CT and MRI Manifestations of Pancreatic Hemangioma: A Literature Review and a New Case Report
Jing Zhang, Jingjing Chen, Dongmei Zou, Xu Cao

TL;DR
This paper reports a rare case of pancreatic hemangioma and discusses its imaging features using CT and MRI to improve diagnosis.
Contribution
A new case report and literature review highlighting the atypical imaging features of pancreatic hemangioma.
Findings
CT and MRI showed a multilocular, low-density lesion with mild enhancement in the pancreas head.
DWI and ADC values indicated no significant diffusion restriction, aiding in differential diagnosis.
Multimodal imaging is crucial for diagnosing pancreatic hemangioma and distinguishing it from other lesions.
Abstract
Pancreatic hemangioma is an extremely rare benign tumor occurring in the pancreas. Preoperative diagnosis is challenging due to its lack of specificity in clinical manifestations and imaging examinations. A pancreatic lesion was found during physical examination of a 54‐year‐old woman who had no symptoms of abdominal discomfort. Computed tomography (CT) revealed a round, well‐defined, and low‐density lesion in the head of the pancreas with a multilocular or honeycomb shape, mild–moderate enhancement of its internal septum, and no enhancement of the cystic component. Magnetic resonance imaging (MRI) showed an abnormal signal lesion in the head of the pancreas, with isointensity and hypointensity on T1‐weighted images and inhomogeneous hyperintensity on T2‐weighted images. The isointensity on diffusion weighted imaging (DWI) and high apparent diffusion coefficient (ADC) values suggested…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
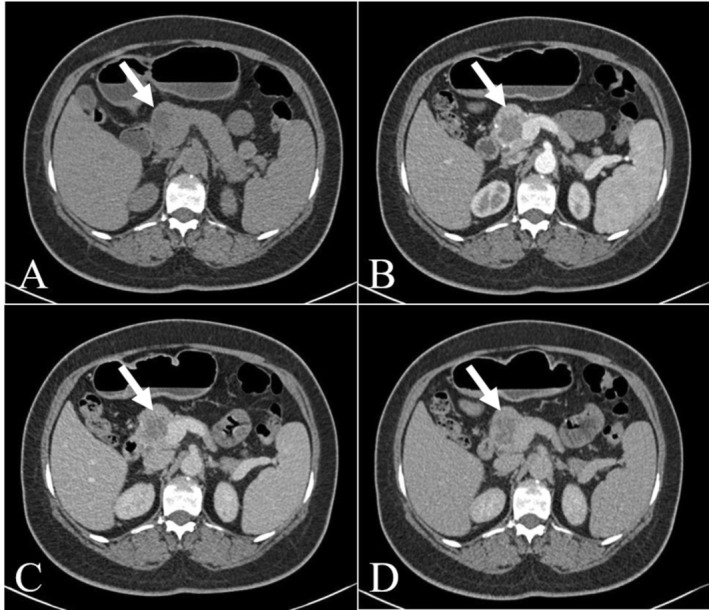 FIGURE 1
FIGURE 1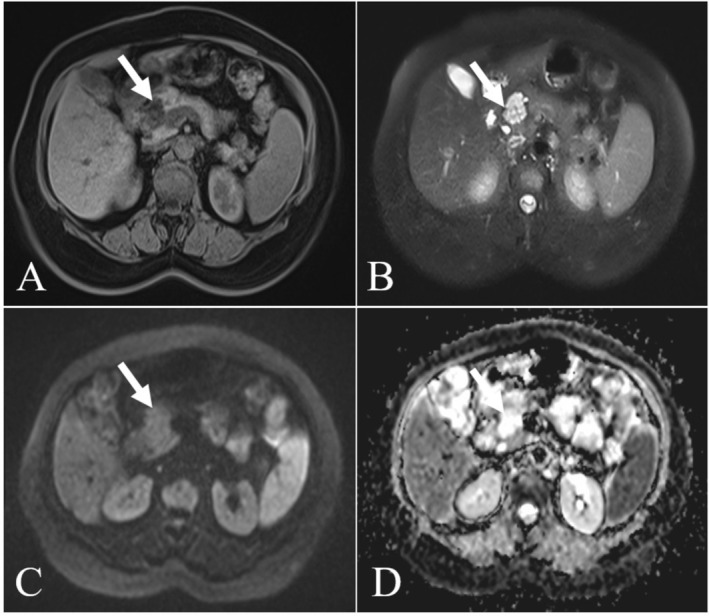 FIGURE 2
FIGURE 2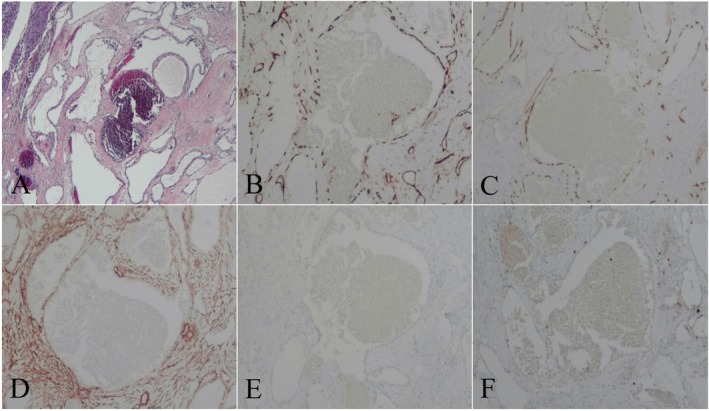 FIGURE 3
FIGURE 3| No. | Year | Author | Age/sex | Clinical symptom | Imaging examination | Clinical diagnosis | Site/size (cm) | Treatment | Follow up |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1939 | Ranstrom [ | 61/F | — | Found at autopsy | — | Head/7 × 7 | — | — |
| 2 | 1961 | Ringoir et al. [ | 71/F | Melena | Plain abdominal film, transvenous cholangiography | — | Head/15 × 15 | Retrocolic gastroenterostomy, vagotomy | — |
| 3 | 1972 | Colardyn et al. [ | 42/F | Upper abdominal pain radiating to the back | Plain abdominal film, angiography | — | Body tail/− | Fat free diet, anticholinergic | — |
| 4 | 1985 | Mangin et al. [ | 62/F | Abdominal discomfort, vomiting | US, ERCP, CT, angiography | — | Head to tail/20 × 7 | Laparotomy with observation | — |
| 5 | 1991 | Kobayashi et al. [ | 30/M | Abdominal bloating | US, CT, MRI, angiography | — | Head/maximum diameter 20 | Pancreatoduodenectomy | — |
