Integrated treatment-decision algorithms for childhood TB: modelling diagnostic performance and costs
M. Gaeddert, D. Jaganath, A. Civan, H.T. Nguyen, M. Bonnet, E. Wobudeya, O. Marcy, M. De Allegri, C.M. Denkinger

TL;DR
This study models diagnostic performance and costs of treatment-decision algorithms for childhood TB in Uganda, comparing primary health centers and hospitals.
Contribution
The novel contribution is evaluating integrated TB treatment-decision algorithms with and without chest X-ray in different healthcare settings.
Findings
TDAs showed high sensitivity (80.8%–91.9%) but low specificity (50.9%–60.9%).
Using mobile CXR at PHCs had the lowest cost per treatment-decision (I$287).
DH referral was the most expensive scenario (I$449 per treatment-decision).
Abstract
To improve childhood TB diagnosis, treatment-decision algorithms (TDAs) with and without chest X-ray (CXR) were developed for children under age 10. We aimed to model diagnostic performance and costs of implementing TDAs in primary health centre (PHC) and district hospital (DH) settings in Uganda. We developed decision-tree models following the TDA pathway from evaluation to treatment-decision. We compared six scenarios with combinations of diagnostic testing (stool and respiratory Xpert, urine lipoarabinomannan, and/or CXR) at PHCs and DHs. Outcomes were diagnostic accuracy and cost per correct treatment-decision for a cohort of 10,000 children with presumptive TB using a Monte Carlo simulation from a health system perspective. Costs were reported in 2024 international dollars (I$). In all scenarios, TDAs had high sensitivity (80.8%–91.9%) but low specificity (50.9%–60.9%). Total…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
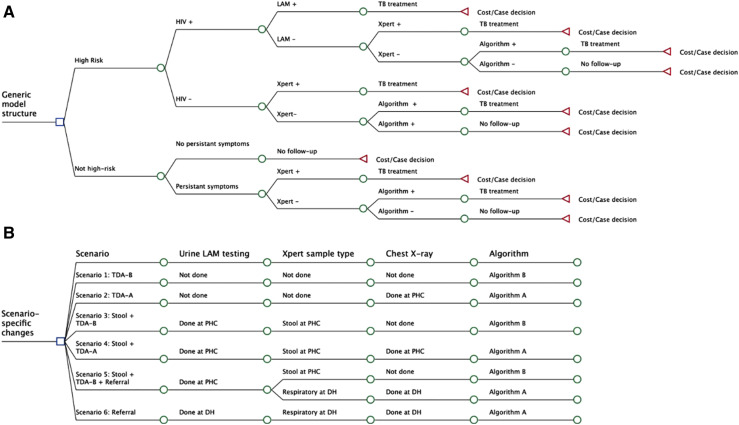 Figure 1
Figure 1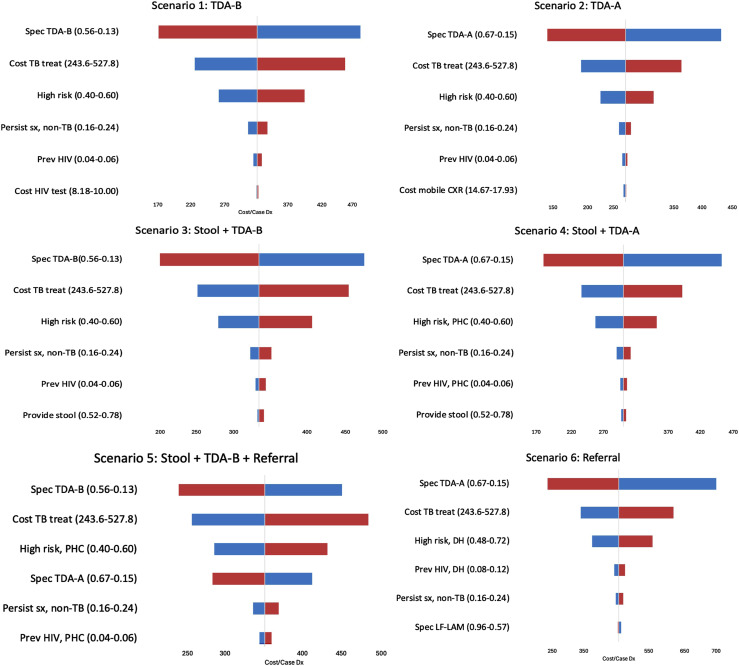 Figure 2
Figure 2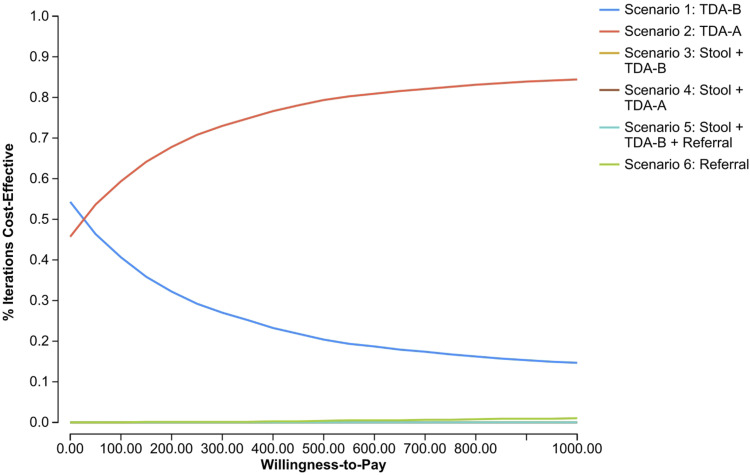 Figure 3
Figure 3| Scenario | Scenario 1: TDA-B | Scenario 2: TDA-A | Scenario 3: Stool + TDA-B | Scenario 4: Stool + TDA-A | Scenario 5: Stool + TDA-B + referral | Scenario 6: Referral |
|---|---|---|---|---|---|---|
| TDA | Algorithm B | Algorithm A | Algorithm B | Algorithm A | Algorithm A and B | Algorithm A |
| CXR available | No | Yes | No | Yes | Partial | Yes |
| TB-specific testing | No | No | Yes | Yes | Yes | Yes |
| Accuracy, overall | 56.8% | 61.6% | 56.1% | 60.7% | 56.9% | 55.0% |
| High-risk group | 32.9% | 40.3% | 32.3% | 39.4% | 33.4% | 41.6% |
