Association between oxidative stress-related IGF-1 and prognosis after ischemic stroke: a systematic review and meta-analysis
Xinyu Liu, Jun Wang, Congcong Wang

TL;DR
This study finds that IGF-1, a protein linked to oxidative stress, may be associated with worse long-term outcomes after ischemic stroke, but not with stroke risk or short-term outcomes.
Contribution
The study identifies a potential long-term prognostic role of IGF-1 in ischemic stroke survivors beyond one year post-onset.
Findings
IGF-1 was not significantly associated with the risk of acute ischemic stroke.
IGF-1 was not significantly linked to short-term post-stroke outcomes.
IGF-1 was significantly associated with poor long-term outcomes more than one year after stroke onset.
Abstract
Insulin-like growth factor-1 (IGF-1), an oxidative stress–related neurotrophic factor, has been investigated in stroke due to its potential roles in neuronal survival and vascular regulation. However, findings on its association with ischemic stroke and functional prognosis remain inconsistent. This review aimed to evaluate the association between circulating IGF-1 levels and (1) the risk of ischemic stroke and (2) post-stroke outcomes. We systematically searched EMBASE, MEDLINE, PubMed, Google Scholar, and the Cochrane Library from inception to June 2021, and updated the search to November 2025. Case-control or cohort studies reporting risks or odds ratios with 95% confidence intervals were included. Summary estimates were pooled using random-effects models when heterogeneity was substantial. Our systematic literature search identified 10 articles. Four of these studies examined the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
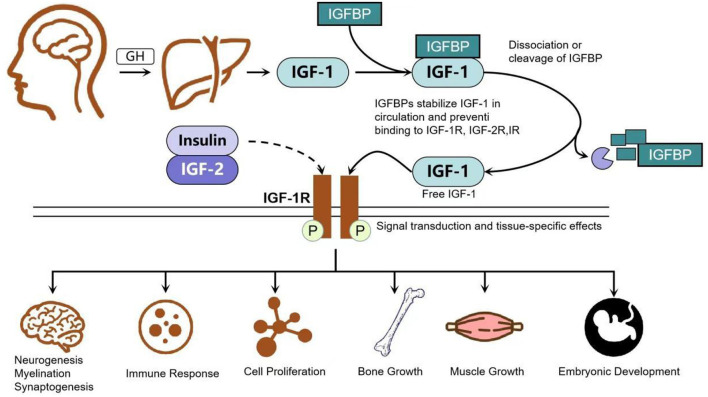 Figure 1
Figure 1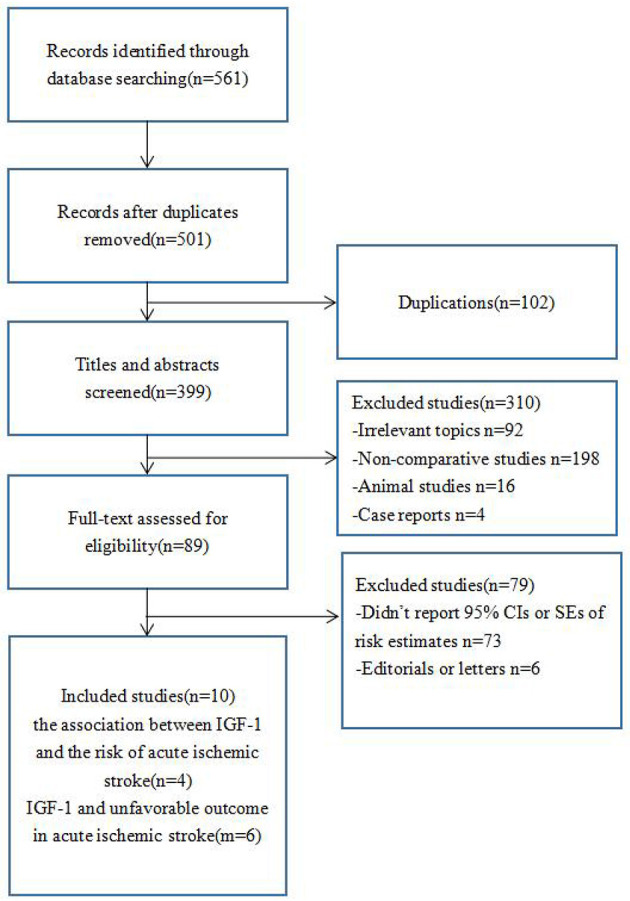 Figure 2
Figure 2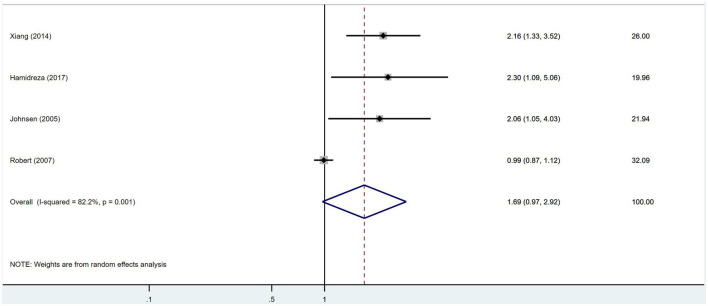 Figure 3
Figure 3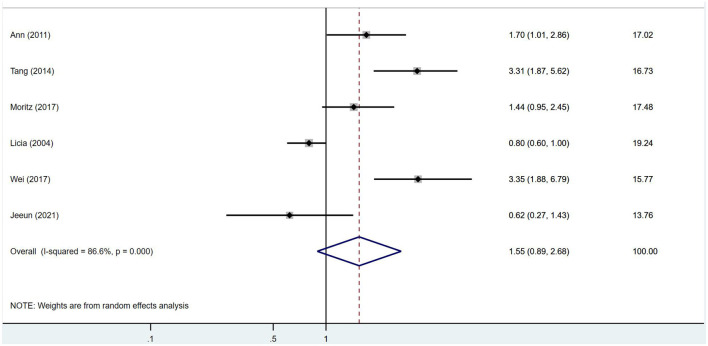 Figure 4
Figure 4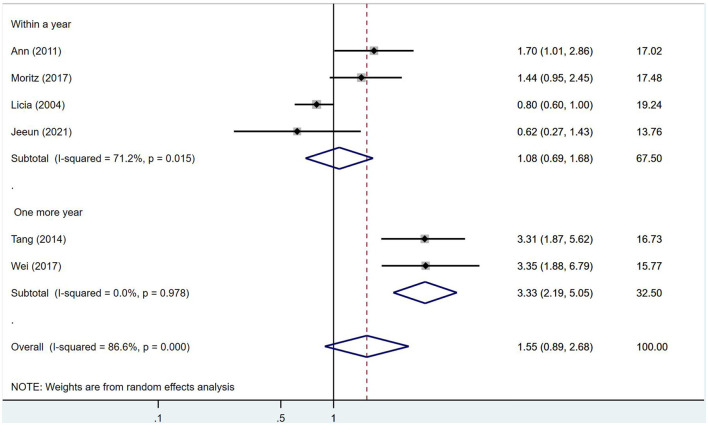 Figure 5
Figure 5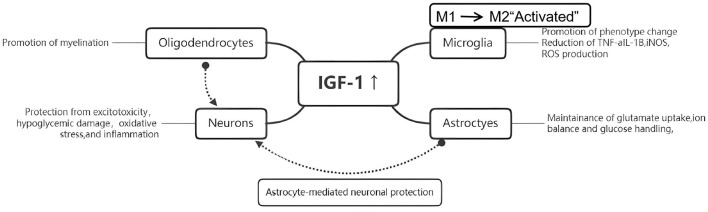 Figure 6
Figure 6|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|
| Ann 2011 ( | Belgium | Low serum IGF-I levels just after ischemic stroke onset are associated with a bad functional outcome. | 346 total 255 stroke | 6 hours after admission | 3 days to 3 months post | HR: 1.7 | NIHSS score; modified Rankin scale | 5 |
