Knowledge, Perceptions, and Expectations of Dental Anesthesia Among Patients Attending the College of Dentistry Clinic in Hail, Saudi Arabia: A Cross-Sectional Study
Hanady S Alrasheedi, Anifah N Alshammari, Hussein A Marouf

TL;DR
This study explores how patients in Saudi Arabia understand dental anesthesia, finding many are unaware of its role and anesthesiologists' responsibilities.
Contribution
The study provides new insights into patient perceptions and knowledge gaps regarding dental anesthesia in a specific regional context.
Findings
Most patients did not recognize the benefits of visiting the anesthesia room before surgery.
A majority believed physicians are not responsible for anesthesia.
Patients preferred general anesthesia to avoid seeing the surgery.
Abstract
Introduction: Anesthesia is unique because it is not a direct means of treatment; rather, it allows other physicians to do things that may treat, diagnose, or cure an ailment, which would otherwise be painful or complicated. In the preoperative period, there are a lot of goals of preparation, but one of the most important is to eliminate anxiety. The current study aims to assess the patients’ knowledge regarding the anesthetist's role and their knowledge about dental anesthesia. Methods: It is a sectional questionnaire prepared at the Faculty of Dentistry, Hail University, Hail, Saudi Arabia. The study population was female patients. The questionnaire consisted of a general part with questions on demography for all participants and three other sections containing multiple-choice questions. The data were analyzed using the IBM SPSS Statistics software, version 22.0 (IBM Corp., Armonk,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
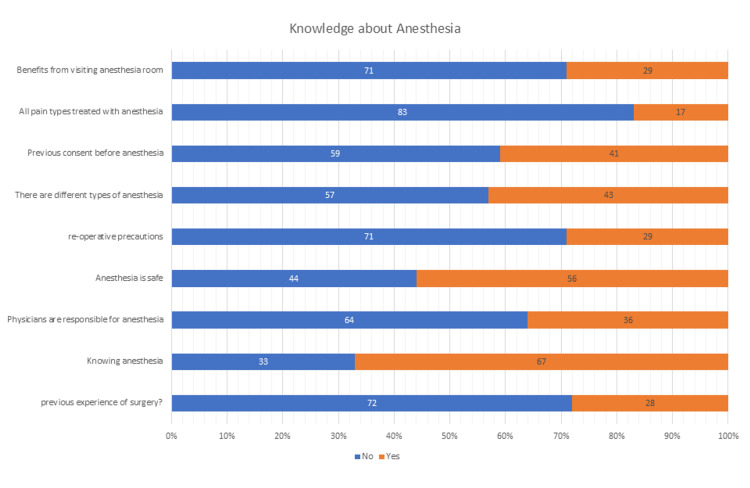 Figure 1
Figure 1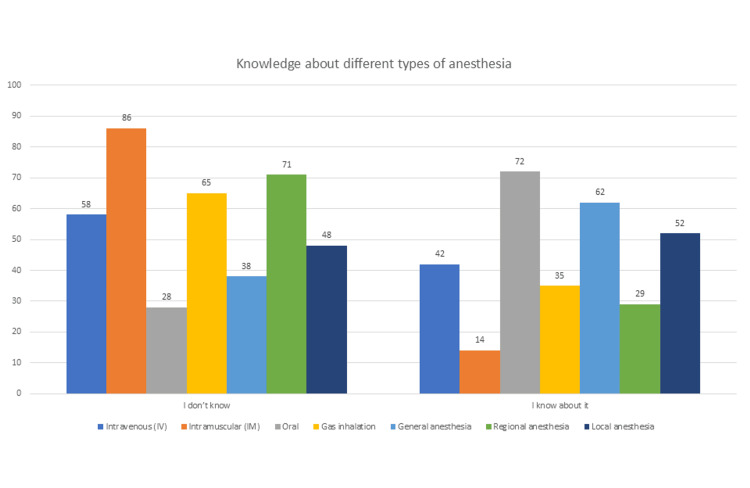 Figure 2
Figure 2| Categories | Frequency (percentage) | |
| Age (in years) | 18-24 | 22 (22%) |
| 25-30 | 23 (23%) | |
| 31-35 | 21 (21%) | |
| 36-40 | 20 (20%) | |
| 40+ | 14 (14%) | |
| Educational level | High | 57 (57%) |
| Low | 43 (43%) | |
| Occupation | Housewife | 43 (43%) |
| Medical professional | 3 (3%) | |
| Non-medical | 15 (15%) | |
| Not working | 20 (20%) | |
| Students | 19 (19%) | |
| Nationality | Non-Saudi | 14 (14%) |
| Saudi | 86 (86%) | |
| Socio-economic condition | High | 7 (7%) |
| Middle | 65 (65%) | |
| Poor | 28 (28%) | |
| Smoking status | Currently smoking | 1 (1%) |
| Ex-smoking | 8 (8%) | |
| Non-smoking | 91 (91%) | |
| Physical activity | Active | 64 (64%) |
| Inactive | 36 (36%) | |
| Frequency of hospital visits | Never go to the hospital | 6 (6%) |
| Once every 5 years | 35 (35%) | |
| Once every 6 months | 18 (18%) | |
| Once every month | 9 (9%) | |
| Once every one year | 32 (32%) | |
| Anesthesia knowledge | Insufficient | 69 (69%) |
| Sufficient | 31 (31%) | |
| Source of knowledge | Media | 38 (38%) |
| Physician | 21 (21%) | |
| Public awareness events | 29 (29%) | |
| Teaching and schooling | 12 (12%) | |
| Total | 100 (100%) | |
| Categories | Frequency (percentage) | |
| Reasons for preferring general anesthesia | Advice of relatives | 10 (10%) |
| Fear of seeing things during surgery | 34 (34%) | |
| Less risk compared to regional anesthesia | 33 (33%) | |
| Other choices not offered | 23 (23%) | |
| Reasons for refusal of general anesthesia | Expensive | 9 (9%) |
| Fear of death | 31 (31%) | |
| Sore throat | 11 (11%) | |
| Will not regain consciousness | 49 (49%) | |
