Remodelling and the fate of bone grafts in shoulder instability surgery
Sarah Remedios, Jillian Karpyshyn, Ivan Wong

TL;DR
This paper reviews surgical techniques for treating shoulder instability, focusing on bone grafts and their long-term outcomes.
Contribution
The paper provides a detailed analysis of graft selection and remodelling patterns in anterior glenoid bone augmentation.
Findings
The Latarjet procedure is widely used but has limitations like graft resorption and complications.
Distal tibial allograft (DTA) is a promising alternative with good anatomical match and clinical outcomes.
Understanding graft remodelling is crucial for optimizing surgical outcomes and postoperative management.
Abstract
Anterior glenoid bone loss is a critical factor in the surgical management of recurrent shoulder instability. In cases where bone loss exceeds the threshold for soft‐tissue repair, bony augmentation is necessary to restore joint stability and prevent recurrence. However, there remains considerable debate regarding the optimal surgical technique and graft selection to maximise clinical outcomes and ensure long‐term graft survival. The Latarjet procedure is widely performed and associated with high success rates. Nevertheless, it is not without limitations, particularly the potential for postoperative complications and inconsistent graft resorption rates. Distal tibial allograft (DTA) has emerged as a biomechanically favourable alternative. Its osteochondral surface offers a strong anatomical match for the glenoid and has shown promising clinical results. Despite its growing adoption,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
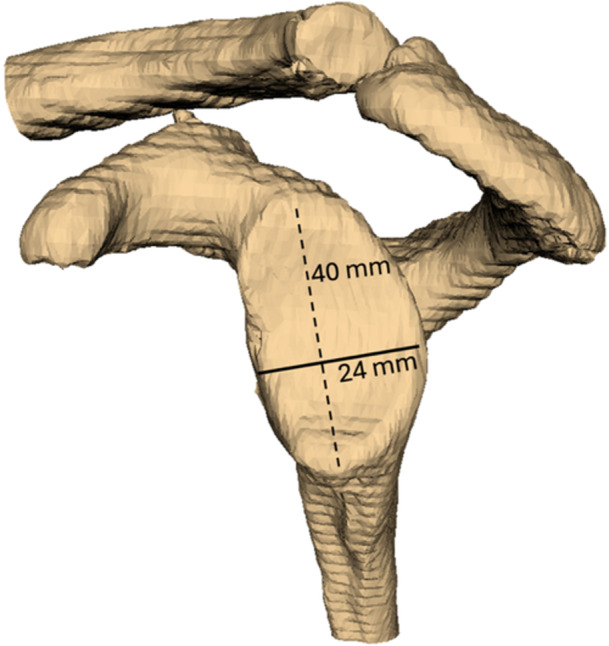 Figure 1
Figure 1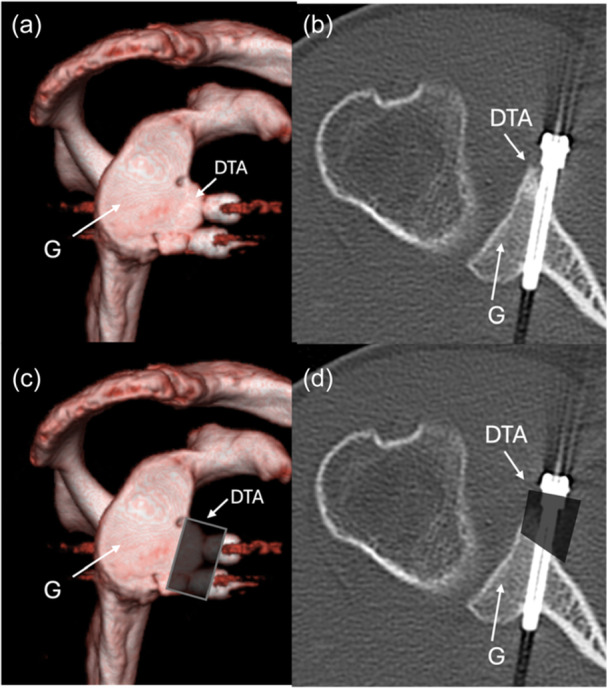 Figure 2
Figure 2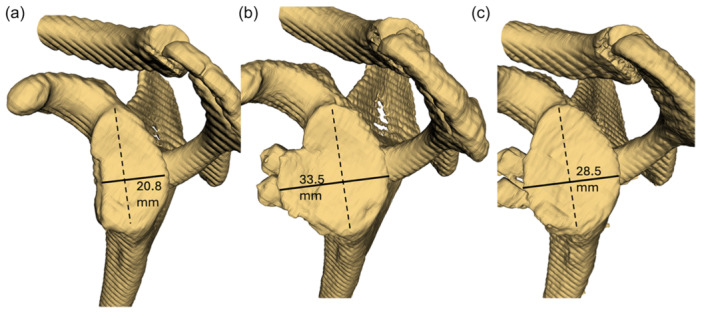 Figure 3
Figure 3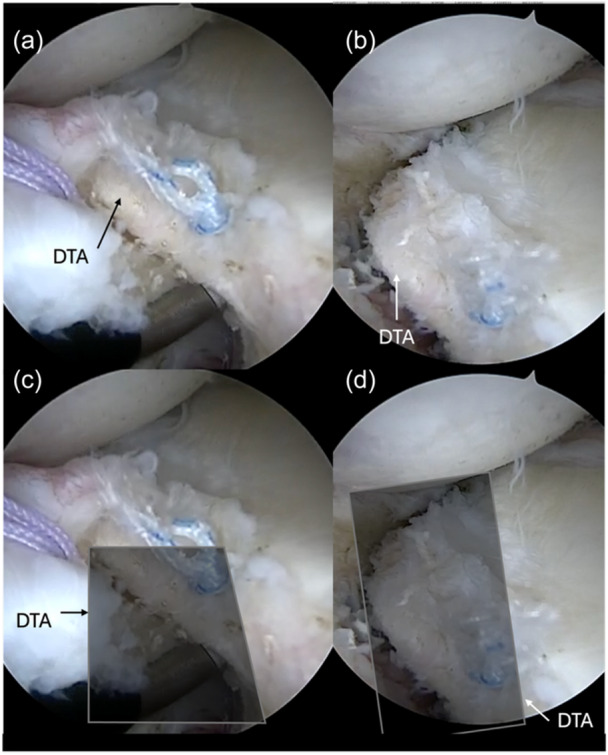 Figure 4