| Tang 2014 ( | China | Serum IGF-1 levels ≤ 130 ng/mL was as an value indicator for unfavorable functional outcome | 268 total 168 stroke | 24 hours after admission | Up to 1 year post | OR 3.31 95% CI: 1.87–5.62 | NIHSS score; modified Rankin scale | 6 |
| Moritz 2017 ( | America | Low IGF-1 levels (day 8) were independently associated with a decreased risk of an unfavorable outcome | 404 stroke | 0/8 days after admission | 3 months post | Day 8:OR 0.61 | modified Rankin scale | 6 |
| Licia 2004 ( | Italy | IGF-1 levels were inversely related to poor outcome (mainly death) at 3 and 6 months. | 173 total, 85 stroke | 24 hours after admission | Up to 6 months post | OR: 0.8 | Glasgow Coma Scale and stroke scores | 5 |
| Wei 2017 ( | China | The data showed that low serum IGF-1 levels at admission are associated with a high risk of poor outcome. | 120 total, 85 stroke | 24 hours after admission | 1 year post | OR: 3.35 | NIHSS score; modified Rankin scale | 7 |
| Jeeun 2021 ( | Korea | A higher serum IGF-1 level is associated with a lower | 379 stroke | 24 hours after admission | 3 months post | OR: 0.62 | NIHSS score | 7 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Xiang 2014 ( | China | Case-control study | 221 cases and 200 control subjects; | Time of Admission | OR: 2.16 95% CI: 1.33–3.52 | 6 |
| Hamidreza 2017 ( | America | Framingham Study | 757 individuals first quintile:151 fifth quintile:150 | Across 10 years | HR: 2.3 95% Cl: 1.09–5.06 | 5 |
| Johnsen 2005 ( | Denmark | Case-control study | 254 cases and 254 control subjects; | Across 3.1 years | OR: 2.06 95% CI: 1.05–4.03 | 7 |
| Robert 2007 ( | America | Cohort | 370 Ischemic stroke 1,122 Random subcohort | Across 5.6 years | HR: 0.99 95% CI: 0.87–1.12 | 6 |
- —National Center for Medical Rehabilitation Research10.13039/100006937
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGrowth Hormone and Insulin-like Growth Factors · Muscle Physiology and Disorders · TGF-β signaling in diseases
Introduction
1
Stroke is one of the leading causes of mortality and long-term disability worldwide, with ischemic stroke representing the most common subtype (1). Despite advances in acute reperfusion therapy, many stroke survivors continue to experience persistent neurological deficits and limited functional recovery (1). This highlights the importance of investigating biological pathways that contribute to ischemic brain injury and long-term outcome.