| Reasons for preferring regional anesthesia | Advice of relatives | 20 (20%) |
| Better post op pain control | 18 (18%) | |
| Less expensive | 2 (2%) | |
| Safe | 56 (56%) | |
| Want to awake during surgery | 4 (4%) | |
| Reasons for refusal of regional anesthesia | Concern about backache | 12 (12%) |
| Concern about headache | 13 (13%) | |
| Concern about numbness | 40 (40%) | |
| Don't want to awake during surgery | 29 (29%) | |
| Relatively bad experience | 6 (6%) | |
| Total | 100 (100%) | |
| Categories | Anesthesia knowledge | ||||
| Insufficient (n=69) | Sufficient (n=31) | P-value* | χ² value | ||
| Age (years) | 18-25 | 15 (21.7%) | 7 (22.6%) | 0.795** | |
| 25-30 | 17 (24.6%) | 6 (19.4%) | |||
| 30-35 | 16 (23.2%) | 5 (16.1%) | |||
| 35-40 | 12 (17.4%) | 8 (25.8%) | |||
| 40+ | 9 (13.0%) | 5 (16.1%) | |||
| Educational level | High | 34 (49.3%) | 23 (74.2%) | 0.02*** | 5.42 |
| Low | 35 (50.7%) | 8 (25.8%) | |||
| Occupation | Housewife | 34 (49.3%) | 9 (29.0%) | 0.029*** | 10.81 |
| Medical professional | 0 (0.0%) | 3 (9.7%) | |||
| Non-medical | 8 (11.6%) | 7 (22.6%) | |||
| Not working | 13 (18.8%) | 7 (22.6%) | |||
| Student | 14 (20.3%) | 5 (16.1%) | |||
| Nationality | Non-Saudi | 9 (13.0%) | 5 (16.1%) | 0.681** | |
| Saudi | 60 (87.0%) | 26 (83.9%) | |||
| Socio-economic condition | High | 4 (5.8%) | 3 (9.7%) | 0.192** | |
| Middle | 42 (60.9%) | 23 (74.2%) | |||
| Poor | 23 (33.3%) | 5 (16.1%) | |||
| Previous experience of surgery? | No | 54 (78.3%) | 18 (58.1%) | .037*** | |
| Yes | 15 (21.7%) | 13 (41.9%) | |||
| Physical activity | Active | 39 (56.5%) | 25 (80.6%) | 0.02*** | |
| Inactive | 30 (43.5%) | 6 (19.4%) | |||
| Frequency of hospital visits | Never go to the hospital | 5 (7.2%) | 1 (3.2%) | 0.0001*** | 19.20 |
| Once every 5 years | 33 (47.8%) | 2 (6.5%) | |||
| Once every 6 months | 6 (8.7%) | 12 (38.7%) | |||
| Once every month | 5 (7.2%) | 4 (12.9%) | |||
| Once every one year | 20 (29.0%) | 12 (38.7%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Anxiety and Anesthesia Techniques · Dental Research and COVID-19 · Dental Education, Practice, Research
Introduction
Anesthesia is unique because it is not a direct means of treatment; rather, it allows other physicians to treat, diagnose, or cure an ailment that would otherwise be painful or complicated. The preoperative evaluation embraces assessing the patient's physiological and psychological condition, gathering information regarding medical, surgical, and medication history, conducting laboratory examinations, and detecting anesthesia-related hazards. During the preoperative phase, numerous preparatory objectives exist, with the paramount goal being the alleviation of anxiety [1, 2]. Numerous patients experience dread and anxiety in the preoperative phase due to insufficient information regarding possible complications related to anesthesia and surgery. Numerous studies have shown inadequate public understanding of anesthesia and the role of anesthetists [3, 4].
A study conducted by Krishnamurthy et al. [5] demonstrated that most participants were aware of one or more symptoms associated with anaphylaxis. However, none of the participants were aware of all the symptoms associated with anaphylaxis. Another study by Mohajer et al. [6] showed that a total of 744 responded to the questionnaire; 58% of the participants were deemed to have sufficient understanding of anesthesia, while 42% had insufficient knowledge; 69% of respondents agreed that anesthesia is safe, while 31% disagreed. Their study also showed a correlation between the education level and the knowledge about anesthesia and anesthetists.
