Ghana Heart Initiative Training for Cardiac Arrest Management Among Health Care Professionals: Outcomes Evaluation Study (2019-2024)
Alfred Doku, Lawrence Sena Tuglo, Chiedozie Osuoji, Juliette Edzeame, Marisa Broni, David Danso Mainoo, Alberta Ewuziwaa Acquah, Kwatetso Honny, Ron J G Peters, Charles Agyemang

TL;DR
This study evaluates how well healthcare professionals in Ghana learned and retained skills in basic and advanced cardiac life support after training from the Ghana Heart Initiative.
Contribution
The study provides empirical evidence on the effectiveness of BLS and ACLS training among healthcare professionals in Ghana.
Findings
74.6% of healthcare professionals had adequate BLS knowledge and skills after training.
Over 73.3% of participants demonstrated adequate ACLS knowledge and skills.
Healthcare professionals in primary facilities and certain regions performed better than those in tertiary facilities and other regions.
Abstract
Health care professionals must stay updated with the latest guidelines for basic life support (BLS) and advanced cardiac life support (ACLS) to effectively assist patients during cardiac emergencies. Since its launch in 2018, the Ghana Heart Initiative has significantly enhanced the skills and knowledge of health care professionals in managing cardiovascular diseases, including cardiac emergencies. This study aims to assess the knowledge and skills of BLS and ACLS among health care professionals immediately after training in Ghana. This cross-sectional, training-based study involved 541 and 302 health care professionals trained in BLS and ACLS, respectively. Among them, 229 BLS and 124 ACLS-trained participants completed the questionnaires immediately after the training, and their data were included in the final analysis. Knowledge was assessed using a standardized questionnaire and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
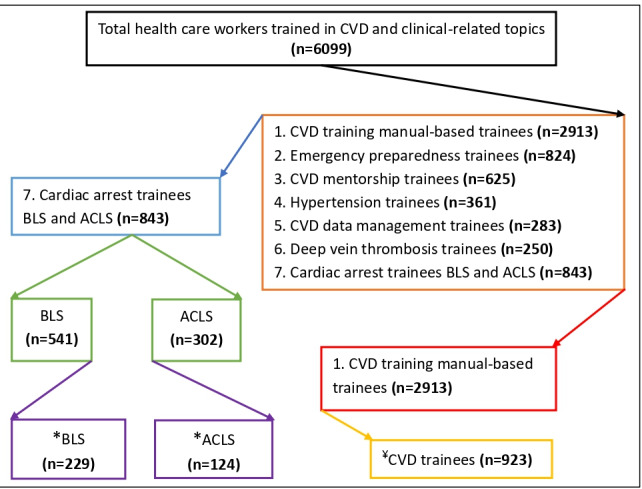 Figure 1
Figure 1| Variable | Total (N=229), n (%) | Basic life support knowledge score | |||||||||
|
|
| Adequate (n=171), n (%) | Inadequate (n=58), n (%) |
| |||||||
|
| .42 | ||||||||||
|
| Female | 152 (66.4) | 111 (64.9) | 41 (70.7) |
| ||||||
|
| Male | 77 (33.6) | 60 (35.1) | 17 (29.3) |
| ||||||
|
| .03a | ||||||||||
|
| Physician assistant/nurse | 86 (37.6) | 57 (33.3) | 29 (50) |
| ||||||
|
| HO/MO/SMOb | 36 (15.7) | 32 (18.7) | 4 (6.9) |
| ||||||
|
| Specialist/trainee specialist | 107 (46.7) | 82 (48) | 25 (43.1) |
| ||||||
|
| .008c | ||||||||||
|
| Primary | 64 (27.9) | 57 (33.3) | 7 (12.1) |
| ||||||
|
| Secondary | 110 (48) | 76 (44.4) | 34 (58.6) |
| ||||||
|
| Tertiary | 55 (24) | 38 (22.2) | 17 (29.3) |
| ||||||
|
| .03a | ||||||||||
|
| Ashanti | 29 (12.7) | 22 (12.9) | 7 (12.1) |
| ||||||
|
| Bono East | 25 (10.9) | 12 (7) | 13 (22.4) |
| ||||||
|
| Central | 25 (10.9) | 19 (11.1) | 6 (10.3) |
| ||||||
|
| Eastern | 23 (10) | 16 (9.4) | 7 (12.1) |
| ||||||
|
| Greater Accra | 60 (26.2) | 49 (28.7) | 11 (19) |
| ||||||
|
| Northern | 32 (14) | 23 (13.5) | 9 (15.5) |
| ||||||
|
| Volta/Oti | 35 (15.3) | 30 (17.5) | 5 (8.6) |
| ||||||
| Variable | UORa (95% CI) | AORb (95% CI) | ||||||