| Not high-risk group | 86.0% | 87.4% | 86.0% | 87.3% | 86.2% | 86.6% |
| Sensitivity, overall | 80.8% | 82.7% | 84.6% | 86.3% | 88.6% | 91.9% |
| High-risk group | 86.7% | 89.8% | 94.4% | 97.2% | 95.5% | 97.4% |
| Not high-risk group | 73.8% | 74.5% | 71.3% | 71.3% | 79.1% | 75.2% |
| Specificity, overall | 56.1% | 60.9% | 55.2% | 59.9% | 55.9% | 50.9% |
| High-risk group | 31.2% | 38.8% | 30.2% | 37.5% | 31.3% | 35.0% |
| Not high-risk group | 86.4% | 87.8% | 86.4% | 87.7% | 86.4% | 87.7% |
| PPV | 5.5% | 6.3% | 5.6% | 6.4% | 6.0% | 17.1% |
| High-risk group | 3.8% | 4.4% | 4.3% | 4.9% | 4.4% | 15.1% |
| Not high-risk group | 14.9% | 16.5% | 13.5% | 14.8% | 14.8% | 35.8% |
| NPV | 98.9% | 99.1% | 99.1% | 99.3% | 99.4% | 98.3% |
| High-risk group | 98.7% | 99.2% | 99.4% | 99.8% | 99.5% | 99.1% |
| Not high-risk group | 99.0% | 99.1% | 99.0% | 99.0% | 99.3% | 97.5% |
| Evaluated with clinical score | 64.8% | 64.8% | 62.3% | 62.3% | 60.7% | 65.8% |
| High-risk group | 100% | 100% | 96.2% | 96.2% | 93.7% | 86.3% |
| Not high-risk group | 21.9% | 21.9% | 20.0% | 20.0% | 19.5% | 17.7% |
| Scenario | Scenario 1: TDA-B | Scenario 2: TDA-A | Scenario 3: Stool + TDA-B | Scenario 4: Stool + TDA-A | Scenario 5: Stool + TDA-B + referral | Scenario 6: Referral |
|---|---|---|---|---|---|---|
| Total cost | $1,772,666.21 | $1,768,957.61 | $1,953,000.94 | $1,893,672.50 | $2,032,567.67 | $2,470,297.56 |
| Treatment, total | $1,633,019.46 | $1,466,310.86 | $1,666,361.18 | $1,505,451.14 | $1,648,965.50 | $1,932,007.71 |
| Treatment, TB cases | $89,877.68 | $92,052.14 | $93,864.19 | $95,676.24 | $98,213.11 | $330,880.33 |
| High risk | $52,187.04 | $53,999.09 | $60,522.47 | $62,334.52 | $61,247.29 | $262,747.25 |
| Not high risk | $37,690.64 | $38,053.05 | $33,341.72 | $33,341.72 | $36,965.82 | $68,133.08 |
| Overtreatment | $1,543,141.78 | $1,374,258.72 | $1,572,496.99 | $1,409,774.90 | $1,550,752.39 | $1,601,127.38 |
| High risk | $1,328,232.65 | $1,181,819.01 | $1,359,762.32 | $1,218,060.01 | $1,338,380.13 | $1,478,995.21 |
| Not high risk | $214,909.13 | $192,439.71 | $212,734.67 | $191,714.89 | $212,372.26 | $122,132.17 |
| Non-treatment costs | $139,646.75 | $302,646.75 | $286,639.76 | $388,221.36 | $383,602.17 | $538,289.85 |
| Cases correctly diagnosed | 5,683 | 6,155 | 5,614 | 6,068 | 5,686 | 5,501 |
| Cost per correct decision | $311.92 | $287.40 | $347.88 | $312.08 | $357.47 | $449.06 |
