss in kg (%) ± SEM* (n)Significance (P-value)No jejunostomy feedingWith jejunostomy feedingAll PatientsWeek 2 (kg)5.50 (7.24%) ± 0.28 (193)2.92 (3.22%) ± 0.22 (256)< 0.001Week 6 (kg)6.37 (8.30%) ± 0.33 (214)3.39 (3.28%) ± 0.25 (258)< 0.0013 Months (kg)7.96 (10.38%) ± 0.47 (172)4.81 (5.49%) ± 0.30 (258)< 0.0016 Months (kg)9.28 (11.46%) ± 0.49 (214)7.25 (6.89%) ± 0.53 (247)0.006NAC** + Surgery + ACWeek 2 (kg)5.55 (7.01%) ± 0.81 (24)3.05 (3.32%) ± 0.45 (54)0.005Week 6 (kg)6.01 (7.77%) ± 1.02 (26)3.38 (4.13%) ± 0.57 (54)0.0173 Months (kg)7.08 (8.81%) ± 1.69 (23)5.37 (5.23%) ± 0.72 (54)0.2726 Months (kg)9.14 (10.86%) ± 1.46 (28)6.29 (9.26%) ± 0.77 (53)0.060Surgery onlyWeek 2 (kg)5.00 (6.90%) ± 0.49 (73)3.07 (3.60%) ± 0.32 (97)< 0.001Week 6 (kg)5.80 (7.86%) ± 0.50 (77)3.31 (3.87%) ± 0.37 (98)< 0.0013 Months (kg)6.73 (9.45%) ± 0.62 (61)5.03 (5.69%) ± 0.44 (98)0.0246 Months (kg)8.72 (11.32%) ± 0.77 (78)7.00 (7.77%) ± 0.63 (94)0.084NAC + surgeryWeek 2 (kg)6.02 (7.70%) ± 0.36 (91)2.70 (3.32%) ± 0.40 (104)< 0.001Week 6 (kg)7.04 (8.88%) ± 0.48 (106)3.45 (4.13%) ± 0.42 (105)< 0.0013 Months (kg)9.25 (11.63%) ± 0.68 (84)4.32 (5.23%) ± 0.48 (105)< 0.0016 Months (kg)9.90 (11.81%) ± 0.72 (103)8.02 (9.26%) ± 1.12 (99)0.157**SEM Standard Error of Mean, **NAC Neoadjuvant chemotherapy, ***AC Adjuvant chemotherapy
Table 3. Secondary outcome measuresNo JejunostomyWith jejunostomySignificance (p)Length of stay (days)15 ± 11 (182)11 ± 9 (290)< 0.05All complications (including Clavien-Dindo < 3)66.5% (109/164)67.9% (230/339)0.75Clavien-Dindo classification of complications > 3 (%)26.1% (49 / 188)27.5% (128/475)0.75
Table 4. Numbers at riskTime (months)Jejunostomy (Number at Risk)No Jejunostomy (Number at Risk)0290217122782052426619336254181482421696023015772218145842061339619412110818210912017097140131126160135135180137133200138138
For the entire cohort, patients without jejunostomy feeding lost significantly more weight at all time points. At 2 weeks post-surgery, patients without jejunostomy lost 5.50 kg (7.24%) compared to 2.92 (3.22%) kg in those with jejunostomy (p < 0.001). This trend continued at 6 weeks (6.37 kg (8.30%) vs. 3.39 kg (3.28%), p < 0.001) and 3 months (7.96 kg (10.38%) vs. 4.81 kg (5.49%), p < 0.001). By 6 months, although the difference narrowed, it remained statistically significant (9.28 kg (11.46%) vs. 7.25 kg (6.89%), p = 0.006).
When analyzing subgroups based on treatment regimens, we observed varying patterns. In the neoadjuvant chemotherapy (NAC) with surgery and adjuvant chemotherapy (AC) group, significant differences in weight loss were observed at 2 weeks (5.55 kg (7.01%) vs. 3.05 kg (3.32%), p = 0.005) and 6 weeks (6.01 kg (7.77%) vs. 3.38 kg (4.13%), p = 0.017). However, by 3 months and 6 months, the differences were no longer statistically significant.
In the surgery-only group, significant differences in weight loss persisted up to 3 months post-surgery. At 2 weeks, patients without jejunostomy lost 5.00 kg (6.90%) compared to 3.07 kg (3.60%) in those with jejunostomy (p < 0.001). This difference remained significant at 6 weeks (5.80 kg (7.86%) vs. 3.31 kg (3.87%), p < 0.001) and 3 months (6.73 kg (9.45%) vs. 5.03 kg (5.69%), p = 0.024). By 6 months, the difference was no longer statistically significant (8.72 kg (11.32%) vs. 7.00 kg (7.77%), p = 0.084).
