Primary Subcutaneous Hydatid Cyst of the Abdominal Wall in a Child: A Case Report and Literature Review
Hafid Talha

TL;DR
A rare case of a subcutaneous hydatid cyst in a child's abdominal wall is reported, highlighting the need to consider this condition in endemic regions.
Contribution
This case report adds to the limited literature on primary subcutaneous hydatid cysts in children without associated visceral disease.
Findings
The cyst was completely excised without complications and treated with albendazole.
Literature review found very few pediatric cases of subcutaneous hydatid cysts without visceral involvement.
The case emphasizes the importance of considering hydatid disease in subcutaneous masses in endemic areas.
Abstract
Hydatid disease is a parasitic infection that can affect almost any organ, with a clear predominance for the liver and lungs, while primary involvement of subcutaneous tissue is exceptionally rare. We report the case of an eight-year-old boy from an endemic region who presented with a slowly growing, painless mass in the right iliac fossa, without systemic symptoms. Ultrasound revealed a well-defined, purely cystic lesion consistent with a Gharbi type I hydatid cyst. Thoracoabdominal CT scan showed no additional hydatid localizations, particularly in the liver or lungs. The lesion was completely excised through a right iliac fossa approach without intraoperative complications, and albendazole therapy was administered. A review of the literature identified only a small number of abdominal wall hydatid cysts located in the subcutaneous tissue, with very few paediatric cases and most…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
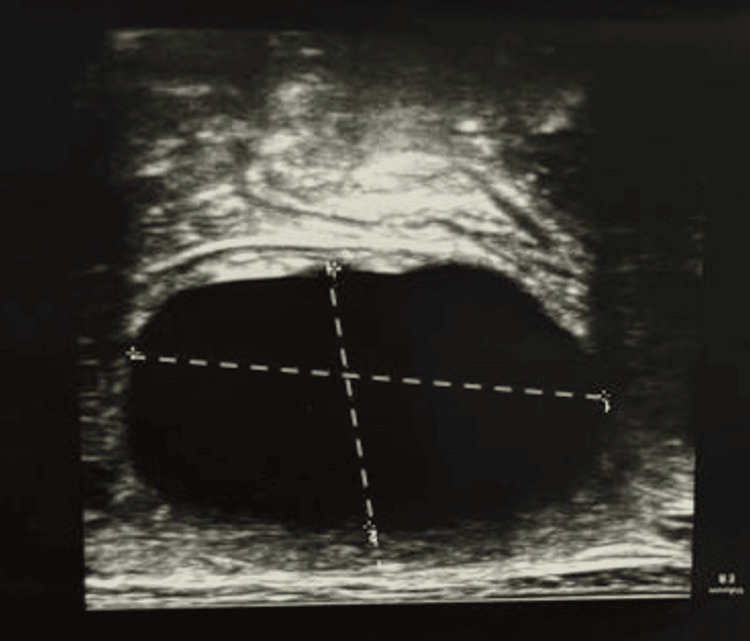 Figure 1
Figure 1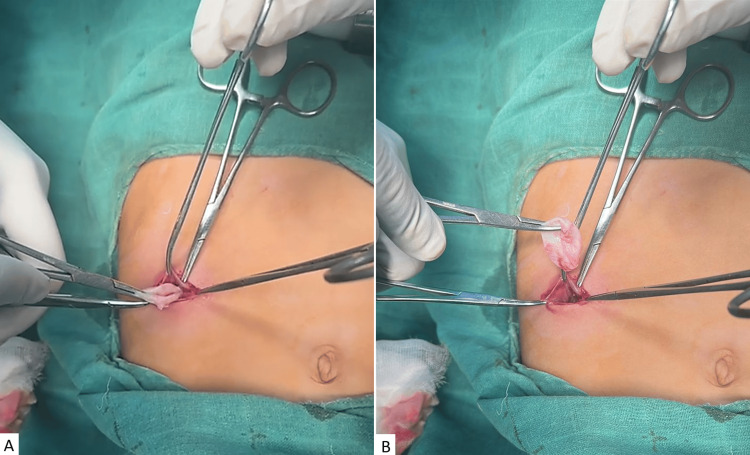 Figure 2
Figure 2| Parameters | Patient’s results | Reference values |
| Hemoglobin (g/dL) | 13.2 | 13–17 |
| White blood cells (×10⁹/L) | 7.4 | 4.0–10.0 |
| Neutrophils (%) | 62 | 40–75 |
| Platelets (×10⁹/L) | 260 | 150–400 |
| C-reactive protein (mg/L) | 6 | < 5 |
| Creatinine (mg/dL) | 0.9 | 0.6–1.2 |
| Urea (mg/dL) | 24 | 15–45 |
| Sodium (mmol/L) | 139 | 135–145 |
| Potassium (mmol/L) | 4.2 | 3.5–5.0 |
| Aspartate aminotransferase (U/L) | 22 | < 35 |
| Alanine aminotransferase (U/L) | 25 | < 45 |
| Glucose (g/dL) | 0.9 | 0.7–1 |
| Prothrombin activity (%) | 95 | 70-100 |
| Case Report | Age/sex | Location | Dissemination | Primary/Other disease |
| Ousadden et al. [ | 70 F | Para-umbilical abdominal wall | Isolated | Complete surgical removal of the cyst |
| Gulmez et al. [ | 60 F | Left periumbilical region of the abdominal wall | Isolated | Complete surgical removal of the cyst |