- —National Institute of Allergy and Infectious Diseases10.13039/100000060
- —National Heart, Lung, and Blood Institute10.13039/100000050
- —German Center for Infection Research (DZIF)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Diagnosis and treatment of tuberculosis · Healthcare Facilities Design and Sustainability
The burden of childhood TB remains high globally, driven by challenges in diagnosis and subsequent treatment initiation. There were an estimated 1.3 million new cases of TB and 191,000 deaths due to TB in children under 15 years of age in 2023,^1^ and it is estimated that 96% of deaths are in children not diagnosed and treated.^2^ In young children, TB often presents with non-specific symptoms, and sputum-based testing is rarely feasible due to challenges obtaining samples.^3^ Even when sputum can be collected, sensitivity of culture and molecular testing is reduced due to the paucibacillary nature of childhood disease.^4^ Furthermore, chest X-ray (CXR) findings can be heterogeneous and difficult to interpret, especially in children living with HIV (CLHIV), and CXR is typically not available at primary health centres (PHCs).^5^ Diagnostic capacity combining clinical assessment with radiographic and laboratory information may only be present in centralised district hospitals (DHs). Decentralising childhood TB services has been shown to expand access to diagnosis and treatment, increasing case-finding at PHCs.^6^
To standardise diagnostic approaches and enable more children to initiate treatment earlier, two treatment-decision algorithms (TDAs) were developed for settings with and without CXR, guided by a large individual-patient data meta-analysis.^7^ The algorithms were designed with high sensitivity to reduce missed cases, at the expense of low specificity, potentially leading to significant overtreatment and associated costs. Previous studies have only validated the TDA’s clinical scoring system and have not incorporated other aspects such as combinations of diagnostic tests and settings.^8,9^ The World Health Organization (WHO) gave a conditional recommendation for the TDAs pending further validation of their accuracy and considerations for implementation, including costs, to guide programmatic adoption and scale-up.^10,11^ The objectives of this analysis were to model the diagnostic performance and costs of implementing TDAs across different implementation scenarios in primary care and hospital-based settings in Uganda.