|
| ||||||||
|
| Physician assistant/nurse | 1.67 (0.89-3.14) | .11 | 1.45 (0.70-2.96) | .32 | |||
|
| House officer/medical officer/senior medical officer | 0.41 (0.13-1.27) | .12 | 0.47 (0.14-1.58) | .22 | |||
|
| Specialist/trainee specialist | Refc | Ref | Ref | Ref | |||
|
| ||||||||
|
| Primary | Ref | Ref | Ref | Ref | |||
|
| Secondary | 1.00 (0.50-2.02) | >.99 | 0.97 (0.44-2.12) | .94 | |||
|
| Tertiary | 0.26 (0.10-0.71) | .009 | 0.20 (0.07-0.59) | .003d | |||
|
| ||||||||
|
| Ashanti | 1.91 (0.54-6.82) | .32 | 1.16 (0.30-4.49) | .83 | |||
|
| Bono East | Ref | Ref | Ref | Ref | |||
|
| Central | 1.90 (0.51-7.08) | .34 | 1.48 (0.37-5.97) | .58 | |||
|
| Eastern | 2.63 (0.72-9.61) | .15 | 1.29 (0.30-5.50) | .73 | |||
|
| Greater Accra | 1.35 (0.43-4.26) | .61 | 0.95 (0.27-3.36) | .93 | |||
|
| Northern | 2.35 (0.69-7.96) | .17 | 1.48 (0.38-5.82) | .58 | |||
|
| Volta/Oti | 6.50 (1.90-22.23) | .003 | 4.94 (1.17-20.80) | .03e | |||
| Variable | Total (n=124), n (%) | Advanced cardiac life support knowledge score, n (%) | |||||||||
|
|
| Adequate (n=91) | Inadequate (n=33) |
| |||||||
|
| <.001a | ||||||||||
|
| Female | 51 (41.1) | 26 (28.6) | 25 (75.8) |
| ||||||
|
| Male | 73 (58.9) | 65 (71.4) | 8 (24.2) |
| ||||||
|
| .003b | ||||||||||
|
| Physician assistant/nurse | 4 (3.2) | 0 (0) | 4 (12.1) |
| ||||||
|
| House officer/medical officer/senior medical officer | 89 (71.8) | 68 (74.7) | 21 (63.6) |
| ||||||
|
| Specialist/trainee specialist | 31 (25) | 23 (25.3) | 8 (24.2) |
| ||||||
|
| .045c | ||||||||||
|
| Primary | 20 (16.1) | 12 (13.2) | 8 (16.1) |
| ||||||
|
| Secondary | 40 (32.3) | 26 (28.6) | 40 (32.3) |
| ||||||
|
| Tertiary | 64 (51.6) | 53 (58.2) | 64 (51.6) |
| ||||||
|
| .34 | ||||||||||
|
| Ashanti | 12 (9.7) | 10 (11) | 2 (6.1) |
| ||||||
|
| Bono East | 11 (8.9) | 8 (8.8) | 3 (9.1) |
| ||||||
|
| Central | 11 (8.9) | 5 (5.5) | 6 (18.2) |
| ||||||
|
| Eastern | 11 (8.9) | 9 (9.9) | 2 (6.1) |
| ||||||
|
| Greater Accra | 55 (44.4) | 39 (42.9) | 16 (48.5) |
| ||||||
|
| Northern | 12 (9.7) | 10 (11) | 2 (6.1) |
| ||||||
|
| Volta/Oti | 12 (9.7) | 10 (11) | 2 (6.1) |
| ||||||
| Variable | UORa (95% CI) | AORb (95% CI) | |||
|
| |||||
|
| Female | Refc | Ref | Ref | Ref |
|
| Male | 7.81 (3.12-19.54) | <.001 | 7.05 (2.69-18.46) | <.001d |
|
| |||||
|
| Physician assistant/nurse | —e | — | — | — |
|
| House officer/medical officer/senior medical officer | 0.89 (0.35-2.28) | .80 | 0.66 (0.22-1.98) | .46 |
|
| Specialist/trainee specialist | Ref | Ref | Ref | Ref |
|
| |||||
|
| Primary | 3.21 (1.06-9.70) | .04 | 2.96 (0.79-11.13) | .11 |
|
| Secondary | 2.59 (1.04-6.50) | .04 | 2.25 (0.80-6.30) | .12 |
|
| Tertiary | Ref | Ref | Ref | Ref |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Disaster Response and Management · Mechanical Circulatory Support Devices
Introduction
