Successful endoscopic management of post-coloplasty cervical esophagocutaneous fistula using sequential diabolo and fully covered stents
Abdeldjalil Sais, Jérôme Rivory, Florian Rostain, Alexandru Lupu, Marius Baldir, Jean Grimaldi, Mathieu Pioche

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
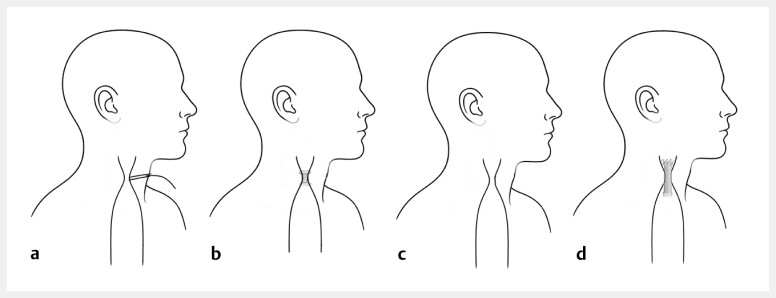 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Dysphagia Assessment and Management · Esophageal Cancer Research and Treatment
A 23-year-old woman with a complex psychiatric history—including multiple suicide attempts and ingestion of caustic agents—presented after deliberate ingestion of 200 mL of corrosive liquid. Initial computed tomography and emergent upper endoscopy revealed necrosis of the esophageal mucosa and extensive gastric injury. She underwent total esogastrectomy with cervical esophagostomy and jejunostomy feeding.
Over the following months, she developed a severe, recurrent stenosis of the cervical esophagostomy, causing salivary obstruction, aspiration, and repeated respiratory complications. Several retrograde endoscopic dilatations (4–11 mm) were performed using biliary balloons, allowing only partial functional improvement.
She underwent retrosternal coloplasty with cervical colo-esophageal anastomosis to restore continuity. The postoperative course was complicated by an anastomotic dehiscence, resulting in a large cervical esophagocutaneous fistula and complete stenosis of the colonic conduit. Surgical revision with the placement of a T-tube drain was required ( Fig. 1 ).
Endoscopic management of a post-coloplasty cervical fistula and stricture. a Cervical esophagocutaneous fistula with a T-tube drain. b Placement of a short diabolo stent for the fistula sealing and stricture support. c Fistula closed with the persistent severe stricture. d A fully covered esophageal stent fixed with sutures to prevent migration.
Endoscopic management of a post-coloplasty cervical esophagocutaneous fistula, using a diabolo stent for fistula, followed by a fully covered esophageal stent secured with endoscopic sutures.Video 1
Re-evaluation showed persistent fistula output and worsening dysphagia. Endoscopy demonstrated a tight anastomotic stricture with direct communication to the cervical cutaneous cavity. The T-tube was removed and a 40-mm × 16-mm “diabolo” stent was placed to simultaneously cover the fistula tract and support the anastomosis ( Video 1 ). Four weeks later, follow-up endoscopy confirmed the complete closure of the fistula but persistent anastomotic stenosis. The diabolo stent was removed, and a fully covered 24-mm × 110-mm esophageal stent was deployed and endoscopically sutured with SutuArt (Olympus) to prevent migration.
At a 2-month follow-up and after removing the fully covered stent, imaging and endoscopic assessment confirmed a healed fistula and stable anastomosis.
This case illustrates that the sequential placement of a diabolo stent followed by a sutured fully covered stent can allow the effective management of complex cervical post-coloplasty fistulas and strictures, avoiding further surgical intervention 1 2 3 .
Endoscopy_UCTN_Code_TTT_1AO_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oprisanescu D Bucur D Sandru V Endoscopic treatment of benign esophageal fistulas using fully-covered metallic esophageal stents Chirurgia (Bucur)201811310811510.21614/chirurgia.113.1.10829509537 · doi ↗ · pubmed ↗
- 2van Boeckel PGA Dua KS Weusten BLAM Fully covered self-expandable metal stents (SEMS), partially covered SEMS and self-expandable plastic stents for the treatment of benign esophageal ruptures and anastomotic leaks BMC Gastroenterol 2012121922375711 10.1186/1471-230X-12-19PMC 3313862 · doi ↗ · pubmed ↗
- 3Wu G Yin M Zhao YS Novel esophageal stent for treatment of cervical anastomotic leakage after esophagectomy Surg Endosc 2017315024503110.1007/s 00464-017-5545-628432462 · doi ↗ · pubmed ↗