METHODS
We modelled the WHO TDAs among children under 10 years of age presenting with symptoms suggestive of pulmonary TB, including cough or fever for 2 weeks or more, poor appetite, weight loss or failure to thrive, and fatigue or reduced playfulness, who do not require urgent care. The setting for the analysis was outpatient clinics in PHCs and DHs in Uganda, which was chosen as a representative high-burden country with a TB incidence rate of 198/100,000, and 37% of TB cases are living with HIV.^1^ Of the TB cases reported nationally in 2023, over 12,000 (14%) were among children of 0–14 years,^1^ but this may be underestimating the true burden.^12^ The current standard of care is to conduct symptom screening for all children at health facility entry points; those meeting the criteria for presumptive TB are evaluated with HIV testing, clinical examination, CXR, and collecting samples for molecular testing.^12^ In this setting, most resources for diagnostic testing, including X-ray facilities, on-site laboratories with GeneXpert, and clinical resources to perform gastric aspirate and sputum induction, are at centralised facilities. However, approximately 54% of children initially present at PHCs with limited resources, so children with presumptive TB are often referred to DHs.^13^
WHO TDAs
Each TDA follows a sequence of evaluations. Because the algorithms aim to detect as many cases as possible, a negative result on any step leads to further assessment until a treatment-decision is reached. Children at high risk for rapid disease progression (under 2 years of age, living with HIV, or with severe acute malnutrition) are tested for TB immediately, including molecular testing on stool or respiratory samples with GeneXpert and urine lateral flow lipoarabinomannan (LF-LAM, Determine TB LAM, Abbott, Chicago) for CLHIV. The children not in a high-risk group are assessed for other likely conditions related to their symptoms and return for follow-up in 2 weeks. Children whose symptoms resolve by the follow-up visit exit the algorithm and undergo no further testing. Children with persistent symptoms continue for molecular testing. If these tests are negative or not available, the child proceeds to the clinical scoring step, which considers history of TB contact and presence of individual symptoms. Algorithm A (TDA-A) includes CXR findings in the scoring and can be used where X-ray is available. While this is typically relevant for DHs, mobile vans with portable X-ray machines may be available to expand access to PHCs.^14^ Algorithm B (TDA-B) is for settings without X-ray, typically PHCs, and only includes clinical signs and symptoms.
Model structure
We developed six scenarios comparing a range of strategies at PHCs and DHs. We converted the TDAs into a decision-tree model with separate arms for each scenario, following the above-described pathway from initial evaluation to treatment-decision (Figure 1). Scenario 1 (‘TDA-B’) considered the simplest scenario with only clinical diagnosis using the TDA-B scoring system and no molecular testing. Scenario 2 (‘TDA-A’) explored the impact of adding mobile CXR and use of the TDA-A scoring. Scenario 3 (‘Stool + TDA-B’) and Scenario 4 (‘Stool + TDA-A’) included molecular testing with Xpert Ultra on stool samples and urine LF-LAM for CLHIV, with or without mobile CXR. Scenario 5 (‘Stool + TDA-B + Referral’) began with stool testing at PHCs and referred a portion of children with a negative result to DHs for respiratory Xpert Ultra testing and TDA-A with CXR. Children in the high-risk group were more likely to be referred, and those who remained at PHCs were evaluated with the TDA-B score. This scenario most closely reflected the current standard of care in Uganda. Scenario 6 (‘Referral’) reflected the centralised approach where all children had CXR and respiratory sample testing at DHs.
Decision-tree model and scenario-specific changes. A shows a simplified version of the clinical pathway converted into a decision-tree model for each scenario. B shows the diagnostic tests used for each model scenario.