| 6 | 1991 | Dageförde et al. [ | 79/F | Abdominal pain | US, ERCP, angiography | — | Body tail/6 × 3 | Observation | — |
| 7 | 2003 | Chang et al. [ | 70/F | Fever, chills, productive cough, and vague epigastralgia | CT, angiography | Serous/cystic adenoma/adenocarcinoma | Body tail/4.0 × 3.2 × 3.0 | Subtotal pancreatectomy | No signs of recurrence or metastasis 14 months after surgery |
| 8 | 2006 | Plank et al. [ | 36/M | Abdominal pain | CT, MRI, intraoperative US | — | Head/maximum diameter 3 | Not resected | — |
| 9 | 2008 | Xu et al. [ | 60/F | Upper abdominal pain, fever | US, CT | Adenoma/adenocarcinoma | Tail/2 × 2 | Pancreas body tail resection + splenectomy | Successful recovery and healthy survival after surgery |
| 2008 | Xu et al. | 41/F | No obvious clinical symptoms | US | Adenoma/islet cell carcinoma | Body/2.5 × 2.0 | Partial resection of the body of the pancreas | ||
| 2008 | Xu et al. | 30/F | Upper abdominal pain, obstruction | US | Benign and cystic tumor | Head/6 × 5 | Pancreaticoduodenectomy | ||
| 10 | 2009 | Mundinger et al. [ | 45/F | Radiating pain in the left upper abdomen | CT, MRI | — | Head/6.2 × 5.3 | Frozen section | — |
| 11 | 2011 | Weidenfeld et al. [ | 73/F | Radiating pain in the upper abdomen | CT | — | Head/5.5 × 4.0 × 3.0 | Whipple's procedure | — |
| 12 | 2011 | Lee et al. [ | 49/F | Vertigo, palpitation | US, intraoperative US, CT | Mucious cyst with malignant features | Neck/5 | Central partial pancreatectomy and gastrostomy | Symptoms disappeared after 6 months |
| 13 | 2012 | Kersting et al. [ | 53/M | No symptoms | US, CT, MRI | Adenocarcinoma | Head/8 | Extirpation of the tumor | — |
| 14 | 2013 | Malik et al. [ | 70/F | — | CT | — | Head/8 | Pylorus preserving pancreatoduodenectomy | — |
| 15 | 2013 | Lu and Wu [ | 23/F | No symptoms | US, CT, MRI | — | Head/5.0 × 4.0 × 3.1 | — | — |
| 16 | 2014 | Williamson et al. [ | 78/F | Increasing epigastric pain | EUS, CT | — | Head/4 | Observation | Repeat CT at four and ten months was unchanged |
| 17 | 2014 | Naito et al. [ | 40/F | Abdominal pain | CT, MRI | Multilocular septated cystic mass | Body tail/10 | Pancreatectomy | No recurrence 6 years after surgery |
| 18 | 2014 | Kim et al. [ | 48/F | Incidentally detected | CT, MRI | Neuroendocrine tumor | Tail/0.5 × 0.6 | Distal pancreatectomy | — |
| 2014 | Kim et al. | 53/F | Abdominal pain | CT, MRI | Cystic mass | Body/− | Distal pancreatectomy | — | |
| 19 | 2015 | Mondal et al. [ | 18/F | Epigastric pain | US, CT, MRI | Benign cyst | Head/5 × 6 | Pylorus preserving pancreatoduodenectomy | No symptoms 6 months after surgery |
