Rescue endoscopic ultrasound-guided hepaticogastrostomy with antegrade stenting for food-impacted complete papillary occlusion via intentional stent-mesh traversal
Hidenobu Hara, Hikari Ishii, Risa Katsumata, Tomohisa Ashikawa, Kazuomi Sakaki, Kouhei Yoshino, Shinya Sakita

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
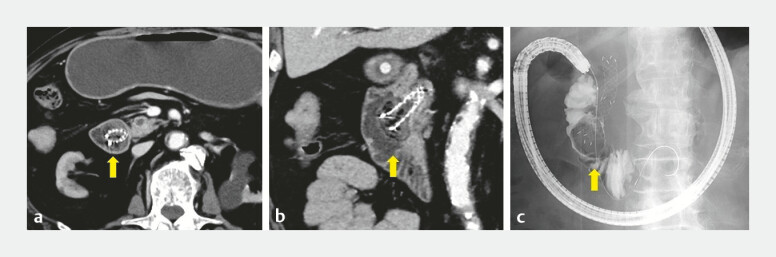 Fig. 1
Fig. 1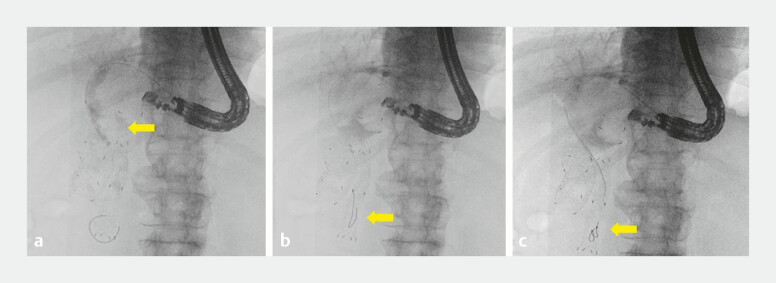 Fig. 2
Fig. 2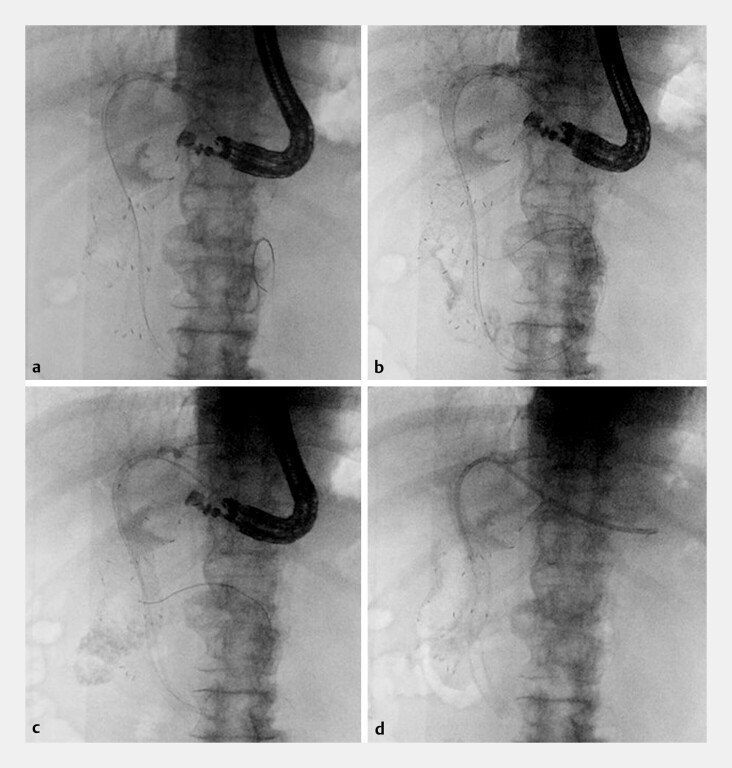 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Organ Transplantation Techniques and Outcomes
Endoscopic ultrasound (EUS)-guided hepaticogastrostomy with antegrade stenting (EUS-HGAS) provides durable drainage when transpapillary access is not feasible 1 2 , but complete papillary occlusion can prevent guidewire passage. We report a rescue case in which a double-guidewire technique 3 4 enabled intentional traversal of the stent mesh to complete EUS-HGAS.