Insulin-like growth factor 1 (IGF-1), a peptide hormone widely studied in ischemic brain injury models, has shown significant neuroprotective effects. Experimental studies have demonstrated that delayed IGF-1 administration can reduce hypoxia-ischemia-induced neuronal damage and improve behavioral recovery in immature and adult ischemic stroke models (2–5). In addition to direct neuronal protection, estrogen–IGF-1 interactions play an important role in modulating neuroprotection following focal cerebral ischemia (6, 7).
IGF-1 also regulates oxidative stress and neuroinflammation, two key contributors to ischemic neuronal damage. It attenuates excessive calcium signaling in neural cells (8), promotes activity-dependent functional recovery in chronic stroke (9), and influences systemic cardiovascular outcomes relevant to stroke risk (10). Microglial and astroglial expression of IGF-1 and its binding proteins increases following hypoxia-ischemia, supporting glial survival and inflammatory regulation (11–16). IGF-1 suppresses microglial oxidative stress and inflammatory cytokine release (7, 17–21), while astrocytic IGF-1 and IGFBP-2 expression contributes to oxidative stress resistance (13, 16, 22, 23). Crosstalk with calcineurin, glucose transport pathways, and Na^+^/K^+^-ATPase-related mechanisms further emphasizes its involvement in glial–neuronal interactions and aging-related vulnerability (19, 24–29). Collectively, IGF-1 plays a key role in regulating oxidative stress, inflammation, and brain repair after ischemia (Figure 1), reinforcing its relevance to stroke pathophysiology.
Growth hormone controls the production and release of IGF-1 in hepatocytes, the binding and separation of circulating IGFBP and its selective receptor IGF-1R, and closely regulates IGF-1 signaling.
Based on these mechanistic insights, circulating IGF-1 has been proposed as a biomarker associated with ischemic brain injury and recovery (6, 9, 10). However, clinical studies have yielded inconsistent results regarding its association with ischemic stroke incidence or functional outcomes, likely due to differences in study design, patient characteristics, timing of IGF-1 measurement, and adjustment for confounders. These discrepancies underscore the need for a systematic synthesis of available evidence.
Therefore, this systematic review and meta-analysis aimed to (1) assess the association between circulating IGF-1 levels and the risk of ischemic stroke, and (2) examine whether IGF-1 is associated with unfavorable outcomes after ischemic stroke, with particular attention to long-term prognosis.