| 20 | 2015 | Lu and Yang [ | 28/F | Abdominal pain | CT | Serous cystadenoma or pseudocyst | Body tail/5.5 × 6.5 × 5.5 | Subtotal pancreatectomy and splenectomy | Without any signs of recurrence; follow‐up was for 2 years and 4 months. |
| 21 | 2015 | Soreide et al. [ | 38/F | Left epigastric pain, nausea, palpable left subcostal mass | US, MRI | Solid pseudopapillary epithelial neoplasm | Tail/19.5 × 10 × 7 | Distal pancreatectomy, splenectomy | No complaints or concerns |
| 22 | 2016 | Bratu et al. [ | 64/M | Acute upper abdominal pain, weight loss | US, endoscopy, CT | Adenocarcinoma | Body/3.2 × 1.9 | Surgical resection of the lesion | — |
| 23 | 2017 | Al Warith et al. [ | 71/F | Left iliac fossa pain | CT, MRI, EUS | Mucinous neoplasia | Tail/2.4 | Laparoscopic distal pancreatectomy, splenectomy | — |
| 24 | 2018 | Raymundo et al. [ | 36/M | Lumbar pain | CT, MRI, ERCP | Neuroendocrine tumor | Body tail/2.4 × 2.2 | Distal pancreatectomy, splenectomy | After 6 months, the patient is in good condition, without abdominal symptoms. |
| 25 | 2019 | Lianyuan et al. [ | 63/M | Left upper abdominal pain and defecation unformed | CT, EUS | — | Head/10 × 5 × 5 | Pancreaticoduodenectomy | Remained symptom free 2 years after surgery |
| 26 | 2020 | Zhou and Chen [ | 71/F | Slight pain on left upper abdomen | US, CT | Cystadenoma or adenocarcinoma | Head/3.2 × 3.0 | Central pancreatectomy with pancreatojejunostomy | No complaints or recurrence of abdominal pain occurred in the next 3 years |
| 27 | 2020 | Jin et al. [ | 52/F | Epigastric pain | EUS, CT | Mucinous/serous cystic neoplasm | Body/4.6 × 4.6 × 3.4 | Pancreaticojejunostomy | No recurrence after 10 months of follow‐up |
| 28 | 2021 | Langmaid et al. [ | 69/F | No symptoms | EUS, CT, MRI, PET | — | Head/1.1 | Conservative management | Remained well and asymptomatic |
| 29 | 2023 | Li [ | 18/M | Physical examination | EUS, CT, MRI | — | Tail/6.4 × 5.1 | Distal pancreatic tumor resection | No complications or recurrences were observed during the follow‐up period |
| 30 | 2024 | Lei et al. [ | 60/M | Intermittent dull pain, aggravated at night | CT, MRI | — | Head/5.8 × 7.5 | Abdominal surgery | No tumor recurrence or metastasis was found in the postoperative follow‐up for 5 years |
| 31 | — | Present case | 54/F | No symptoms | CT, MRI | Serous cystadenoma | Head/2.5 × 1.5 × 2.0 | Laparoscopic pancreaticoduodenectomy | No complications on clinical follow‐up 4 months after surgery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Pancreatic and Hepatic Oncology Research · Organ Transplantation Techniques and Outcomes
Introduction
1