Model parameters and analysis
Estimates for clinical and cost parameters matching the modelled setting were obtained from the literature (Supplementary Data Table S1). Several clinical parameter estimates were obtained from a multi-site study on decentralisation of TB testing, and the authors (MB, OM, and EW) provided additional data for the Ugandan site.^13^ We also consulted expert opinion (see Acknowledgements) for input on clinical parameters, including TB prevalence and resolution of symptoms by the 2-week follow-up visit for children not in a high-risk group. Due to limited data available on pre-diagnostic loss and the unknown impact of new diagnostic strategies such as stool testing at PHCs, loss to follow-up before and during the diagnostic process was not included. The costs of clinical examination, sample collection, HIV testing, and TB molecular testing were included as specified for each scenario. The costs of facility-based and mobile CXR included the cost for interpretation by the treating clinician. The cost of respiratory sample collection at DH included gastric aspirates for children under five and induced or expectorated sputum for older children. TB treatment costs included direct costs of medications for 6 months and follow-up visits until completion of therapy. Patient costs such as transportation and the burden of treatment (i.e., giving daily medications and side effects) were not included. Drug-resistant TB was not included as the rates are low among children in Uganda.^15^
The outcomes were diagnostic accuracy and cost per correct treatment-decision (both true-positives and true-negatives). Treatment costs were reported separately for true TB cases, overtreatment, and risk group. Outcomes were calculated for a cohort of 10,000 children using a Monte Carlo simulation. The analysis adopted a health system perspective, using a time horizon of 1 year for program implementation, and no discounting was applied. Costs were converted to 2024 international dollars (I$) using World Bank inflation data.^16,17^
One-way and probabilistic sensitivity analyses (PSAs) were conducted to evaluate how uncertainty in model parameters impacted outcomes. TreeAge Pro 2024 was used for analysis. Details of the evaluation are reported following the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guidance (Supplementary Data Table S2).^18^ Ethical approval was not required as all parameters were obtained from published literature and there was no human subject participation.
Ethical statement
This analysis used data from published studies and did not require ethical approval.
RESULTS
Overall, the diagnostic accuracy of the scenarios was moderate, ranging from 55.0% to 61.6%, balancing a high sensitivity and low specificity (Table 1, full results in Supplementary Data Table S3). The sensitivity was high in all scenarios, ranging from 80.8% to 91.9%, indicating that the TDAs are not missing many TB cases. However, the specificity was consistently low (50.9%–60.9%), resulting in a low positive predictive value (5.5%–6.4%), particularly in Scenarios 1–5 at PHCs with low prevalence of TB disease (3%). The negative predictive value (NPV) was above 98% across all scenarios.
When comparing Scenarios 1 and 2 (clinical diagnosis with and without CXR, respectively), the addition of mobile CXR at PHCs improved both sensitivity (80.8% vs. 82.7%, respectively) and specificity (56.1% vs. 60.9%, respectively). The addition of molecular testing, with or without CXR, in Models 3 and 4 improved sensitivity (84.6% vs. 86.3%, respectively) and specificity (55.2% vs. 59.9%, respectively) compared to Scenarios 1 and 2. Referring either some or all children for CXR and respiratory sample testing (Scenarios 5 and 6, respectively) improved sensitivity (88.6% vs. 91.9%, respectively) but lowered specificity (55.9% vs. 50.9%, respectively). These relationships were similar when comparing high- and low-risk groups. However, low-risk groups had on average 12% lower sensitivity and 31% higher specificity compared to the overall results.
Costs
The total costs of TB testing and treatment for a cohort of 10,000 children ranged from I2,470,298 in Scenario 6 (Table 2). The costs were driven by the overtreatment of false-positive cases, which resulted in more than I$1.4 million in every scenario. The lower specificity in the high-risk group resulted in a larger proportion of overtreatment costs than in the low-risk group. Due to the low prevalence of TB at PHCs, the cost for treating true TB cases was only 5% of total costs for Scenarios 1–5.