One more study was done by Sagün et al. [7] using a questionnaire consisting of 21 questions to be filled out by the patients who applied to the anesthesia clinic. They reported that out of the 250 patients studied, 37.6% had secondary education, and the highest percentage belonged to the housewives (33.6%). This study found that having an anesthetic experience and a high level of education have a statistically significant effect on anesthesia knowledge.
The current study aims to evaluate the awareness of local female patients regarding the role of dental anesthesia and anesthesiologists and the need for educating them.
Materials and methods
It is a cross-sectional questionnaire that was prepared at the Faculty of Dentistry, Hail University, Hail, Saudi Arabia. The population was female patients who attended the Faculty of Dentistry, Hail University, from May 1, 2020, to August 31, 2020.
Our inclusion criteria were female patients who were aged ≥18 years, attended the Faculty of Dentistry at Hail University, and had undergone any dental procedure that required anesthesia. As the department only receives female patients, the sample included only female patients. We excluded female patients who were aged < 18 years, males, and patients who had undergone any dental procedure that did not require anesthesia.
Sampling procedure
We used random sampling. The study was open. The questionnaire was interviewer-administered to help the patients fill out the questionnaire. The questionnaire was in English, and no translation was needed (Appendix A). The questionnaire included a basic component with demographic questions for all participants, as well as three other parts with multiple-choice questions addressing discrete facts and demanding a "Yes," "No," or "Don't know" response. Patients were asked about their physical activity and smoking status, as both can affect patients' response to anesthesia. Socioeconomic status was defined as low if patients had limited financial resources (i.e., difficulty affording food, housing, healthcare, or education); middle if they had moderate income and resources (i.e., enough money for daily operations, paying expenses, and modest growth) and were not considered poor; or high if they had greater access to financial resources (i.e., involved large transactions and major investments). Patients were categorized with a high educational level if they attended a university or college, and a low educational level if they obtained a degree before university or college.
The first segment included a series of questions designed to measure patients' attitudes and understanding of anesthesia, the role of anesthetists and surgeons in patient care, and patients' recollection of who the anesthetist or surgeon was if they had previously had anesthesia and surgery. The second segment consisted of multiple questions to assess patients' knowledge about anesthesia. In addition to anesthetists' experience in dealing with patients who had no prior experience with anesthesia or surgery. The third section consisted of a series of questions directed at all participants, assessing their knowledge of the proposed surgical procedure, technique, and choice of anesthesia (regional or general); potential complications of anesthesia; and desire to meet with the anesthetist and learn more about anesthesia.