Cardiac arrest, the sudden and complete shutdown of heart function, causes both respiratory and circulatory failure [1]. It is a critical emergency that demands immediate action [1]. Most adult cardiac arrests occur suddenly mainly due to heart diseases or systemic issues such as electrolyte and acid-base imbalances [2]. Therefore, delivering chest compression is essential for maintaining blood flow [3]. Prompt initiation of cardiopulmonary resuscitation (CPR) is crucial because it temporarily preserves life by ensuring that sufficient blood reaches vital organs such as the brain and heart [4]. Knowledge and skills in basic life support (BLS) and advanced cardiac life support (ACLS) are vital for managing sudden cardiac arrest, myocardial infarction, foreign body airway obstructions, respiratory failure [3], and other serious cardiovascular diseases (CVDs) [5,6].
The American Heart Association (AHA) plays a crucial role in emergency cardiovascular care (ECC) by regularly updating the CPR and ECC guidelines [7,8]. These guidelines provide a standard approach for delivering BLS and ACLS to revive patients [7,8]. BLS, which involves a series of care given to patients experiencing respiratory arrest, cardiac arrest, or airway obstruction, is a fundamental part of these guidelines [9]. The BLS course, based on AHA guidelines, teaches participants how to quickly recognize life-threatening emergencies, perform effective chest compressions, provide proper ventilation, and use an automated external defibrillator [9]. Similarly, the ACLS, also based on AHA guidelines, includes recognizing signs of sudden cardiac arrest, myocardial infarction, and complete airway obstruction, as well as performing CPR and defibrillation with an automated external defibrillator [1]. Following these guidelines, ACLS and CPR, when administered promptly, have been shown to improve survival rates in medical emergencies [1].
As health care professionals play a vital role in emergency response, they are expected to possess a strong understanding of the basic resuscitation principles in patient care and stay updated with the BLS and ACLS guidelines for rescuing patients who are unconscious or in cardiac arrest. However, studies conducted in low-income countries such as South Africa [10], Afghanistan [2], and Pakistan [11] have reported limited BLS knowledge and skills among health care professionals. Additionally, research in Ethiopia [1] and Spain [4] has shown insufficient understanding of ACLS among health care professionals (nurses and doctors) and nurses, respectively. Unlike in high-income countries, where strict licensing or certification is required before practice, few studies [1,2,9,11,12] have evaluated the BLS and ACLS knowledge of health care professionals in low-income countries.
In Ghana, there are no strict licensing requirements for health care professionals to be trained in current BLS and ACLS guidelines or to obtain a certificate before practicing. However, through the Ghana Heart Initiative, some health care professionals in Ghana have received training in BLS and ACLS based on AHA-certified guidelines, filling this critical gap in the health system [13]. To our knowledge, no study has assessed the knowledge and skills in BLS and ACLS among health care professionals in Ghana. Therefore, this study aims to evaluate their knowledge and skills in BLS and ACLS through training, enabling them to manage cardiac arrest effectively in Ghana.