| Patmano et al. [ | 45 M | Right upper quadrant of abdominal wall | Isolated | Complete surgical removal of the cyst |
| El Haissoufi et al. [ | 6 M | Right posterolateral abdominal wall | Associated to lung hydatid disease | Surgical excision of the cyst + albendazole therapy |
| Bedioui et al. [ | 70 F | Hypogastric region | Isolated | Complete surgical removal of the cyst |
| Present case | 8 M | Right iliac fossa | Isolated | Complete surgical excision of the cyst + albendazole therapy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Head and Neck Anomalies · Parasite Biology and Host Interactions
Introduction
Hydatid disease is a parasitic infection that can involve almost any organ of the human body, although the liver and lungs are most frequently affected, while other sites, such as the subcutaneous tissue, are rarely encountered [1]. Pastoral and poor rural areas, where people keep livestock in close proximity to dogs, are the most affected regions [2].
The liver and lungs act as natural mechanical filters for parasitic oncospheres, making it difficult for the parasite to reach atypical locations without primary involvement of these organs [1]. Solitary primary subcutaneous localization is therefore very rare, and its exact incidence remains unknown [3]. The diagnosis of hydatid disease relies on imaging and serological investigations [4]. Surgery remains the preferred therapeutic modality; however, recurrences are frequent following resection [5].
Herein, we report the case of an eight-year-old boy with hydatid disease of the anterior abdominal wall, confined to the subcutaneous tissue and without primary hepatic or pulmonary involvement, who was successfully treated with complete surgical excision.
Case presentation
An eight-year-old boy presented with a slowly growing, painless mass in his right iliac fossa, without associated fever. The parents reported a history of contact with dogs. Initial ultrasound examination showed a fluid-filled cystic lesion without solid components, measuring 5x4.5x4cm consistent with a stage I cyst according to the Gharbi classification [6] (Figure 1). A complete imaging workup with a thoracoabdominal CT scan did not reveal any additional hydatid localizations, particularly in the lungs or liver. Admission laboratory results were within normal range and are summarized in Table 1.
Ultrasound findings of the abdominal lesion.Ultrasound of the abdominal lesion showing a purely cystic lesion with no solid components or membranous structures, consistent with a stage I hydatid cyst of Gharbi classification.