The questionnaire used in this study was adapted from previously published and validated instruments that assessed patients’ knowledge and perceptions regarding anesthesia and the role of anesthesiologists, including those by Mohajer et al. [6], Sagün & Birbiçer [7], and Krishnamurthy et al. [5]. Content validity was ensured through expert review by faculty members in anesthesia and dentistry who confirmed the relevance and clarity of each item. Linguistic clarity and logical sequencing of questions were verified prior to data collection. Although internal-consistency reliability (e.g., Cronbach’s alpha (α)) was not recalculated in this study, the questionnaire’s prior validation in the cited works provides established reliability. A limited pilot application within the same institutional setting was conducted to confirm item comprehension and feasibility before the main survey. The response rate was 95%.
Knowledge scores were dichotomized as follows: Sufficient knowledge: participants answering ≥ 50% of the knowledge items correctly; Insufficient knowledge: participants answered fewer than 50% correctly.
Data analysis
Data and statistical analyses were performed using IBM SPSS Statistics, Version 22.0 (IBM Corp., Armonk, NY, USA) and Microsoft Excel (Microsoft Corp., Redmond, WA) for data entry and verification. Descriptive statistics (frequency and percentage) summarized categorical variables. Associations between socio-demographic factors and knowledge level were examined using the chi-square (χ²) test. The level of statistical significance was set at p < 0.05, and results with p < 0.001 were considered highly significant. Effect magnitude for significant associations was interpreted using Cramer’s V or Phi (φ), where applicable. All analyses adhered strictly to standard cross-sectional analytical procedures.
Results
Socio-demographic characteristics
A total of 100 patients participated in the survey. All of them were women who attended the Faculty of Dentistry, Hail University. The socio-demographic data of the selected study sample are presented in Table 1. Participants were grouped into five age categories; 22% of the participants were aged between 18 and 24 years, 23% between 25 and 30 years, 21% between 31 and 35 years, and 20% between 36 and 40 years, while the last group included those who were more than 40 years old. The majority of the participants were Saudis (86%), and the rest (14%) were 14 non-Saudis. According to their responses about the level of education, 57% had a higher level of education.
Regarding participants’ occupation, the majority were housewives, representing about 43% of the whole sample. On the other hand, only 3% were medical professionals, 15% were non-medical, and 19% were students. Of the participants, 65% were of moderate socio-economic status, while only 7% were high level and 28% were poor.
Regarding physical activity and smoking, the studied sample showed that 64% were doing physical activity, and in addition, 91% were non-smokers.
Visiting hospitals varied among participants, as 35% of them visited hospitals every five years, 32% visited hospitals every year, and 6% never visited hospitals before. On the other hand, only 9% of the participants visited hospitals every month.
Participants’ knowledge about anesthesia was sufficient in 31% of them and insufficient in 69%. Most of their knowledge was from the media 38% while physicians had a limited role, about 21%.
Knowledge about anesthesia and its types
According to this scoring system, 31% of respondents demonstrated sufficient knowledge, and 69% insufficient knowledge; 34% and 33% of participants preferred general anesthesia because of fear of seeing things during surgery and less risk, respectively. While only 10% of participants preferred it because of their relatives’ advice, 49% of participants refused general anesthesia due to the fear of not regaining consciousness, while 31% of patients refused it because of fear of death (Table 2).
Regarding regional anesthesia, the major reason for preferring it was safety for 56% of participants, while the major reason for refusal was concern about numbness after the procedure for 40% of the participants (Table 2).
Upon assessing knowledge regarding anesthesia, 71% of participants reported that there are no benefits from visiting the anesthesia room before surgery. Of all participants, 83% did not think that all pain types can be treated with anesthesia, and 59% did not know about the consent before anesthesia; 57% of participants did not think that there are different types of anesthesia, and 56% of them think that anesthesia is safe. 64% of participants said that physicians are not responsible for anesthesia, and 71% did not believe in preoperative anesthesia precautions, as shown in Figure 1.