Hemangiomas result from the rapid proliferation of endothelial cells in early infancy and then degenerate over time, which are relatively common benign tumors that can occur anywhere in the body and are most commonly found under the skin of the head, neck, and trunk [1]. Among the internal organs, the liver and spleen are common sites where hemangiomas occur. However, hemangiomas occurring in the pancreas are extremely rare [2]. Pancreatic hemangioma is poorly recognized and difficult to diagnose preoperatively because of its low incidence, varied clinical presentation, and atypical imaging findings. Therefore, most lesions are diagnosed incidentally after surgery.
We recently encountered a woman with an occupancy in the head of the pancreas, which was proposed to be diagnosed as a serous cystadenoma on preoperative computed tomography (CT) and magnetic resonance imaging (MRI) but turned out to be diagnosed as pancreatic hemangioma postoperatively. Therefore, we analyzed the imaging findings of this case of pancreatic hemangioma and reviewed the literature to deepen our understanding of this rare disease.
Case History/Examination
2
A 54‐year‐old female was transferred to our hospital due to a lesion in the head of the pancreas accidentally found by ultrasonography (US) during physical examination in an outside hospital. Subsequently, she was treated with medication (details unknown) and came to our hospital for review. Except for the past history of hepatitis B and hysterectomy, any symptoms of abdominal discomfort were denied by the patient. Laboratory tests after admission showed three positives: hepatitis B surface antigen (+), anti‐HBe (+), and anti‐HBc (+). In addition, tumor markers, including carcinoembryonic antigen (CEA), alpha‐fetoprotein (AFP), carbohydrate antigen 125 (CA125), carbohydrate antigen 199 (CA199), and other routine laboratory tests were within normal ranges. Non‐contrast CT revealed a round, well‐defined, and low‐density lesion in the head of the pancreas, measuring about 2.5 × 1.5 × 2.0 cm. Additionally, no significant calcification was observed. Enhancement scans showed internal segments of the lesion with mild to moderate enhancement and internal cystic components with no enhancement, which appear as a multilocular or honeycomb shape (Figure 1A–D). MRI showed an abnormal signal lesion in the head of the pancreas, with isointensity and hypointensity on T1‐weighted images and inhomogeneous hyperintensity on T2‐weighted images. The isointensity on diffusion weighted imaging (DWI) and high apparent diffusion coefficient (ADC) values indicated low impedance to the diffusion of water molecules within the lesion. In addition, the lesion was not connected to the main pancreatic duct and there was no dilatation of the main pancreatic duct (Figure 2A–D). Finally, a combination of preoperative clinical and imaging tests led to the diagnosis of a serous cystadenoma of the pancreatic head.
