Double Agglutination Observed in Mycoplasma-Associated Kawasaki Disease: Pathophysiological Insights and Considerations for Treatment Strategy
Megumi Akutsu, Daisuke Matsubara, Kazuo Takahashi, Mitsuru Seki, Kazuhiko Kotani

TL;DR
A rare case of Kawasaki disease linked to Mycoplasma infection shows both red blood cell and neutrophil agglutination, offering insights into diagnosis and treatment.
Contribution
This case highlights the rare occurrence of neutrophil agglutination in Mycoplasma-associated Kawasaki disease and its diagnostic challenges.
Findings
Neutrophil agglutination resolved within a week, while erythrocyte agglutination lasted four weeks.
Erythrocyte agglutination may help diagnose Mycoplasma infection, but neutrophil agglutination is rare and challenging to detect in children.
Abstract
We describe a rare pediatric case of Mycoplasma-associated Kawasaki disease, accompanied by secondary cold agglutinin disease, characterized by both erythrocyte and neutrophil agglutination. In this case, neutrophil agglutination resolved within one week, while erythrocyte agglutination persisted for four weeks, paralleling the decline in Mycoplasma antibody titers and suggesting possible differences in their agglutination thresholds. Erythrocyte agglutination through secondary cold agglutinin disease sometimes facilitates the concomitant diagnosis of Mycoplasma infection. On the other hand, neutrophil agglutination is rare, particularly in children, which poses a diagnostic challenge. This case also highlights potential diagnostic considerations and management challenges when Kawasaki disease occurs in the setting of Mycoplasma infection. A brief discussion of clinical implications and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
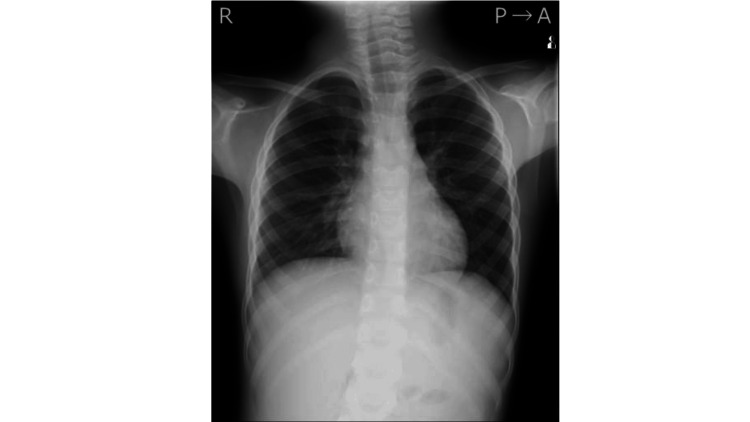 Figure 1
Figure 1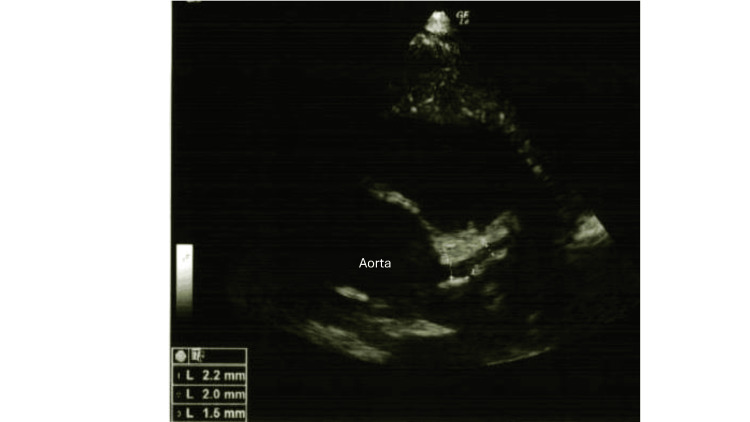 Figure 2
Figure 2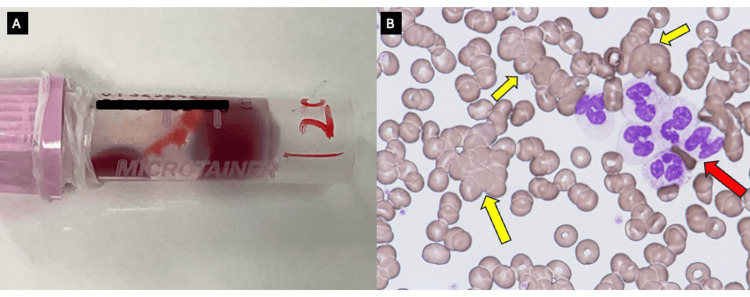 Figure 3
Figure 3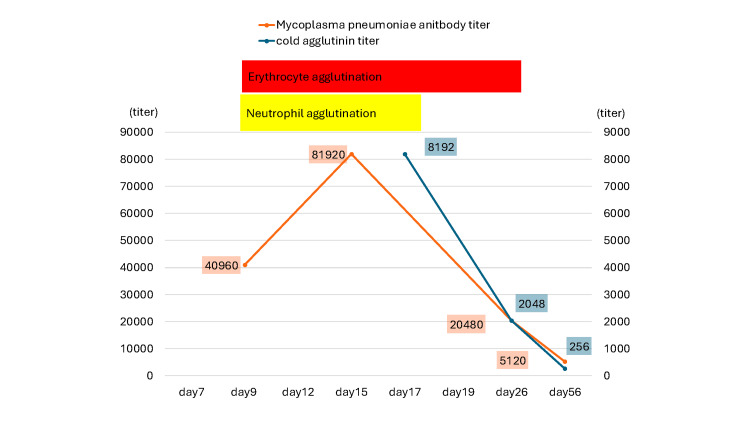 Figure 4
Figure 4| Parameter | Value | Reference Range |
| White blood cell count (×103/μL) | 5.9 | 3.3–8.6 |
| Neutrophils (%) | 65.3 | 42–74 |
| Hemoglobin (g/dL) | 13.1 | 13.7–16.8 |
| Platelet count (×104/μL) | 20.7 | 15.8–34.8 |
| D-dimer (μg/mL) | 0.5 | 0–1.0 |
| C-reactive protein (mg/dL) | 2.95 | 0–0.14 |
| Albumin (g/dL) | 3.2 | 4.1–5.1 |
| Total bilirubin (g/dL) | 0.2 | 0.4–1.5 |
| Aspartate aminotransferase (U/L) | 31 | 13–30 |
| Alanine aminotransferase (U/L) | 18 | 10–42 |
| Lactate dehydrogenase (U/L) | 427 | 124–222 |
| Creatine phosphokinase (U/L) | 37 | 59–248 |
| Blood urea nitrogen (mg/dL) | 7.8 | 8–20 |
| Creatinine (mg/dL) | 0.28 | 0.65–1.07 |
| High-density lipoprotein cholesterol (mg/dL) | 24 | 38–90 |
| Sodium (mmol/L) | 136 | 138–145 |
| Potassium (mmol/L) | 3.5 | 3.6–4.8 |