Participants' knowledge regarding anesthesia
Finally, participants were asked about their knowledge of different types of anesthesia (Figure 2). Their answers have shown us that intramuscular anesthesia was the least common type among participants, as 86% of them did not know about it, followed by regional anesthesia. Participants were most familiar with oral anesthesia, as 72% of them knew well about it, followed by general anesthesia.
Participants' knowledge about different types of anesthesia
Correlation studies
Of participants with sufficient knowledge about anesthesia, 74.2% (n=23) had a high educational level, while only 25.8% (n=8) had a low educational level. On the other hand, 49.3% (n=34) of participants with insufficient knowledge had a high educational level, while 50.7% (n=35) of them had a low educational level; χ² value = 5.42; p-value = 0.02 < 0.05. It is a significant finding (Table 3).
**Table 3: Comparison of sociodemographic characteristics according to anesthesia knowledge.*Statistical test applied = chi-square (χ²); Not statistically significant (p > 0.05); Statistically significant (p < 0.05)' 0.0001 highly significant (p < 0.001).
Regarding occupation, of participants with sufficient knowledge about anesthesia, nine (29.0%) were housewives, three (9.7%) were medical professionals, seven (22.6%) did not work in the medical field, and five (16.1%) were students. Of participants with insufficient knowledge about anesthesia, 34 (49.3%) were housewives, 14 (20.3%) were students, eight (11.6%) did not work in the medical field, and none of them (0.0%) were medical professionals; χ² value = 10.81; p-value = 0.029 < 0.05 (Table 3).
Regarding hospital visit frequency, participants visiting hospitals every month, every six months, and every year comprised 28 (90.3%) of those with sufficient knowledge about anesthesia. Participants visiting hospitals every five years, every year, and no hospitals before, comprised 58 (84%) of those with insufficient knowledge about anesthesia; χ² value = 19.20; p-value = 0.0001 < 0.001 (Table 3).
Discussion
When a dentist needs to inform patients of the benefits and risks of any procedure and the patient’s agreement to this procedure, this is where informed consent becomes evident. It has become mandatory for all dentists to obtain informed consent from every patient prior to any procedure because written and signed informed consent is the only evidence that can save the practitioners and their decision [8].
Results interpreted earlier had shown insufficient knowledge about anesthesia and anesthetists among patients of the Faculty of Dentistry, Hail University, in Hail City. Only 31% of our sample had sufficient knowledge about anesthesia, which is low compared to other studies. Another study in Saudi Arabia, Gazan [6], showed that 58.1% had sufficient knowledge about anesthesia, and about the same result was found in Pakistan [9] and in South Africa [10], which are higher than ours. Developed countries showed much higher results, such as 70% in Hong Kong [11]. Singh et al. conducted a study to evaluate the awareness among patients regarding anesthesia. The majority of their patients were not aware of the role of anesthesiologists inside and outside the operating room. However, they were aware of the general and regional anesthesia. Finally, they concluded that about half of the patients had good knowledge of anesthesia [12]. The reason for this low knowledge of patients regarding an anesthesiologist may be limited interaction of an anesthesiologist with their patients, as seen in hospital visits; participants visiting hospitals frequently knew more about anesthesia and anesthetists, and illiteracy.
Concerning anesthetists, only 36% in this study knew that anesthetists are physicians, but it is much higher in previous studies, such as 51% in Pakistan [9], 49.2% in Hong Kong [11], 40% in Turkey [12], and 87.4% in Saudi Arabia [6].
People may have concerns and fears about anesthesia. In this study, the major concern was not regaining consciousness in 49% of participants. A similar result found in a study in New York [13] was that 35% were afraid of not waking up after anesthesia.
The studied sample had a relatively low knowledge about anesthesia, as only 41% knew about the consent before anesthesia, but in a previous study in Saudi Arabia [6], about 78.5% knew about it. In addition, out of 100 participants in this study, only 29% knew about preoperative anesthesia measures. This result is low, comparable to 36.9% in India [14] and 91.9% in Saudi Arabia [6].
Regarding awareness about types of anesthesia, 43% of participants in this study were aware of different types of anesthesia, but in another previous study in India [15], only 7%. In addition, 62% of the study sample knew about general anesthesia. This is higher than some of the other studies, such as 27.5% in South Africa [10].