Non‐enhanced computed tomography (CT) revealed a round, well‐defined, and low‐density lesion in the head of the pancreas, measuring about 2.5 × 1.5 × 2.0 cm. Additionally, no significant calcification was observed (A). Enhancement scans showed internal segments of the lesion with mild to moderate enhancement and internal cystic components with no enhancement, which appear as a multilocular or honeycomb shape (B–D).
Magnetic resonance imaging (MRI) showed an abnormal signal nodule in the head of the pancreas, with isointensity and hypointensity on T1‐weighted images (A) and inhomogeneous hyperintensity on T2‐weighted images (B). The isointensity on diffusion weighted imaging (DWI; C) and high apparent diffusion coefficient (ADC; D) values indicated a low impedance to diffusion of water molecules within the lesion. In addition, the lesion was not connected to the main pancreatic duct and there was no dilatation of the main pancreatic duct.
Differential Diagnosis, Investigations and Treatment
3
Clinically, pancreatic hemangiomas are easily confused with other common cystic pancreatic lesions such as pseudocysts, serous cystadenomas, mucinous cystadenomas, and intraductal papillary mucinous neoplasms (IPMN). Pancreatic pseudocysts do not enhance on contrast‐enhanced CT scans, and patients often have a history of chronic pancreatitis. Serous cystadenomas predominantly occur in elderly women and typically present on imaging as cystic or lobulated lesions with septa, which may calcify. Mucinous cystadenomas are more common in middle‐aged women, appearing as smooth‐edged lesions with or without septa, often featuring peripheral eggshell calcifications. IPMN presents as pleomorphic cystic masses communicating with the main pancreatic duct, which is key to diagnosis. Beyond these, numerous other less common pancreatic tumors present as cystic lesions. These include pancreatic solid pseudopapillary neoplasms, cystic neuroendocrine tumors, cystic degeneration of other solid tumors, and extremely rare cystic acinar cell tumors, ductal tubular neoplasms, hemangiomatous tumors, lymphoepithelial cysts, and a few other mesenchymal‐derived tumors.
Preoperative clinical evaluation strongly suggested the pancreatic serous cystadenoma, though a definitive diagnosis was not established. Additionally, the patient experienced significant psychological distress and expressed a strong desire for surgery. Indeed, patients should be advised to undergo Endoscopic Ultrasound‐guided Fine Needle Aspiration (EUS‐FNA) in accordance with the guidelines. Our clinicians also made this recommendation. However, due to the uncertainty and risk of diagnosis of EUS‐FNA, and the patient's unwillingness to refer to a higher hospital and bear the additional costs of EUS‐FNA, she rejected this suggestion and chose direct surgery. At the patient's request and after the surgical contraindications were ruled out, a laparoscopic pancreaticoduodenectomy was performed.
Conclusion and Results (Outcome and Follow‐Up)
4
A solid mass in the pancreatic head was observed on the postoperative autopsy specimen, and the mass appeared gray and white on the cut surface. Postoperative light microscopy showed that the mass consisted of dilated blood vessels of different diameters, and it was considered a tumor of vascular origin in the head of the pancreas, most likely a cavernous hemangioma (Figure 3A). Immunohistochemical staining showed: CD31(+), CD34(+), SMA(+), D2‐40(−), Ki‐67(−) (Figure 3B–F). The final postoperative pathological diagnosis was cavernous hemangioma. The patient had no complications during the clinical follow‐up 4 months after surgery. No signs of recurrence or metastasis were found on CT examination of the upper abdomen.
Postoperative light microscopy showed that the mass consisted of dilated blood vessels of different diameters, and it was considered a tumor of vascular origin in the head of the pancreas, mostly cavernous hemangioma (A). Immunohistochemical staining showed: CD31(+; B), CD34(+; C), SMA(+; D), D2‐40(−; E), Ki‐67(−; F), supporting the diagnosis of cavernous hemangioma.