The diagnostic costs are lowest in Scenario 1 with only clinical diagnosis (I538,290). When comparing scenarios, the increased cost of diagnostics was mostly offset by the decreased cost of overtreatment. For example, the addition of mobile CXR between Scenarios 3 and 4 increased diagnostic costs by I162,722. However, referring all children in Scenario 6 substantially increased diagnostic costs but did not reduce overtreatment. This is reflected in the cost per correct treatment-decision, which was lowest using mobile CXR at PHCs (Scenario 2, I449).
Sensitivity analyses
One-way sensitivity analyses showed that the parameters with the greatest impact were the specificity of TDAs, cost of TB treatment, and proportion of children who were high-risk (Figure 2). As TDA specificity increases, reduction in overtreatment lowers the cost per case. Decreasing treatment costs and proportions of high-risk children also decreased the cost per case. The PSA indicated that Scenario 2 was more cost-effective than other scenarios across a range of willingness-to-pay thresholds (Figure 3). Additional PSAs are in Supplementary Data Figure S1.
One-way sensitivity analyses for each scenario. Parameters are shown in order of decreasing impact on the outcome of cost per correct treatment-decision. Blue = low range of parameter; red = high range of parameter.
Cost-effectiveness acceptability curve. Probabilistic sensitivity analysis for the joint uncertainty of all parameters using a Monte Carlo simulation with 10,000 iterations. The cost-effectiveness acceptability curve shows which scenario was most cost-effective at the given willingness-to-pay threshold.
DISCUSSION
This is the first analysis to model both the diagnostic accuracy and costs of the new TDAs in a cohort of children across a range of implementation scenarios. The TDAs were developed to support the clinical assessment for childhood TB and reduce the diagnostic gap. We showed that the TDAs have high sensitivity to detect TB cases with high NPV, but their low specificity leads to substantial overtreatment costs. The current standard of referring children to DHs had both the highest sensitivity and highest cost. However, expanding diagnostic capacity at PHCs improved specificity, reduced overtreatment, and consequently offset costs. These findings suggest that implementation of TDAs at PHCs with and without TB-specific testing would have high sensitivity to detect TB and lower costs than referral to a DH, but further improvements are needed to reduce costs of overtreatment.
The scenarios with DH referral do not substantially improve accuracy or reduce costs compared to scenarios at PHCs. Although children have respiratory samples tested with highly specific Xpert Ultra, those with a negative result proceed to the less-specific clinical score and could still be initiated on TB treatment. At the same time, there are additional costs for the DH assessment and any previous PHC visits before referral. In PHC scenarios, mobile CXR improved specificity and higher diagnostic costs were offset by the reduction in overtreatment. Stool-based testing did not improve accuracy, again as children with negative stool tests would then be assessed with the clinical score. The difference in clinical pathway for high-risk children increased the sensitivity, but with a trade-off of lower specificity and associated higher overtreatment cost.
While stool and respiratory Xpert testing did not improve accuracy overall, it is important to recognise the benefits of microbiological confirmation, including detection of drug resistance.^19^ CXR also has benefits of classifying disease severity and eligibility for shorter treatment regimens, or identifying alternative diagnoses.^11^ Clinicians at DH may have more experience in making clinical TB diagnoses than at PHC, but implementation of algorithms in this setting, especially TDA-A with CXR, can support their clinical judgement.^13^ Additional benefits of decentralisation for children and caregivers include reduced costs and burden of visits to referral facilities.