| Chloride (mmol/L) | 102 | 101–108 |
| Antinuclear antibody (titer) | <40 | 0–40 |
| Complement activity (CH50/mL) | 25.1 | 25–48 |
| C3 (mg/dL) | 123 | 73–138 |
| C4 (mg/dL) | 10 | 11–31 |
| Myeloperoxidase anti-neutrophil cytoplasmic antibody (U/mL) | <1.0 | 0–3.5 |
| Proteinase-3 anti-neutrophil cytoplasmic antibody (U/mL) | 1.4 | 0–3.5 |
| Case | Age / Sex | Comorbidity | Treatment | Neutrophil agglutination | Erythrocyte agglutination | Other leukocyte agglutination | Duration of neutrophil agglutination | Duration of erythrocyte agglutination | Cold agglutinin titer | Mycoplasma pneumonia antibody titer | Reference |
| 1 | 8 y / M | MP | Antibiotic (+) | (+) | Unknown | (-) | Days 13–21 | Unknown | >1:1024 | >1:40,960 | 6 |
| 2 | 7 y / M | MP | Antibiotic (+) | (+) | Unknown | (-) | Days 10–14 | Unknown | >1:512 | >1:40,960 | 6 |
| 3 | 6 y / F | MP | Antibiotic (+) | (+) | Unknown | (-) | Days 12–14 | Unknown | >1:512 | >1:10,280 | 6 |
| 4 | 7 y / M | MP | Antibiotic (+) | (+) | Unknown | Eosinophil | Days 15–32 | Unknown | >1:512 | >1:40,960 | 6 |
| 5 | 13 y / F | MP + HSV | Antibiotic (+) (erythromycin) | (+) | Unknown | (-) | Days 15–5 mo | Unknown | unknown | >1:320 | 7 |
| 6 | 7 y / M | MP + EBV | Antibiotic (+) (amoxicillin → discontinued) | (+) | (+) | (-) | Days 6–11 | Days 6–11 | >1:4096 | Positive | 8 |
| 7 | 12 y / F | MP | Antibiotic (+) (azithromycin) | (+) | (+) | Eosinophil, lymphocyte | Unknown | Unknown | <1:64 | >1:116 | 9 |
| 8 | 18 y / F | MP | Antibiotic (+) (levofloxacin) | (+) | (+) | Eosinophil, monocyte | Unknown | Unknown | >1:8192 | >1:20,480 | 10 |
| 9 (present case) | 6 y / M | MP + KD | Antibiotic (+) (ABPC/SBT) + IVIG + ASA | (+) | (+) | (-) | Days 9–16 | Days 9–1 mo | >1:8192 | >1:40,960 | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Blood groups and transfusion · Hematological disorders and diagnostics
Introduction
Mycoplasma pneumoniae is a common respiratory pathogen in children, classified as an atypical bacterium, and can trigger immunological reactions in the host [1]. Secondary cold agglutinin disease (CAD), which causes erythrocyte agglutination, may serve as an indicator of this infection [1,2]. In this context, neutrophil agglutination is a rare phenomenon, particularly in children. Kawasaki disease (KD) is a common vasculitis affecting young children [3], and some cases have been reported to be associated with M. pneumoniae infection [4]. Given the serious cardiovascular complications of KD, early diagnosis and treatment are essential. Here, we describe a case of Mycoplasma-associated KD with secondary CAD accompanied by both erythrocyte and neutrophil agglutination. A review of relevant literature is also provided.
Case presentation