Unlike previous individual studies, our meta-analysis simultaneously evaluates IGF-1 in relation to both ischemic stroke risk and long-term functional prognosis, with subgroup analyses based on follow-up duration.
Materials and methods
2
Data sources and searches
2.1
We conducted a systematic search in EMBASE, PubMed, the Cochrane Library and Google Scholar (as a supplementary source) from their inception to June 2021 to identify studies evaluating the effect of IGF-1 on the risk and functional outcomes of ischemic stroke. No language restrictions were applied. The search strategy included the terms “insulin-like growth factor 1,” “IGF-1,” “ischemic stroke,” and “stroke.” Additionally, we reviewed the references of retrieved articles to identify any further relevant studies. In response to reviewer comments, we updated the search in PubMed, Embase, the Cochrane Library, and Google Scholar up to November 2025 using the same search terms and eligibility criteria. The updated search identified several additional reviews, experimental studies, and one cross-sectional clinical study; however, none fulfilled the predefined inclusion criteria (prospective cohort or case-control design assessing ischaemic stroke incidence or post-stroke functional outcome with OR/RR/HR and 95% CI). Therefore, no new primary studies were added to the quantitative synthesis.
Study selection criteria
2.2
Published articles were included if they: (1) had a case-control or cohort design, (2) evaluated the association between IGF-1 and ischemic stroke, (3) assessed the impact of IGF-1 on unfavorable outcomes after ischemic stroke, and (4) reported the odds ratio (OR) or risk ratio (RR) with 95% confidence intervals (CI). Duplicate publications or those reporting on the same study population were excluded, with the most recent publication selected. Studies on pediatric populations, articles with insufficient data, and those focused solely on transient ischemic attacks were also excluded.
Literature search
2.3
Our systematic literature search identified 10 articles. Four of these studies examined the association between IGF-1 and the risk of acute ischemic stroke, while the other six focused on the relationship between IGF-1 and unfavorable outcomes after acute ischemic stroke. A flow diagram detailing the study selection process is shown in Figure 2. Of the 561 titles identified from the databases, 10 studies were included in the final analysis after reviewing the full text of the remaining studies. The primary reason for exclusion was the lack of 95% confidence intervals (CIs) or standard errors of risk estimates.
Flow diagram of study selection.
Data extraction and quality assessment
2.4
Two authors independently assessed the eligibility of all retrieved studies and extracted relevant data using a standardized data form. The data form included the following items: study name (with the first author's name and year of publication), journal name, country, study design, study population, follow-up duration, and adjusted odds ratios (ORs) or risk ratios (RRs) with 95% confidence intervals (CIs). The authors compared their lists, and any disagreements were resolved by consensus. Study quality was assessed independently by two reviewers using the Newcastle-Ottawa Scale (NOS), evaluating participant selection, comparability, and outcome assessment.
Statistical methods
2.5
To calculate the summary risk ratio (RR) and 95% confidence interval (CI), we used the most-adjusted RR or odds ratio (OR) and its 95% CI from each study. The overall effect size was recalculated by pooling risk estimates and unfavorable outcomes using the inverse-variance method. Heterogeneity across studies was assessed using I^2^ statistics. When substantial heterogeneity was detected, the summary estimate was calculated using a random-effects model. Otherwise, the pooled estimate was derived using a fixed-effects model. Subgroup analyses were conducted based on follow-up duration. All data analyses were performed using STATA 15.1.
Results
3
Study characteristics and quality assessment
3.1
Descriptive data for the studies included in our analysis are summarized in Tables 1, 2. The studies were conducted in Japan, Belgium, China, the United States, Italy, Korea, and Denmark. Study-specific quality scores are also summarized in Tables 1, 2, with scores ranging from 6 to 10; the median score was 6.
Overall analyses
3.2
No significant association was found between IGF-1 and ischemic stroke (RR = 1.69, 95% CI = 0.97–2.92, I^2^ = 82.2%, random-effects model, Figure 3), nor was there an impact of IGF-1 on unfavorable outcomes after ischemic stroke (RR = 1.55, 95% CI = 0.89–2.68, I^2^ = 86.6%, random-effects model, Figure 4).
Forest plots shows there was no significant association between IGF-1 and ischemic stroke.
No impact of IGF-1 on unfavorable outcome after ischemic stroke was found.