Methods
Study Setting and Recruitment
This study was conducted from 2019 to 2024 across 8 of Ghana’s 16 administrative regions. These include Ashanti, Bono East, Central, Eastern, Greater Accra, Northern, Volta, and Oti. Ghana, located in West Africa, is classified as a lower-middle-income country. Ghana borders the Gulf of Guinea and the Atlantic Ocean, sharing borders with Côte d'Ivoire to the west, Burkina Faso to the north, and Togo to the east [14]. As of 2021, Ghana had an estimated population of 33 million, covering approximately 238,535 square kilometers. Accra serves as the capital and functions as the country's economic and administrative center [14]. To ensure fair representation, proportional sampling was used to select 44 health facilities, including primary, secondary, and tertiary levels, as well as both public and quasi-governmental facilities. These included 6 health centers, 27 secondary facilities, 5 tertiary hospitals, and 6 community health planning and services facilities [15]. Written memos were sent to the administrators of the selected health facilities, requesting at least 1 health professional such as a physician assistant, nurse, house officer, medical officer, senior medical officer, specialist, or trainee specialist to participate in the training. The sessions took place in the capital cities of these regions at designated locations to encourage high attendance among health care professionals.
Study Design and Population
This study employs a cross-sectional, training-based design involving 541 and 302 health care professionals recruited from selected health facilities and trained in BLS and ACLS, respectively. Among them, 229 BLS and 124 ACLS-trained participants completed the questionnaires immediately after the training, and their data were included in the final analysis (Figure 1).
*Flow diagram of health care professionals trained in CVDs and clinical topics. Completed the BLS and ACLS training questionnaires and included in the final analysis. ¥The details of CVD trainees and the data are presented in a different study. ACLS: advanced cardiac life support; BLS: basic life support; CVD: cardiovascular disease.
BLS and ACLS training
BLS and ACLS training took place over 1 and 3 days, respectively, conducted by Code Red, a certified training provider experienced in AHA. The course guide was based on the updated 2018 [7] and 2020 [8] AHA guidelines for CPR and ECC and was provided to participants at least 4 weeks prior to the training for preparation. The training packages included lectures with PowerPoint presentations, video materials, practical demonstrations, and hands-on exercises. The BLS course covered, among other topics, the chain of survival, the use of automated external defibrillators, team dynamics, CPR for infants and children, ventilation techniques, opioid-related emergencies, and choking. For ACLS, topics included, among others, cardiac arrest, acute coronary syndromes, stroke, arrhythmias, respiratory arrest, types of cardiac arrest (pulseless electrical activity, asystole, and ventricular tachycardia/fibrillation), and postcardiac arrest care.
Data Collection and Assessment
After the training, an assessment of knowledge was conducted immediately through the self-administration of a standardized questionnaire and CPR skills drills, according to the updated 2018 [7] and 2020 [8] AHA guidelines for CPR and ECC. The questionnaire included demographics (gender, profession, facility type, and region) as well as 20 multiple-choice questions on BLS and ACLS. Ten questions were on BLS, and the other 10 questions were on ACLS. The participants took at least 30-45 minutes immediately after the training to complete the questionnaire.
Classification of Knowledge and Skill Scores for BLS and ACLS
The knowledge and skill scores on BLS and ACLS were categorized into 2 levels. Scores ≥90% are considered adequate, while scores <90% are regarded as inadequate.
Statistical Analysis
Data were coded and entered into Microsoft Excel 2016. Data were imported into SPSS software (version 25; IBM Corp) for analysis. Categorical data were presented as frequencies and percentages. When appropriate, the chi-square test or Fisher exact test was used to determine the associations between the BLS and ACLS knowledge and skill scores and demographic data. A P value <.05 was considered significant, and only those variables were included in the logistic regression analyses to test for associations.
Ethical Considerations
Ethical clearance was obtained from the Ghana Health Service Ethics Review Committee (approval 018/05/19). Informed consent was obtained from all participants after the purpose of the training was explained to them in English. Data from participants who opted out at any time from the study or incomplete data were not included in the final analysis. Privacy and confidentiality were ensured by completing the questionnaires individually, and the data were used following their consent. Participants were compensated (money for transportation and attendance and food such as breakfast, lunch, snacks, and take-home supper) for their participation in the training based on the number of days they participated. Our study adhered to the principles of the Declaration of Helsinki.
Results
BLS Training
A total of 229 health care professionals received BLS training, and immediately standardized questionnaires were administered for the assessment of knowledge and skills. The majority (152/229, 66.3%) were females. Most (107/229, 46.7%) were specialists or trainee specialists, with 48.1% (110/229) working in secondary health care facilities. Additionally, 26.2% (60/229) of the BLS training sessions were held in the Greater Accra region. The majority (171/229, 74.6%) demonstrated adequate knowledge and skills in BLS. We identified statistically significant associations between profession, facility, region, and BLS knowledge and skill scores (P<.05; Table 1).