The NAC and surgery group demonstrated the most pronounced differences in weight loss. At 2 weeks, patients without jejunostomy lost 6.02 kg (7.70%) compared to 2.70 kg (3.32%) in those with jejunostomy (p < 0.001). This substantial difference persisted at 6 weeks (7.04 kg (8.88%) vs. 3.45 kg (4.13%), p < 0.001) and was most noticeable at 3 months, where patients without jejunostomy lost over twice as much weight (9.25 kg (11.63%) vs. 4.32 kg (5.23%), p < 0.001). However, by 6 months, the difference was no longer statistically significant (9.90 kg (11.81%) vs. 8.02 kg (9.26%), p = 0.157).
These results suggest that jejunostomy feeding is most effective in reducing weight loss in the early postoperative period, particularly within the first 3 months after surgery. The benefits appear to be most pronounced in patients receiving neoadjuvant chemotherapy. However, the impact of jejunostomy feeding on weight loss seems to diminish over time, with differences becoming non-significant by 6 months in most treatment groups.
A significantly higher proportion of patients in the jejunostomy group received adjuvant treatment compared to those without a jejunostomy (21.2% vs. 12.4%), suggesting that jejunostomy placement may be associated with increased uptake of adjuvant chemotherapy.
Length of hospital stay
Median length of stay for patients who received jejunostomy feeding was significantly shorter (11 days ± 9), compared to those who did not receive jejunostomy feeding (15 days ± 11), p = 0.05.
Weight loss in patients with complications greater than Clavien-Dindo 3
There was no significant difference in weight loss in patients who experienced severe complications based on the Dindo severity grading system.
Long-term survival duration
Long-term survival outcomes after esophagectomy were compared between patients who received routine postoperative jejunostomy feeding and those who did not, using Kaplan-Meier analysis. The survival curves demonstrate a visible separation in favor of the jejunostomy group (Fig. 1). Median survival was higher in the jejunostomy group (81.1 months, 95% CI: 62.4–99.8) compared to the non-jejunostomy group (50.2 months, 95% CI: 34.6–65.8). However, the difference did not reach statistical significance by the log-rank test (χ² = 2.82, p = 0.093), indicating that the observed difference may represent a trend rather than a definitive survival benefit within this cohort.
Fig. 1. Kaplan Meier survival curve
Discussion
The results of this study show that jejunostomy feeding offers significant benefits in the short term, particularly in reducing weight loss in the early postoperative period. However, the long-term effects of jejunostomy feeding on clinical outcomes such as survival and functional recovery require further investigation. Moreover, additional research is needed to identify patient populations that would benefit most from routine jejunostomy placement, ensuring that its use provides optimal nutritional support while minimizing potential complications.
The use of jejunostomy feeding tubes after esophagectomy remains a subject of ongoing debate. While jejunostomy placement offers a reliable route for postoperative nutritional support, it is not without its complications. Previous studies have documented several jejunostomy-related issues, including bowel obstruction [7, 8] infections at the insertion site, ileus, and frequent emergency room visits [5, 9]. A recent meta-analysis of 12 studies found that routine jejunostomy placement was associated with longer operating times [10, 11] and higher rates of morbidity and wound infection [12]. Furthermore, jejunostomy feeding does not consistently prevent weight loss in the long term, nor does it uniformly improve nutritional status compared to oral feeding [1, 8].
Despite these challenges, evidence suggests that jejunostomy feeding may lower 30-day mortality without significantly influencing other common postoperative complications [11]. Additionally, routine jejunostomy placement can improve short-term nutritional outcomes and may be associated with better long-term survival [10]. However, there remains conflicting evidence, with some studies reporting no significant differences in clinical outcomes such as anastomotic leak rates, protein levels, or the need for further nutritional interventions [13, 14].
Postoperative weight loss following esophagectomy is clinically significant because it is linked to poorer nutritional status, decreased tolerance to adjuvant therapies, and reduced overall survival, especially in patients with advanced disease. Kubo et al. showed that patients who lost 12% or more of their body weight six months after surgery experienced significantly worse survival outcomes, highlighting the importance of strategies to minimize weight loss in this population [15]. Additionally, malabsorption commonly occurs after esophagectomy, further contributing to nutritional deficiencies and weight loss [16]. This underscores the value of enteral feeding via jejunostomy, which may help mitigate malabsorption by ensuring adequate nutrient delivery in the early postoperative period. The percentage of weight loss observed in our study is consistent with the ranges reported in the literature. Prior studies have described a mean weight loss of 11.7% at six months post-esophagectomy, with up to 62.9% of patients experiencing >10% unintentional weight loss, and some subgroups, losing as much as 16.2% of their preoperative weight. Another prospective cohort study reported an average 8% weight loss at six months, with 20% of patients losing more than 15% [17]. In our cohort, patients without jejunostomy feeding lost between 10.38% and 11.81% of their body weight by six months, while those with jejunostomy feeding generally lost less (6.89% to 9.26%). Our findings indicate that patients who received jejunostomy feeding consistently demonstrated less weight loss across all time points, particularly in the early postoperative period (up to 3 months). This effect was especially pronounced in patients undergoing neoadjuvant chemotherapy in combination with surgery, reinforcing the importance of jejunostomy feeding in reducing early postoperative weight loss. Furthermore, routine jejunostomy feeding was associated with a significantly shorter length of hospital stay, although no significant difference was observed in the occurrence of severe complications.