A hydatid cyst was strongly suspected, and the lesion was surgically excised without intraoperative complications. The operative field was first isolated with pads soaked in a scolicidal agent, followed by cyst puncture and controlled aspiration using a trocar aspirator to minimize spillage. After evacuation, the puncture orifice was enlarged to allow exposure of the cyst cavity, and the hydatid membrane was gently grasped and extracted without rupture (Figure 2).
Intraoperative photographs showing removal of the cyst through a right iliac fossa incision (A and B).
No postoperative complications were detected. The patient received albendazole therapy; preoperative albendazole was administered as adjuvant therapy (10-15 mg/kg/day in two doses) prior to surgery to reduce cyst viability and the risk of recurrence/spillage. At the one-year follow-up, the patient remained asymptomatic, with no clinical or radiological signs of recurrence.
Discussion
Hydatidosis is a zoonosis caused by Echinococcus granulosus, a cestode belonging to the family Taeniidae [7]. Hydatid disease is considered a major public health problem, particularly in developing countries [8]. It remains endemic in regions where livestock raising is common, including Mediterranean countries, the Middle East, India, Oceania, and South America [9]. Humans act as accidental intermediate hosts, with transmission occurring via orofecal contamination. After intestinal absorption, Echinococcus larvae cross the intestinal wall and reach the liver and other organs through the portal circulation [2].
The liver and lungs are the most frequently affected sites of hydatid cysts. Other locations, including the kidneys, spleen, bones, and brain, are less commonly affected [8]. Although hydatid disease can theoretically involve any organ, primary hydatid cysts arising in soft tissues such as the subcutaneous tissue, without concomitant hepatic or pulmonary involvement, are exceedingly uncommon [2]. The reported incidence of subcutaneous hydatid cysts is approximately 2% of all hydatid cysts, and most of these are associated with liver and/or lung disease; primary subcutaneous hydatid cysts are therefore exceedingly rare [9]. Patmano et al. reported only one abdominal wall localization among eight subcutaneous hydatid cysts in their series [10].
In our review of the literature, we identified several dozen subcutaneous localizations, including both isolated and disseminated forms. However, to the best of our knowledge, only five cases have described a similar localization to ours, in the subcutaneous tissue of the abdominal wall; among these, just one involved a pediatric patient (Table 2). Notably, that pediatric case was associated with primary pulmonary disease, in contrast to our patient, who presented with an isolated subcutaneous abdominal wall hydatid cyst.
Passage of the parasite from the portal vein into the systemic circulation is difficult because of the well-developed capillary networks of the liver and lungs, which act as an effective filter [2]. The exact mechanisms underlying primary hydatid cysts, outside the liver and lungs, at rare sites, including the abdominal wall, remain unclear. The most widely accepted hypothesis is subcutaneous colonization by ingested eggs after they have traversed the hepatic and pulmonary filters [8]. A small number of ova may pass through the liver and reach the lungs and systemic circulation, thereby causing hydatid disease in other organs [4]. Alternatively, parasites may bypass the portal-liver filter by using lymphatic pathways or venous shunts to gain direct access to the systemic circulation [8]. Direct extension from adjacent organs represents another possible mechanism for involvement of unusual sites [4].
The most common clinical manifestation is a painless, slowly growing mass without inflammatory signs [13], with a wide range of nonspecific symptoms that are largely related to the localization and size of the cyst [9]. The diagnosis of hydatid cyst is based mainly on imaging modalities, including ultrasonography, CT scan, and magnetic resonance imaging (MRI), together with serological tests (e.g., indirect hemagglutination and enzyme-linked immunosorbent assay (ELISA)), which may be used; however, negative serology does not exclude hydatid disease. Therefore, serological testing was not performed in our case.