However, it is important to recognise the high total costs. Our model estimated that the costs for a cohort of 10,000 children, including diagnostics and treatment, were over I32 million, and 84% came from international sources.^1^ In a time of decreased global health funding, it may not be feasible for national programs or donors to cover costs of expanding services, and the cost of diagnostics alone may not be affordable for many countries.^20^ An analysis of decentralisation strategies, which included scale-up costs such as training and equipment, found that decentralisation to the PHC level would likely not be cost-effective,^21^ and a cost-effectiveness analysis of TB screening in Uganda found similar challenges in an adult population with low TB prevalence.^22^ Our sensitivity analyses showed that improved TDA specificity, especially among high-risk children, and reduced treatment costs would provide the greatest impact. Moreover, implementing newly recommended shorter treatment regimens for children with non-severe disease would also reduce treatment costs.^11,23^
Strengths of this analysis include using parameters from studies conducted in similar high-burden settings, including a childhood TB decentralisation study in Uganda.^13^ We also consulted expert opinion to support the limited data available for some clinical parameters. However, there are still limited data available for childhood TB, and the impact of this uncertainty was explored in the sensitivity analyses. Clinicians at DHs with greater TB expertise may have better accuracy in clinical diagnosis than estimated in the TDAs.^24^ These models did not include pre-diagnostic loss to follow-up, so our estimations are likely overoptimistic. We also did not include patient costs which would likely support more patient-centred algorithms at PHCs. Implementation will require additional resources for training and supporting health care workers.
Clinical studies to validate TDA performance in high-burden settings are ongoing, and the results will inform future implementation. When these studies are completed, it will be valuable to conduct formal budget impact analyses. Additional evaluations including patient costs, caregiver preferences regarding location of care, and feedback from health care workers on their experience using the algorithms will inform stakeholder decision-making. Modifications to improve algorithm performance, especially increasing specificity (e.g., through more scalable and accessible pathogen-based diagnostics, adjusting the clinical score, or changing steps in clinical pathway), should be considered.
CONCLUSION
Increasing children’s access to TB diagnostic tools is important. Our models indicate that the TDAs have high sensitivity and NPV, enabling increased detection of childhood TB, and can be implemented at primary care centres at lower cost than DHs. However, the low specificity and subsequent overtreatment costs could reduce the feasibility of implementation in real-world settings, unless there are further efforts to improve specificity and reduce treatment costs.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global tuberculosis report 2024. Geneva: WHO, 2024.
- 2Dodd PJ, The global burden of tuberculosis mortality in children: a mathematical modelling study. Lancet Glob Health. 2017;5(9):e 898-e 906.28807188 10.1016/S 2214-109X(17)30289-9PMC 5556253 · doi ↗ · pubmed ↗
- 3Ioos V, Cordel H, Bonnet M. Alternative sputum collection methods for diagnosis of childhood intrathoracic tuberculosis: a systematic literature review. Arch Dis Child. 2019;104(7):629-635.30127061 10.1136/archdischild-2018-315453 · doi ↗ · pubmed ↗
- 4Atherton RR, Xpert MTB/RIF ultra for tuberculosis testing in children: a mini-review and commentary. Front Pediatr. 2019;7:34.30873392 10.3389/fped.2019.00034 PMC 6403143 · doi ↗ · pubmed ↗
- 5Berteloot L, Value of chest X-ray in TB diagnosis in HIV-infected children living in resource-limited countries: the ANRS 12229-PAANTHER 01 study. Int J Tuberc Lung Dis. 2018;22(8):844-850.29991391 10.5588/ijtld.18.0122 · doi ↗ · pubmed ↗
- 6Zawedde-Muyanja S, Decentralisation of child tuberculosis services increases case finding and uptake of preventive therapy in Uganda. Int J Tuberc Lung Dis. 2018;22(11):1314-1321.30355411 10.5588/ijtld.18.0025 PMC 7237826 · doi ↗ · pubmed ↗
- 7Gunasekera KS, Development of treatment-decision algorithms for children evaluated for pulmonary tuberculosis: an individual participant data meta-analysis. Lancet Child Adolesc Health. 2023;7(5):336-346.36924781 10.1016/S 2352-4642(23)00004-4PMC 10127218 · doi ↗ · pubmed ↗
- 8Kitonsa PJ, The accuracy of the Uganda national tuberculosis and leprosy program diagnostic algorithm and the World Health Organisation treatment decision algorithms for childhood tuberculosis: a retrospective analysis. P Lo S Glob Public Health. 2025;5(4):e 0004026.40193335 10.1371/journal.pgph.0004026 PMC 11975100 · doi ↗ · pubmed ↗