Achieving adequate nutritional status is particularly relevant for patients who require adjuvant chemotherapy following neoadjuvant therapy and esophagectomy, as this approach has been associated with improved survival, even in node-negative and margin-negative disease [18]. Since malnutrition can delay or prevent patients from receiving adjuvant therapy, routine use of jejunostomy feeding may play a crucial role in optimizing postoperative recovery and ensuring patients can proceed with further oncological treatment.
A higher proportion of patients in the jejunostomy group received adjuvant treatment compared to those without a jejunostomy (21.2% vs. 12.4%), suggesting a potential association between jejunostomy placement and greater uptake of adjuvant chemotherapy. While this may reflect an additional benefit beyond nutritional support, the retrospective nature of the study limits interpretation. Confounding factors such as differences in chemotherapy regimens, comorbidities, treatment tolerance, patient preference, social support, health literacy, and time to recovery may have influenced access to or suitability for adjuvant treatment independently of jejunostomy use.
Due to the retrospective design and limitations in data retrieval, a detailed assessment of jejunostomy-related complications was not feasible. A limitation of this study is the introduction of bias due to the simultaneous introduction of routine jejunostomy feeding and the adoption of chemotherapy regimens. Additionally, this study compares two non-concurrent cohorts from different time periods (2012–2014 and 2016–2019), introducing temporal bias that may further confound the observed outcomes. Since the two changes occurred concurrently, it is difficult to entirely separate the effects of the feeding protocol from the potential impact of neoadjuvant chemotherapy on postoperative recovery and nutritional status. The potential confounding effect of neoadjuvant chemotherapy on the observed outcomes as well as evolving surgical techniques should therefore be considered when interpreting the results. Enhanced recovery after surgery protocols were introduced in 2016, and these have been shown to improve both short and long term outcomes. Such changes in discharge criteria, hospital policies, and postoperative care pathways may have independently impacted the outcomes observed and represent potential confounding factors not fully controlled for in this retrospective analysis [19]. Future studies with a more controlled design and clearer distinction between the effects of nutritional support and chemotherapy could provide further insight into the specific role of jejunostomy feeding.
Previous research has emphasized the importance of implementing perioperative pathways to optimize patient recovery and reduce the risk of complications [20]. In this study, we sought to determine whether the routine use of jejunostomy feeding could contribute to reducing the effects of postoperative complications by improving nutritional status and minimizing excessive weight loss. Additionally, it is important to note that we do not have data on functional improvement or quality of life (QoL) in our cohort. Recent research by Jia et al. highlights that esophageal cancer survivors who experience greater weight loss and higher symptom distress tend to have significantly worse QoL, underscoring the clinical importance of minimizing postoperative weight loss to improve patient-centered outcomes [21]. While our findings suggest that early enteral feeding may be a valuable component of perioperative care, we did not observe a significant difference in the incidence of severe complications between patients with or without jejunostomy feeding.
Conclusion
This study underscores the significant role of routine jejunostomy feeding in reducing short-term weight loss after esophagectomy. Jejunostomy feeding is associated with improved early postoperative nutrition and a reduced length of hospital stay, offering valuable support to patients during their recovery. However, the long-term clinical benefits, including its impact on survival, long-term nutritional status, and functional recovery, remain unclear and warrant further research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koterazawa Y, Oshikiri T, Hasegawa H, Yamamoto M, Kanaji S, Yamashita K et al (2020) Routine placement of feeding jejunostomy tube during esophagectomy increases postoperative complications and does not improve postoperative malnutrition. Dis Esophagus 33. 10.1093/dote/doz 02110.1093/dote/doz 02130997494 · doi ↗ · pubmed ↗
- 2Al-Temimi MH, Dyurgerova AM, Kidon M, Johna S (2019) Feeding jejunostomy tube placed during esophagectomy: is there an effect on postoperative outcomes? Perm J 23. 10.7812/TPP/18.21010.7812/TPP/18.210PMC 673096031496496 · doi ↗ · pubmed ↗