In some cases, the diagnosis is only confirmed by preoperative biopsy or on postoperative histopathological examination [8]. MRI provides a detailed assessment of soft tissue structures and the degree of extension [2]. Imaging also helps determine the stage of the hydatid cyst and to exclude differential diagnoses. In subcutaneous locations, the differential diagnosis includes other soft tissue masses, mainly abscesses, dermal and epidermal cysts, and lipomas [9]. Preoperative recognition of hydatid cysts is crucial, as the condition must be distinguished from other entities with similar presentations [2]. Diagnosis may be particularly challenging when classical sites such as the liver and lungs are not involved and when epidemiological risk factors are absent.
Complete surgical excision of the cyst is the treatment of choice in the majority of cases [8], considering the exact site of the lesion, the proximity of critical structures, and any systemic involvement [2]. Surgical management carries specific risks, primarily related to the operative procedure itself and to potential cyst rupture, which may result in anaphylaxis, dissemination, and local recurrence [8]. When the complete resection of the cyst is not possible, all the cyst content should be carefully evacuated [9].
Percutaneous approaches have also been reported as effective treatment options for hydatid cysts of the lungs, kidneys, orbit, and parotid glands [8]. Other management strategies include aspiration followed by injection of a scolicidal agent and re-aspiration, systemic albendazole therapy, and surveillance in selected cases [2]. However, benzimidazoles appear to be less effective in muscle and renal hydatid cysts because of their low concentrations within cyst fluid [1].
In our case, the cyst was managed surgically, with no perioperative complications and no evidence of recurrence at the one-year follow-up.
Conclusions
Hydatid disease remains a common parasitic infection that should be considered in the differential diagnosis of any subcutaneous mass, particularly in patients from endemic regions. Radiological assessment of the liver and lungs is essential to detect disseminated disease. The treatment of choice is complete surgical excision of the cyst to minimize the risk of recurrence. Through this case, we aim to raise awareness of hydatid disease and highlight that unusual subcutaneous localizations may occur even in the complete absence of hepatic or pulmonary involvement.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hydatid cysts in muscle: a modified percutaneous treatment approach Int J Infect Dis Ormeci N Idilman R Akyar S Palabiyikoğlu M Coban S Erdem H Ekiz F 2042081120071681458610.1016/j.ijid.2005.10.015 · doi ↗ · pubmed ↗
- 2Primary hydatid cyst of skeletal muscle: a rare clinical entity Int J Surg Case Rep Ismail A Haider SM Fatima U Ismail MS Butt UI 11110612820254004340710.1016/j.ijscr.2025.111106 PMC 11925152 · doi ↗ · pubmed ↗
- 3Subcutaneous hydatid cysts occurring in the palm and the thigh: two case reports J Med Case Rep Dirican A Unal B Kayaalp C Kirimlioglu V 273220081870098310.1186/1752-1947-2-273PMC 2533018 · doi ↗ · pubmed ↗
- 4A solitary primary subcutaneous hydatid cyst in the abdominal wall of a 70-year-old woman: a case report J Med Case Rep Ousadden A Elbouhaddouti H Ibnmajdoub KH Mazaz K Aittaleb K 270520112172238610.1186/1752-1947-5-270PMC 3152916 · doi ↗ · pubmed ↗
- 5Surgical treatment of hepatic hydatid disease Br J Surg Dawson JL Stamatakis JD Stringer MD Williams R 946950751988321954010.1002/bjs.1800751004 · doi ↗ · pubmed ↗
- 6Ultrasound examination of the hydatic liver Radiology Gharbi HA Hassine W Brauner MW Dupuch K 4594631391981722089110.1148/radiology.139.2.7220891 · doi ↗ · pubmed ↗
- 7Primary hydatid cysts in the extremities: a systematic review of the literature Cureus Paspala A Mela E Vailas M 016202410.7759/cureus.63174 PMC 1127317639070504 · doi ↗ · pubmed ↗
- 8Echinococcal cyst of the subcutaneous tissue: a rare case report Parasitol Int Safioleas M Nikiteas N Stamatakos M Safioleas C Manti CH Revenas C Safioleas P 2362385720081820365510.1016/j.parint.2007.11.002 · doi ↗ · pubmed ↗