The level of education and occupation in our study was positively correlated with the knowledge about anesthesia and anesthetists (p-value = 0.02 < 0.05). This is similar to the results of other studies. Mohajer et al. [6] showed that the majority of the highly educated participants (82.2%) had sufficient knowledge about anesthesia. Marulasiddappa et al. [15] showed that patients with higher levels of education had better knowledge of anesthesiology and the role of an anesthesiologist (p < 0.05). In our study, previous surgery experience was positively correlated with knowledge of anesthesia (p-value = 0.037 < 0.05), but they were not correlated in Marulasiddappa et al.'s results [15], as they reported that about half of the participants had no idea about anesthesia despite the majority of them (62%) having had previous surgery with no statistically significant difference (p > 0.05) between those with previous surgery and those without previous surgery regarding their knowledge of anesthesiology and anesthesiologists.
Our study has its strengths. The possible outcomes patients might experience by having knowledge about anesthesia are alleviating fear of the unknown, reducing anxiety, increasing patients' satisfaction, and improving patients' compliance and adherence to the care plan. Our study has its own limitations. First, it was a single-center study that focuses mainly on the center and does not include other dental offices in the country. In addition, our study included only female participants, which can affect the generalizability of the study. Second, the small sample size and self-report bias can increase variability and lead to poor generalizability.
Conclusions
Many of the patients in our research were unfamiliar with the role of anesthesia, its many forms and procedures, and the role of anesthesiologists both inside and outside of the operating room. Although this could be attributed to a lower level of education and less contact with physicians, the anesthesiologists' fraternity bears a significant responsibility to educate patients and surgeons about the role of anesthesia, its types, techniques, and benefits, and the critical role played by anesthesiologists both inside and outside of the operating room. This may be accomplished by interacting with patients, using print and electronic media, and becoming acquainted with patients before surgery. This might significantly improve the image of anesthesiologists among patients and the general public.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pre-operative anxiety variables as possible predictors of post-operative stay in hospital Br J Clin Psychol Boeke S Jelicic M Bonke B 366368311992139317010.1111/j.2044-8260.1992.tb 01008.x · doi ↗ · pubmed ↗
- 2Hypnosis and daycase anaesthesia. A study to reduce pre-operative anxiety and intra-operative anaesthetic requirements Anaesthesia Goldmann L Ogg TW Levey AB 466469431988313667610.1111/j.1365-2044.1988.tb 06633.x · doi ↗ · pubmed ↗
- 3A survey of patients' knowledge of anaesthesia and perioperative care Singapore Med J Chew ST Tan T Tan SS Ip-Yam PC 399402391998 http://www.smj.org.sg/sites/default/files/3909/3909 a 3.pdf 9885718 · pubmed ↗
- 4Patients view of the anaesthetist in a developing country J Pak Med Assoc Khan FA Hassan S Zaidi A 47491999 https://europepmc.org/article/med/1046300710463007 · pubmed ↗
- 5Knowledge and attitude toward anaphylaxis during local anesthesia among dental practitioners in Chennai - a cross-sectional study Clin Cosmet Investig Dent Krishnamurthy M Venugopal NK Leburu A Kasiswamy Elangovan S Nehrudhas P 11712110201810.2147/CCIDE.S 159341 PMC 602960429988726 · doi ↗ · pubmed ↗
- 6A survey on Jazan public awareness about the role of the anesthesiologists Egypt J Hosp Med Mohajer AA Matiri AY Jaafari AA 376381702018 https://www.semanticscholar.org/paper/A-Survey-on-Jazan-Public-Awareness-about-The-Role-Mohajer-Matiri/94e 410169 daa 020b 5a 15d 1e 4cb 00268 cf 4064 be 4
- 7Patients', who applied to the anesthesia clinic, perceptions and knowledge about anesthesia in Türkiye Saudi J Anaesth Sagün A Birbiçer H Yapici G 170174720132395671810.4103/1658-354X.114076 PMC 3737694 · doi ↗ · pubmed ↗
- 8Informed consent: corner stone in ethical medical and dental practice J Family Med Prim Care Kakar H Gambhir RS Singh S Kaur A Nanda T 6871320142479124110.4103/2249-4863.130284 PMC 4005206 · doi ↗ · pubmed ↗