Follow-up duration affects the severity of post-stroke disability and may better reflect recovery vs. degeneration, therefore subgroup analyses were stratified by 1-year follow-up. However, in the subgroup analysis, IGF-1 was significantly associated with poor prognosis more than 1 year after stroke onset (RR = 3.33, 95% CI = 2.19–5.05, I^2^ = 0%, random-effects model, Figure 5). As only a few studies contributed to this subgroup analysis, this finding should be considered exploratory and requires confirmation in future research.
In the subgroup analysis of the effect of IGF-1 on unfavorable outcome after ischemic stroke, IGF-1 was significantly associated with a poor prognosis at more than 1 year after stroke onset.
Publication bias
3.3
To assess the potential impact of publication bias on the meta-analysis results, we used a funnel plot. The funnel plot of the included studies showed clear left-right symmetry, indicating no evidence of publication bias.
Discussion
4
In this systematic review and meta-analysis, we found no significant association between circulating IGF-1 levels and either the risk of acute ischemic stroke or unfavorable short-term outcomes following stroke onset. However, patients with higher IGF-1 levels exhibited an increased risk of poor prognosis at >1 year post-stroke, suggesting potential relevance for long-term outcomes. Given the substantial global burden of stroke-related disability, these findings highlight IGF-1 as a possible biomarker for risk stratification during recovery phases.
IGF-1 plays a fundamental role in growth regulation, metabolism, and tissue repair (30–34). Beyond developmental functions, circulating IGF-1 levels correlate with musculoskeletal performance (35) and show altered regulation across various chronic diseases including cancer and metabolic disorders (36–39). Epidemiological studies have reported inconsistent associations between IGF-1 and stroke risk (40, 41), while preclinical evidence supports its vascular and neuroprotective properties (42, 43). Low IGF-1 levels have been linked to severe neurological injury in acute stroke settings (44), cognitive decline in the elderly (45), and improved recovery with supplementation in animal models (42).
Mechanistically, IGF-1 exerts neuroprotective functions through several complementary pathways (Figure 6). First, IGF-1 reduces oxidative stress and inflammation by modulating microglial activation and cytokine production (42, 43). It has been shown to regulate early atherosclerotic processes and endothelial integrity (46). In clinical studies, lower IGF-1 levels have been associated with poorer outcomes after ischemic stroke (47–49), although findings vary according to baseline patient factors (50). Second, IGF-1 binds to its receptor (IGF-1R) and activates downstream PI3K/Akt and MAPK survival pathways (51–55), which enhance neuronal survival, synaptic plasticity, and metabolic support. IGF-1R is widely expressed in neuronal and glial tissues (56–58), and delays in IGF-1 signaling reduce neuroprotective and anti-apoptotic responses (59, 60). Third, IGF-1 promotes angiogenesis and neurogenesis, both essential for long-term neurological restoration after stroke (61–67).
Key cellular functions in the brain are known to be regulated by IGF-1.
These biological mechanisms provide a rational explanation for our finding: IGF-1 may be more closely associated with long-term neurological remodeling rather than immediate post-stroke injury, consistent with the >1-year subgroup result. Early outcomes are primarily determined by infarct size and reperfusion damage, whereas long-term prognosis reflects ongoing neuronal recovery, synaptic reorganization, and vascular remodeling—processes in which IGF-1 plays major roles.
However, substantial clinical and methodological heterogeneity must be acknowledged. IGF-1 levels are influenced by age, metabolic syndrome, nutritional intake, IGFBP-mediated bioavailability, and hormonal status (36–38, 50), while laboratory assays and sampling times varied widely among included studies. Substantial heterogeneity across studies may reflect differences in study design, population characteristics, timing of IGF-1 measurement, laboratory assays, and inconsistent adjustments for confounding factors such as age, metabolic disorders, and circulating IGFBPs. Therefore, the pooled estimates should be interpreted cautiously. Furthermore, IGF-1 may reflect systemic anabolic capacity rather than disease-specific neuroprotection, complicating causal interpretation.
Our results also showed high statistical heterogeneity. This likely arises from regional diversity, inconsistent confounder adjustments, and variations in timing of outcome assessment. Although subgroup analysis reduced heterogeneity and revealed a statistically significant association, this finding is based on limited data and should be considered exploratory.