Logistic regression analysis showed that respondents working in tertiary health care facilities were 80% less likely (adjusted odds ratio [AOR] 0.20, 95% CI 0.07-0.59; P=.003) to have adequate BLS knowledge and skills compared to those in primary health care facilities. Respondents in the Volta and Oti regions were 4.94 times more likely (AOR 4.94, 95% CI 1.17-20.80; P=.03) to possess adequate BLS knowledge and skills compared to those in the Bono East region (Table 2).
ACLS Training
In total, 124 health care professionals received ACLS training, and standardized questionnaires were administered for the assessment of knowledge and skills. Most (73/124, 58.8%) were males. The majority (89/124, 71.7%) were doctors (house officer/medical officer/senior medical officer). More than half (64/124, 51.6%) worked in tertiary health care facilities. Most (55/124, 44.3%) of the ACLS trainings took place in the Greater Accra region. The majority (91/124, 73.4%) showed adequate knowledge and skills in ACLS. Statistically significant differences in ACLS knowledge and skills scores were observed based on gender, profession, and facility (P<.05; see Table 3).
Compared to their female counterparts, males were 7.05 times more likely (AOR 7.05, 95% CI 2.69-18.46; P<.001) to have adequate knowledge and skills in ACLS (see Table 4).
Discussion
Principal Findings
This study aims to evaluate the knowledge and skills of health care professionals immediately after training in Ghana on managing cardiac arrest through BLS and ACLS. We found that 75% of the health care professionals had adequate knowledge and skills in BLS, which was notably higher than that reported in other studies [2,9,11,12]. In similar training contexts, these percentages were 12% in Nepal [9] and 54% in Yemen [12]. Our results differ from studies in Afghanistan [2] and Pakistan [11], where 5% and 42% of respondents, respectively, had adequate BLS knowledge. The differences across these studies could be attributed to variations in research methods, the cutoff points used for determining knowledge levels, the effectiveness of the training programs, and whether assessments were conducted immediately after training. Additionally, prior BLS training may account for these variations, as Chaudhary et al [9] reported a strong correlation between knowledge scores and previous training.
This study reveals significant associations between BLS knowledge and skill scores and profession, facility, and region; however, no research has shown an association between the knowledge and skill scores of professions and facility type or region for comparison. We found that health care professionals working in tertiary health care facilities were less likely to have adequate knowledge and skills about BLS than those working in primary health care facilities. The reason could be that primary health care facilities in Ghana often provide basic emergency care as part of their primary services to communities; therefore, they receive more focused and frequent training on BLS techniques as part of their routine responsibilities compared to tertiary health care facilities, which prioritize specialized care for severe medical conditions, resulting in less emphasis on BLS training. The disparity in the findings could also be attributed to the assumption of prior knowledge and skills from practicing in a tertiary health facility.
Our study shows that health care professionals in facilities within the Volta and Oti regions possessed more adequate knowledge and skills in BLS compared to those in the Bono East region. This may be due to differences in the frequency of BLS training programs conducted in these areas. Facilities in the Volta and Oti regions might have more regular BLS training sessions than those in Bono East. Additionally, regions with better access to resources may facilitate more effective training for health care professionals, resulting in higher retention of BLS knowledge and skills; however, there is no evidence in the literature to support this justification.
Regarding ACLS, this study shows that 73% of the participants possessed adequate knowledge and skills, which contrasts with that reported in studies conducted in Ethiopia [1] and Spain [4]. Those studies showed that the majority, at 40% and 28%, respectively, had adequate knowledge of ACLS [1,4]. The difference may relate to variations in study methodologies, how knowledge was classified, and the previous training received on ACLS; none of these assessments were based on AHA-certified ACLS training. Adal and Emishaw [1] revealed that health care professionals who had previously received ACLS training were 5 times more knowledgeable than those who had not.
We found a significant difference between the ACLS knowledge and skill scores and gender. Compared with their female counterparts, male health care professionals were more likely to have adequate knowledge and skills in ACLS. This may be because our study had more male participants than female counterparts. Another reason could be the differences in the types or frequency of the clinical experiences.
