A novel application of the submucosal tunnel technique for resection of a giant duodenal lipoma
Jingjing Lian, Aiping Xu, Tao Chen, Meidong Xu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
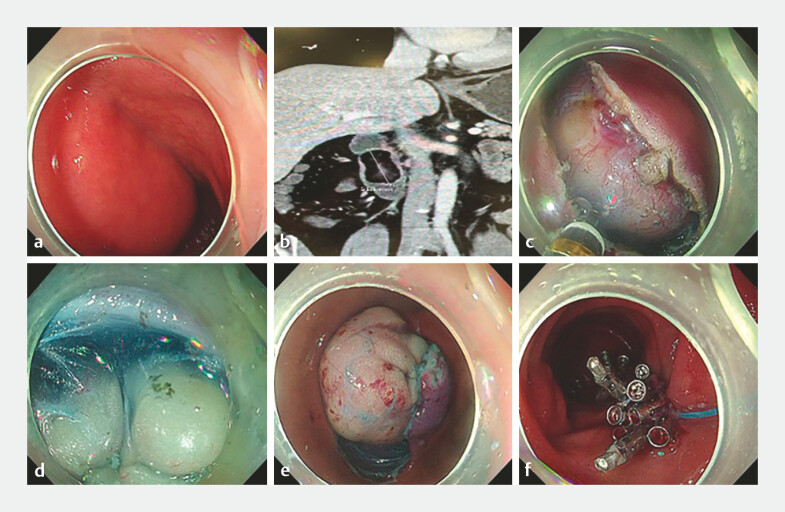 Fig. 1
Fig. 1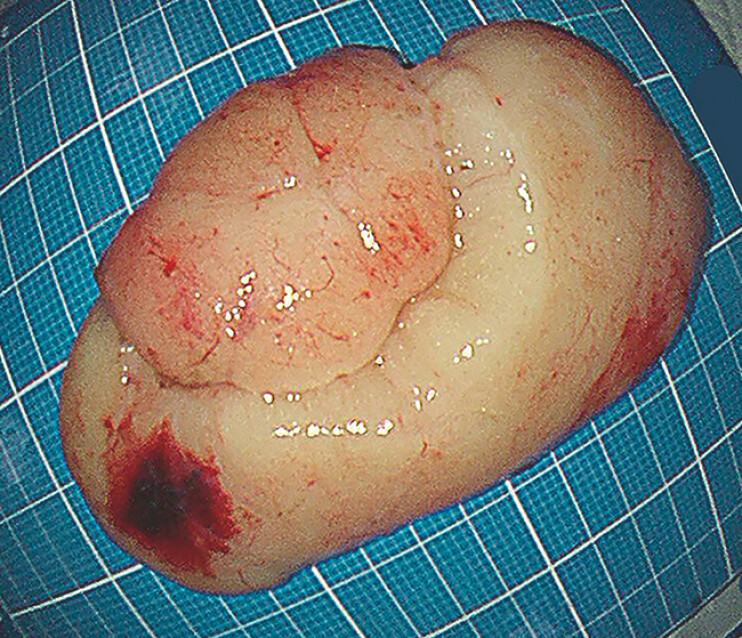 Fig. 2
Fig. 2- —Medical Discipline Construction Project of Pudong Health Committee of Shanghai
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Tumors and Oncological Cases
A 47-year-old male was admitted for investigation of melena. Esophagogastroduodenoscopy revealed a large, smooth, submucosal mass in the descending duodenum ( Fig. 1 a ). The patient underwent endoscopic ultrasound and abdominal magnetic resonance imaging (MRI) for further characterization of the duodenal mass. Both studies were unequivocally consistent with a submucosal lipoma ( Fig. 1 b ). The lesion was estimated to be >5 cm in the greatest diameter.
Endoscopic resection of a giant duodenal lipoma using a submucosal tunnel technique. a Endoscopic view of the large, submucosal mass in the descending duodenum. b Axial abdominal MRI findings of the duodenal lipoma. c A horizontal mucosal incision was made at the proximal edge of the tumor. d Submucosal dissection was performed, creating a tunnel above the yellow fatty tissue of the lipoma. e The tumor was gradually extruded into the lumen. f The mucosal entry site was closed with endoclips and secured with a nylon loop.
Given the symptomatic nature of the lesion, endoscopic resection was indicated. Prior to dissection, we introduced a side-viewing duodenoscope to repeatedly verify that the lesion was unrelated to the papilla.
However, due to its enormous size and broad base, a standard ESD was deemed high-risk, as the resulting defect would be massive and impossible to close securely, posing a significant risk of perforation. We here presented a novel application of submucosal tunnel resection, allowing for en-bloc removal while preserving the overlying mucosa. The steps were as follows ( Video 1 , Fig. 1 ): First, a 3-cm horizontal mucosal incision was made at the oral (proximal) edge of the tumor following submucosal injection ( Fig. 1 c ). Then, the submucosal layer was dissected carefully above the tumor capsule to create a tunnel and the dissection was advanced distally between the mucosal layer and the tumor mass ( Fig. 1 d ). As dissection proceeded, the tumor was gradually extruded into the lumen ( Fig. 1 e ). Next, the final connection was cut, and the tumor was immediately captured and retrieved en-bloc with a snare. Finally, the mucosal incision site and the small residual defect were closed with endoclips and finally secured with a nylon loop ( Fig. 1 f ). The resected specimen measured 7.0 cm × 4.0 cm ( Fig. 2 ).
The process of endoscopic resection of a giant duodenal lipoma.Video 1
The resected lipoma specimen measuring 7.0 cm × 4.0 cm.
The patient recovered uneventfully, was started on a clear liquid diet on postoperative day 2, and was discharged on day 4. Pathological examination confirmed the diagnosis of a lipoma.
To our knowledge, this is the first report of a submucosal tunnel technique being used for a large duodenal lesion. It represents a valuable addition to the therapeutic endoscopist's arsenal for managing complex SMTs in this challenging anatomical location.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