Clinically, IGF-1 measurement is feasible and inexpensive, indicating potential as a prognostic indicator for post-stroke management. Patients with persistently low or elevated IGF-1 levels may benefit from closer monitoring and tailored rehabilitation strategies. Nonetheless, practical challenges remain, including assay standardization, reference ranges by age and sex, and integration with existing prognostic models.
This study has several limitations. All included studies were observational; thus, causality cannot be inferred. Residual confounding may persist despite adjusted analyses. Individual patient-level data were unavailable, preventing stratification by stroke subtype, therapeutic interventions, and comorbidity burden. Further well-designed longitudinal cohort studies and interventional trials are required to validate whether modifying IGF-1 signaling could influence long-term stroke prognosis.
Taken together, although preliminary evidence suggests IGF-1 may contribute to long-term neurological outcomes through anti-inflammatory and pro-repair processes, the current findings should be interpreted cautiously. IGF-1 remains a promising prognostic biomarker, but its role as a therapeutic target for ischemic stroke recovery has yet to be confirmed.
Conclusions
5
This meta-analysis suggests that oxidative stress-related IGF-1 may be associated with long-term unfavorable outcomes in patients with ischemic stroke, especially beyond 1 year after symptom onset. However, no significant associations were identified between IGF-1 levels and the risk of incident ischemic stroke or short-term functional outcomes.
Given the limited number of studies included, substantial heterogeneity, and the observational nature of the evidence, these findings should be interpreted with caution. IGF-1 may serve as a potential prognostic biomarker for long-term functional decline after stroke, but causality and its therapeutic implications remain uncertain.
Future prospective, large-scale studies with standardized IGF-1 measurements and comprehensive adjustment for confounding factors are needed to confirm the prognostic utility of IGF-1 and clarify its biological relevance in post-stroke recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boehme AK Esenwa C Elkind MSV. Stroke risk factors, genetics, and prevention. Circul Res: J Am Heart Assoc. (2017) 120:472–495. doi: 10.1161/CIRCRESAHA.116.30839828154098 PMC 5321635 · doi ↗ · pubmed ↗
- 2Zhong J Zhao L Du Y Wei G Yao WG Lee WH. Delayed IGF-1 treatment reduced long-term hypoxia–ischemia-induced brain damage and improved behavior recovery of immature rats. Neurol Res. (2013) 31:483–9. doi: 10.1179/174313208 X 33813319500451 · doi ↗ · pubmed ↗
- 3De Geyter D De Smedt A Stoop W De Keyser J Kooijman R. Central IGF-I receptors in the brain are instrumental to neuroprotection by systemically injected IGF-I in a rat model for ischemic stroke. CNS Neurosci Ther. (2016) 22:611–6. doi: 10.1111/cns.1255027080541 PMC 6492886 · doi ↗ · pubmed ↗
- 4Ahmad S., Erik B, Ron K. Insulin-like growth factor-1 is neuroprotective in aged rats with ischemic stroke. Front Aging Neurosci. (2019) 11:349. doi: 10.3389/fnagi.2019.0034931920629 PMC 6918863 · doi ↗ · pubmed ↗
- 5De Geyter D Stoop W Sarre S De Keyser J Kooijman R. Neuroprotective efficacy of subcutaneous insulin-like growth factor-I administration in normotensive and hypertensive rats with an ischemic stroke. Neuroscience. (2013) 250:253–62. doi: 10.1016/j.neuroscience.2013.07.01623872393 · doi ↗ · pubmed ↗
- 6Sohrabji F. Estrogen-IGF-1 interactions in neuroprotection: ischemic stroke as a case study. Front Neuroendocrinol. (2015) 36:1–14. doi: 10.1016/j.yfrne.2014.05.00324882635 PMC 4247812 · doi ↗ · pubmed ↗
- 7Wendy S Deborah DG Jacques DK Ron K. Neuroprotective effects exerted by 17β-estradiol (E 2) and the insulin-like growth factor IGF-I after a focal cerebral ischemia in the endothelin-1 rat model. Front Neurosci. (2015) 9. doi: 10.3389/conf.fnins.2015.89.0005925688184 · doi ↗
- 8Heidenreich DJ Reedy MV Brauer PR. Homocysteine enhances cardiac neural crest cell attachment in vitro by increasing intracellular calcium levels. Dev Dyn. (2008) 237:2117–28. doi: 10.1002/dvdy.2164418651663 · doi ↗ · pubmed ↗