Strengths and Limitations
This study’s strength is that it is the first in Ghana to evaluate health care professionals' knowledge and skills in managing cardiac arrest by using BLS and ACLS. It also included professionals from various backgrounds, facility types, and regions, thereby providing a thorough assessment across different parts of Ghana. In addition, our study created a standard for BLS and ACLS training and assessment that could be used in Ghana and other countries to support and monitor health care professionals’ proficiency.
However, our study has some limitations. First, the evaluation of BLS and ACLS knowledge and skills was based on posttraining tests, which may not accurately reflect participants’ real-world performance in emergencies and could introduce social desirability bias. Second, participants were recruited from only 8 regions and may not represent all the health care professionals in Ghana, potentially leading to selection bias. Third, there are no data on the specific deficiencies encountered.
Conclusion
Given an opportunity to learn and practice, health care professionals in Ghana attain adequate knowledge and skills in BLS and ACLS. BLS knowledge and skill scores were significantly associated with profession, facility, and region. Additionally, ACLS knowledge and skill scores were found to be associated with gender, profession, and facility. It is recommended that BLS and ACLS training be provided regularly to all health care professionals across all regions to improve their ability to respond effectively to medical emergencies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adal O Emishaw S Knowledge and attitude of healthcare workers toward advanced cardiac life support in Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia, 2022 SAGE Open Med 20231120503121221150101 10.1177/205031212211501013668579510.1177_2050312122115010136685795 PMC 9850119 · doi ↗ · pubmed ↗
- 2Nemat A Nedaie M Essar M Ashworth H Aminpoor H Sediqi A Basic life support knowledge among healthcare providers in Afghanistan: a cross-sectional study of current competencies and areas for improvement Ann Med Surg. 2023;5?20230316810.1097/ms 9.000000000000027337113965 PMC 1012922237113965 · doi ↗ · pubmed ↗
- 3Kumar R Raja Badil Gulsher Ali J Kumar A Advanced cardiovascular life support performance: study on the effectiveness of training among nurses in a tertiary care hospital, Karachi JPRI 202202091810.9734/jpri/2022/v 34i 8b 35478 · doi ↗
- 4Pérez-Ibáñez Rosa Almodóvar-Fernández Isabel Gregori Roig PSánchez-Thevenet Paula Level and determinants of advanced life support knowledge among nurses in Spain: a national cross-sectional study SAGE Open Med 20251320503121251326655 10.1177/205031212513266554011586610.1177_2050312125132665540115866 PMC 11924098 · doi ↗ · pubmed ↗
- 5Doku A Tuglo LS Boima V Agyekum F Aovare P Ali Abdulai Martha Godi A Peters RJ Agyemang C Prevalence of cardiovascular disease and risk factors in Ghana: a systematic review and meta-analysis Glob Heart 202419121 10.5334/gh.13073840461438404614 PMC 10885824 · doi ↗ · pubmed ↗
- 6Akumiah F Yakubu A Ahadzi D Tuglo L Mishra S Mohapatra R Cardiovascular care in Africa: cost crisis and the urgent need for contextual health service solutions Glob Heart 2023830310.5334/gh.12593766481937664819 PMC 10473171 · doi ↗ · pubmed ↗
- 7Panchal A Berg K Kudenchuk P Del RM Hirsch K Link M 2018 American Heart Association Focused Update on Advanced Cardiovascular Life Support Use of Antiarrhythmic Drugs During and Immediately After Cardiac Arrest: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation 2018 American Heart Association focused update on advanced cardiovascular life support use of antiarrhythmic drugs during and immediately after cardiac arresta 10.1161/c · doi ↗ · pubmed ↗
- 8Panchal Ashish R Bartos Jason A Cabañas José G Donnino Michael W Drennan Ian R Hirsch Karen G Kudenchuk Peter J Kurz Michael C Lavonas Eric J Morley Peter TO'Neil Brian J Peberdy Mary Ann Rittenberger Jon C Rodriguez Amber J Sawyer Kelly N Berg Katherine M Adult Basic Advanced Life Support Writing Group Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care Circulation 2020102014216_suppl_2S 366S 468 10.1161/CIR.00000000000009163 · doi ↗ · pubmed ↗