A previously healthy six-year-old boy presented with mild respiratory symptoms and a high-grade fever. On illness day five, he was initially diagnosed with acute sinusitis at a local clinic and was treated with oral antibiotics (amoxicillin hydrate), but his symptoms did not resolve. Subsequently, he developed conjunctival injection, a strawberry tongue, an erythematous mouth, and bilateral cervical lymphadenopathy. Upon admission, seven days after disease onset, his vital signs were as follows: body temperature, 38.0 °C; blood pressure, 84/40 mmHg; pulse rate, 123 beats per minute; respiratory rate, 24 breaths per minute; and oxygen saturation, 100% on ambient air. He met four diagnostic criteria for KD according to the Japanese guidelines [3], and incomplete KD was suspected.
Blood tests revealed mild inflammation (C-reactive protein, 3.0 mg/dL; white blood cell count, 5,900/μL with 65% neutrophils) and mild hemolysis (total bilirubin, 0.2 mg/dL; lactate dehydrogenase, 427 U/L; hemoglobin, 13.1 g/dL), along with a positive direct Coombs test (Table 1). Although M. pneumoniae infection was prevalent in the community at that time, nasal M. pneumoniae DNA testing was negative. A chest X-ray obtained at admission showed no evidence of pneumonia (Figure 1). Echocardiography revealed no cardiac involvement, including coronary arterial lesions (Figure 2).
Chest X-ray at admission.A chest X-ray obtained at admission showed no evidence of pneumonia.
Echocardiography at admission.Echocardiography revealed no cardiac involvement, including coronary arterial lesions.
Nine days after disease onset, antibiotic therapy with sulbactam/ampicillin (150 mg/kg/day) did not resolve the fever or KD symptoms; therefore, incomplete KD was confirmed. On the same day, peripheral blood agglutination was observed for the first time during the clinical course at room temperature (Figure 3, Panel A) and disappeared after warming to 37 °C, indicating cold agglutination, as noted by a medical technologist. Additionally, both erythrocyte (yellow arrows) and neutrophil (red arrows) agglutination were identified (Figure 3, Panel B), a finding rarely reported in KD. Anti-neutrophil cytoplasmic antibody tests were negative. High titers of cold agglutinins (>1:8192) suggested secondary CAD. Considering the epidemic status of Mycoplasma infection and the presence of secondary CAD, concomitant Mycoplasma infection was strongly suspected, leading to the diagnosis of Mycoplasma-associated KD and secondary CAD with neutrophil aggregation.
Peripheral blood agglutination and smear findings. (A) Peripheral blood agglutination was observed at room temperature and disappeared after warming to 37 °C, indicating cold agglutination. (B) Both erythrocyte (yellow arrows) and neutrophil (red arrow) agglutination were observed in the peripheral blood smear (May–Giemsa stain, ×400).