Discussion
5
Since 1939, a total of 30 reports of pancreatic hemangioma have been retrieved from PubMed. In addition to our report this time, a total of 34 cases (Table 1) of pancreatic hemangioma were analyzed [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32]. According to these cases, like other hemangiomas, pancreatic hemangiomas were also more common in women (26 cases in this series, 76.5%), with a male to female sex ratio of 1.0:3.3. The most common symptom remains abdominal pain (21/34, 61.8%), which usually occurs in the upper abdomen and sometimes radiates to the back. Other associated symptoms include low back pain, bloating, nausea, and vomiting, all caused by the tumor pressing on surrounding organs. Others were incidental clinical findings or physical examination findings.
Diagnostic imaging of pancreatic hemangioma is mostly confirmed by CT (27/34, 79.4%), followed by US or endoscopic US (EUS) (20/34, 58.8%), and MRI applied in recent cases (16/34, 47.17%). Other imaging tests such as angiography, endoscopy, endoscopic retrograde cholangiopancreatography (ERCP), abdominal plain film, cholangiography, and PET may also be found in a few cases. The site of the disease was most commonly located in the head of the pancreas (18/34, 52.9%), followed by the body‐tail (6/34, 17.6%), tail (5/34, 14.7%), body (4/34, 11.8%), and pancreatic neck (1/34, 2.9%). The maximum diameter of the lesion ranged from 0.5 to 20.0 cm. Under US examination, pancreatic hemangioma appeared as a hyperechoic mass with no or low velocity venous flow signal, which contrasts with the adequate blood supply of malignant tumors. On US, the hemangioma may show rapid enhancement but the clearance speed is slow, forming an obvious “fast in, slow out” sign [6, 7, 8, 11, 14, 15, 17, 18, 21, 23, 24, 25, 28, 29, 30, 31]. Since the patient in this case did not undergo US in our hospital, we were not able to observe this presentation. By CT and MRI, the tumor was usually presented as a classically rounded, well‐defined, and low‐density mass with a multilocular or honeycomb shape and no dilatation of the main pancreatic duct [6, 7, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32]. In addition, some pancreatic hemangiomas reported in the literature presented as highly vascular masses, usually showing strong enhancement in the arterial phase of enhanced images. However, this finding was not confirmed in our case or in some other cases. The reason for this may be the lack of larger supplying vessels, slow blood flow within the tumor, and the absence of significant arteriovenous shunting, which may result in a low degree of enhancement. Also, there were different proportions of cystic and solid components in the tumor, which may lead to varying degrees of enhancement in the arterial phase [7, 8, 9, 27, 31]. Furthermore, in patients with pancreatic hemangioma, only a very small number of patients would show characteristic changes, and the vast majority of imaging diagnoses are difficult. Therefore, it is easy to confuse it with other pancreatic lesions (e.g., pseudocysts, serous cystadenomas, mucinous cystadenomas, and IPMN). However, through our case and review of the literature, the diagnosis of hemangioma cannot be excluded when imaging reveals a multilocular cystic tumor of the pancreas without invasion of adjacent structures, obstruction of the main pancreatic duct or other signs of malignancy such as lymph node metastasis, and enhancement is not significant. Pre‐surgical imaging is still essential to provide some indication and to rule out the malignancy of the lesion. If malignancy can be safely ruled out, the decision to operate must be based on a risk–benefit analysis. In some cases, close observation and regular follow‐up may be more beneficial.