A 91-year-old man with pancreatic cancer previously underwent endoscopic retrograde cholangiopancreatography, with the placement of a 10-mm self-expanding metal stent (SEMS) of multi-hole design; a duodenal SEMS was later placed for malignant obstruction. Computed tomography (CT) and contrast studies showed food residue around the papilla, forming an obstructive mass ( Fig. 1 ). The patient developed acute cholangitis, and rescue EUS-HGAS was planned ( Video 1 ).
Preprocedural imaging demonstrating a food-impacted papilla with complete obstruction. a Axial CT shows dense intraluminal food impacted at the periampullary segment (arrow). b Coronal CT confirms the food residue abutting the papilla (arrow). c Fluoroscopic duodenography demonstrates a filling defect with contrast hold-up at the papilla (arrow). CT, computed tomography.
Bypassing a food-impacted papilla via intentional stent-mesh traversal.Video 1
The left intrahepatic duct (B3) was punctured with a 19-gauge FNA needle, and a 0.025-inch guidewire was advanced into the intrahepatic duct. Cholangiography confirmed the intraductal position, and a tapered catheter was inserted. Contrast demonstrated hilar obstruction ( Fig. 2 a ). Repeated attempts to cross the papilla with a guidewire failed ( Fig. 2 b ), and catheter advancement was impeded by the indwelling stent. A double-lumen cannula enabled a double-guidewire technique with advancement toward the peripapillary segment; yet, crossing remained impossible ( Fig. 2 c ). We elected intentional traversal through the stent mesh. The leading-lumen wire crossed the mesh of SEMS ( Fig. 3 a ); after failed catheter tracking, reintroduction of the tapered catheter permitted successful mesh traversal. Contrast confirmed the intraduodenal position ( Fig. 3 b ). Two uncovered SEMSs (8 × 80 mm and 8 × 60 mm) were deployed in series toward the papillary side to restore luminal continuity ( Fig. 3 c ). The HGS fistula was not dilated to minimize the bile-leak risk, and a plastic stent (7 F, 15 cm) was placed from the hepatic duct into the HGS tract ( Fig. 3 d ). No complications occurred on clinical/CT follow-up.
Cholangiography and guidewire attempt before mesh traversal. a Cholangiography demonstrates a hilar obstruction. b Guidewire passage across the papilla is impeded by food impaction (arrow). c A double-guidewire technique was used to attempt the traversal of the impaction, but crossing remained unsuccessful (arrow).
Intentional stent-mesh traversal and completion of rescue EUS-guided hepaticogastrostomy with antegrade stenting (EUS-HGAS). a The guidewire intentionally traverses the mesh of the pre-existing transpapillary self-expandable metallic stent (SEMS) and is positioned on the duodenal side. b The catheter crosses the SEMS mesh; contrast injection confirms intraduodenal positioning. c Two uncovered SEMSs are deployed in series from the duodenum toward the hilar segment to restore luminal continuity. d A plastic stent is placed across the HGS fistula to secure the hepaticogastrostomy fistula.
To our knowledge, this is the first report of rescue EUS-HGAS overcoming complete papillary occlusion from food impaction around a pre-existing SEMS by stent-mesh traversal.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ishiwatari H Ogura T Hijioka SEUS-guided hepaticogastrostomy versus EUS-guided hepaticogastrostomy with antegrade stent placement in patients with unresectable malignant distal biliary obstruction: a propensity score-matched case-control study Gastrointest Endosc 2024100667538382887 10.1016/j.gie.2024.02.012 · doi ↗ · pubmed ↗
- 2Moond V Loganathan P Koyani B Efficacy and safety of EUS-guided hepatogastrostomy: a systematic review and meta-analysis Endosc Ultrasound 20241317118210.1097/eus.000000000000005539318645 PMC 11419430 · doi ↗ · pubmed ↗
- 3Ishiwatari H Satoh T Sato J Double-guidewire technique facilitates endoscopic ultrasound-guided biliary drainage for hilar biliary obstruction Endoscopy 201951 E 321E 32210.1055/a-0915-191731163486 · doi ↗ · pubmed ↗
- 4Nakai Y Oyama H Kanai S Double guidewire technique using an uneven double lumen catheter for endoscopic ultrasound-guided interventions Dig Dis Sci 2021661540154710.1007/s 10620-020-06345-932436121 · doi ↗ · pubmed ↗