The patient was treated with intravenous immunoglobulin (IVIG, 2 g/kg) and oral aspirin (30 mg/kg) for KD, which led to the prompt resolution of both KD and respiratory symptoms. He exhibited no cardiac involvement, including coronary artery lesions and pericarditis, during the course.
Subsequent testing confirmed elevated M. pneumoniae antibody titers (passive agglutination test, 40,960; IgM, 20,480). As M. pneumoniae antibody titers decreased, neutrophil and erythrocyte agglutination normalized over one and four weeks, respectively (Figure 4).
Clinical course of erythrocyte and neutrophil agglutination with Mycoplasma pneumoniae antibody titers.As M. pneumoniae antibody titers decreased, neutrophil and erythrocyte agglutination normalized over one and four weeks, respectively. The left Y-axis represents the M. pneumoniae antibody titers, and the right Y-axis represents the cold agglutinin titers.
Discussion
We report a pediatric case of Mycoplasma-associated KD characterized by both erythrocyte and neutrophil agglutination. Although neutrophil agglutination, a rare phenomenon observed in clinical practice, is generally regarded as having limited clinical significance, the present case is noteworthy for two reasons. First, these agglutinations facilitated the concomitant diagnosis of Mycoplasma infection. Second, Mycoplasma infection can coexist with KD, warranting special consideration in both diagnosis and management.
In this patient, both erythrocyte and neutrophil agglutinations were identified on day nine after disease onset, which allowed the concomitant diagnosis of Mycoplasma infection. Secondary CAD associated with Mycoplasma infection, resulting in erythrocyte agglutination, is well recognized [1,2]. Conversely, neutrophil agglutination is a rare occurrence. Leukoagglutination can be classified into two types: (1) ethylenediaminetetraacetic acid (EDTA)-dependent leukoagglutination (the most common) and (2) EDTA-independent cold-induced leukoagglutination [5]. The latter has been described in association with cirrhosis, infections (*M. pneumoniae *infection or infectious mononucleosis), autoimmune diseases, uremia, immunosuppression, and malignancies [5].
Neutrophil agglutination is particularly rare in children, with most cases being associated with Mycoplasma infection, as observed in the present case. A review of the literature identified nine pediatric cases, including the present one, of Mycoplasma infection accompanied by neutrophil agglutination (Table 2) [6-10]. The ages ranged from 6 to 18 years. Neutrophil agglutination was transient, resolving within two to three weeks in most cases, although one case required five months for normalization. Some patients exhibited additional leukocyte agglutination involving eosinophils, lymphocytes, or monocytes. Almost all cases demonstrated high cold-agglutinin titers (>1:512) and elevated M. pneumoniae antibody titers (>1:20,960), findings consistent with the present case. Two patients were also coinfected with herpes simplex virus or Epstein-Barr virus. The present case represents the first report of Mycoplasma-associated KD.
The mechanism of neutrophil agglutination remains undetermined. Erythrocyte agglutination can be explained by anti-I antibodies (cold agglutinins), which bind to the I antigen on the surface of erythrocytes during M. pneumoniae infection [11]. Because erythrocyte and neutrophil agglutinations are likely to share a similar underlying mechanism, our close observation that neutrophil and erythrocyte agglutinations normalized over one and four weeks, respectively, following the decline in Mycoplasma antibody titers suggests differences in their agglutination thresholds, which may partially explain the varying frequency of each.
KD is a common vasculitis in young children of unknown etiology and is most frequently reported in Japan [3]. To prevent serious cardiovascular complications such as coronary artery lesions, IVIG should be administered as early as possible. Recent meta-analyses have shown that approximately 30% of KD cases coexist with infections, including rhinovirus (19%), adenovirus (10%), and M. pneumoniae (10-22%) [4,12]. Among these, Mycoplasma-associated KD warrants special attention because its distinct inflammatory mechanisms may contribute to a pathophysiology different from that of non-Mycoplasma-associated KD [13]. M. pneumoniae infection induces systemic inflammation through multiple mechanisms: (1) direct injury caused by invasion or locally produced inflammatory cytokines; (2) indirect injury mediated by autoimmune reactions and immune complexes; and (3) vascular occlusion resulting from vasculitis or thrombosis [13]. As Mycoplasma-associated KD tends to present with prolonged fever after IVIG treatment and increased cardiac involvement compared with non-Mycoplasma-associated KD [14], this may be partly explained by immune functional alterations in the host caused by Mycoplasma infection [4]. Given the distinctive clinical features of Mycoplasma-associated KD, early identification of concomitant Mycoplasma infection is essential for an appropriate and timely treatment strategy. Interestingly, in the present case, agglutination observed in the peripheral blood smear provided valuable clues for the early diagnosis of concomitant Mycoplasma infection.