Currently, the gold standard for the diagnosis of pancreatic hemangioma remains pathologic examination. Microscopically, hemangiomas consist predominantly of dilated abnormal sinus nodes lined with a single layer of vascular endothelial cells, which are not completely spaced by fibrous tissue forming spongy structures. Depending on the size of the vascular space, they can be capillary or spongy. On immunohistochemistry, CD31 and CD34 positivity indicates hemangiomas, lymphangiomas, and other benign vascular tumors, and the lymphatic endothelial marker D2‐40 negativity and lymphocyte deficiency help to rule out lymphangiomas [22, 27, 31]. Unlike the established observations for pediatric hemangioma, there are no definitive standards for the treatment of pancreatic hemangiomas in adults. However, surgical resection is usually recommended due to its risk of sudden bleeding and the uncertain differential diagnosis with epithelial tumors [23, 31]. The choice of surgical approach is based primarily on the location of the pancreatic hemangioma and is also influenced by the size of the tumor. So far, no cases of recurrence or metastasis have been found. Most patients achieved good clinical outcomes after surgical treatment.
In conclusion, pancreatic hemangioma in adults is a rare benign tumor without specific clinical symptoms and lacks typical imaging manifestations. Diagnosis is usually made postoperatively through histologic examination and immunohistochemical studies. However, careful evaluation of imaging characteristics through CT and MRI, combined with US and laboratory examination results, can provide valuable information for diagnosing pancreatic hemangioma and guiding management or treatment decisions.
Author Contributions
Jing Zhang: conceptualization, data curation, formal analysis, resources, writing – original draft, writing – review and editing. Jingjing Chen: data curation, formal analysis, supervision. Dongmei Zou: data curation, formal analysis. Xu Cao: supervision, visualization, writing – review and editing.
Funding
The authors have nothing to report.
Ethics Statement
This study was performed in line with the principles of the Declaration of Helsinki.
Consent
The patient gave her written informed consent for the publication of any identifying information/images in this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Jeong , S. B. Park , E. J. Lee , M. K. Kim , H. J. Park , and E. Lee , “Intranodal Hemangioma in the Pelvic Cavity: A Case Report,” Current Medical Imaging 16, no. 9 (2020): 1182–1184.33135609 10.2174/1573405616666200106143456 · doi ↗ · pubmed ↗
- 2J. Le Borgne , L. de Calan , and C. Partensky , “Cystadenomas and Cystadenocarcinomas of the Pancreas: A Multiinstitutional Retrospective Study of 398 Cases,” French Surgical Association. Annals of Surgery 230, no. 2 (1999): 152–161.10450728 10.1097/00000658-199908000-00004 PMC 1420857 · doi ↗ · pubmed ↗
- 3V. Ranstrom , “Haemangioma Cavernosum Pancreatitis (In German),” Zentralblatt Für Allgemeine Pathologie and Pathologische Anatomie 73 (1939): 33–35.
- 4S. Ringoir , F. Derom , R. Colle , and G. Mortier , “Hemangioma of the Pancreas. Report of a Case,” Gastroenterology 41 (1961): 43–45.13741765 · pubmed ↗
- 5F. Colardyn , A. Elewaut , E. Van de Velde , and F. Barbier , “Hemangioma of the Pancreas,” Tijdschrift Voor Gastro‐Enterologie 15, no. 4 (1972): 260–267.4642101 · pubmed ↗
- 6P. Mangin , M. Perret , and A. Ronjon , “Hemangioma of the Pancreas,” Journal de Radiologie 66, no. 5 (1985): 381–384.4032348 · pubmed ↗
- 7H. Kobayashi , T. Itoh , R. Murata , and M. Tanabe , “Pancreatic Cavernous Hemangioma: CT, MRI, US, and Angiography Characteristics,” Gastrointestinal Radiology 16, no. 4 (1991): 307–310.1936772 10.1007/BF 01887375 · doi ↗ · pubmed ↗
- 8J. Dageförde , E. Gmelin , and M. Otte , “Hemangioma of the Pancreas,” Ro Fo: Fortschritte Auf Dem Gebiete der Rontgenstrahlen Und der Nuklearmedizin 154, no. 3 (1991): 332–333.1849305 10.1055/s-2008-1033142 · doi ↗ · pubmed ↗