Additionally, we propose three clinically important considerations for managing the present case, i.e., Mycoplasma-associated KD with secondary CAD and neutrophil agglutination: pseudo-leukopenia, thrombosis, and pathogen-specific treatment. First, neutrophil agglutination can result in pseudo-leukopenia, necessitating careful interpretation of laboratory findings [15], although this was not observed in the present case. Because KD is an inflammatory disorder, the white blood cell count, particularly the neutrophil count, is essential for clinical decision-making and is among the major predictors of IVIG resistance [16]. Therefore, neutrophil agglutination could potentially mislead treatment planning in KD. Second, the presence of CAD may increase the risk of thrombosis [17]. This is particularly important in KD, as coronary arterial lesions represent the most serious complications. Although no cardiac involvement was observed in the present case, physicians should monitor cardiac lesions closely in similar cases. Third, pathogen-specific therapy may be required in cases of Mycoplasma-associated KD, as suggested in previous reports [6-10]. The reason why IVIG therapy alone (without antibiotic administration such as macrolides) resulted in prompt resolution of both KD symptoms and respiratory manifestations in the present case remains unclear. Nevertheless, this finding supports that the present case indeed represented true KD, although Mycoplasma infection can occasionally mimic KD [18].
Conclusions
We reported a rare case of KD with secondary CAD accompanied by both erythrocyte and neutrophil agglutination, which facilitated the concomitant diagnosis of Mycoplasma infection. Although M. pneumoniae DNA testing was initially negative, serological testing later confirmed the diagnosis through elevated M. pneumoniae IgM antibody titers. This case is the first to demonstrate a detailed serological course and its association with neutrophil and erythrocyte agglutination, suggesting different thresholds within a shared underlying mechanism. Because Mycoplasma-associated KD may require special attention in management, including IVIG treatment with or without antibiotics, this case also provides several clinically important insights for physicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The clinical presentation of pediatric Mycoplasma pneumoniae infections - a single center cohort Pediatr Infect Dis J Gordon O Oster Y Michael-Gayego A 6987053820193098551910.1097/INF.0000000000002291 · doi ↗ · pubmed ↗
- 2Neutrophil aggregation on the peripheral blood smear in a patient with cold agglutinin disease Ann Hematol Lee JH 8858869620172830330510.1007/s 00277-017-2962-5 · doi ↗ · pubmed ↗
- 3Revision of diagnostic guidelines for Kawasaki disease (6th revised edition)Pediatr Int Kobayashi T Ayusawa M Suzuki H 113511386220203300152210.1111/ped.14326 · doi ↗ · pubmed ↗
- 4The relationship between Mycoplasma and Kawasaki disease in pediatric patients: an updated systematic review and meta-analysis Arch Rheumatol Cheng M Zheng G Gao L Zhang B 1401483920243877470510.46497/Arch Rheumatol.2023.10149 PMC 11104762 · doi ↗ · pubmed ↗
- 5Cold-induced pseudoneutropenia in human immunodeficiency virus infection: first case report and review of related articles Indian J Hematol Blood Transfus Goyal P Agrawal D Kailash J Singh S 1481503020142533256410.1007/s 12288-013-0300-1PMC 4192267 · doi ↗ · pubmed ↗
- 6White blood cell aggregation in Mycoplasma pneumoniae infection Syonika Takiguchi M Iizuka A Nagao T 643648221981
- 7Neutrophil aggregates in a 13-year-old girl: a rare hematological phenomenon Ann Hematol Claviez A Horst HA Santer R Suttorp M 2512538220031270773110.1007/s 00277-003-0627-z · doi ↗ · pubmed ↗
- 8Combined neutrophil and erythrocyte agglutination in a 7-year-old boy J Pediatr Hematol Oncol Yenson PR Fleming A Kaikov Y Wadsworth LD 6646652920071780504910.1097/MPH.0b 013e 3181461662 · doi ↗ · pubmed ↗