Figure 4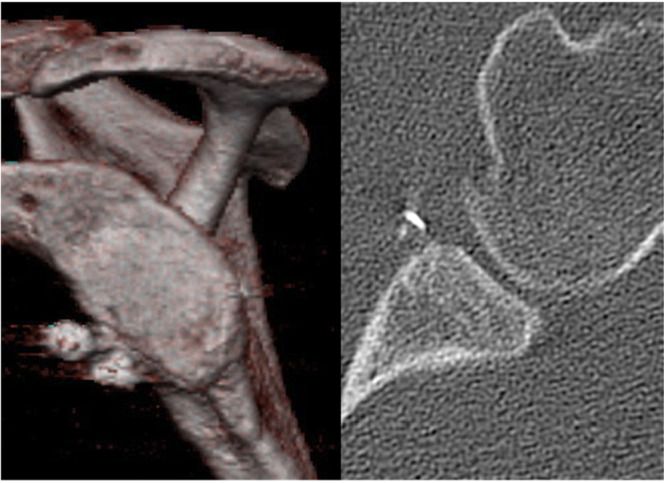 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Nerve Injury and Rehabilitation
INTRODUCTION
In the setting of anterior shoulder instability with critical glenoid bone loss (GBL), the use of a bony augmentation procedure is crucial to prevent recurrence and revision surgery. ‘Critical′ GBL is variably defined, but a defect as low as 10% GBL can be considered for a bony augmentation procedure [25, 60, 74, 91]. Recurrence rates have been reported up to 75% when arthroscopic Bankart repairs are performed in the presence of GBL > 25%, leading to subsequent recurrent dislocations and further glenoid erosion [26, 46]. Multiple bone grafts have been proposed to address GBL and restore the contour and surface area of the glenoid, providing mechanical stability and preventing recurrent dislocations.
Bone grafting procedures date back to the early 1900s and have continued to develop since then [28, 45]. These procedures vary in technique and can be open or arthroscopic, and with an auto‐ or allograft. Autografts for shoulder instability commonly include a coracoid transfer in the Bristow and Latarjet procedures [54], as well as iliac crest bone graft transfer (ICBGT) [79], distal clavicle autograft [82], and scapular spine [71]. Allografts include the iliac crest allograft [51], and distal tibial allograft (DTA) [69, 88], which has become an increasingly popular technique for addressing recurrent anterior shoulder instability with GBL. These auto‐ and allograft techniques make up key surgical procedures to re‐establish shoulder stability by recreating the glenoid track following traumatic and/or recurrent instability [16].
During surgery, the bone grafts are placed against the native glenoid, in continuity with the articular surface, and over time the graft undergoes biological remodelling, during which resorption can occur, defined as the extent the added bone integrates into the natural bone over time [33, 34, 72]. Resorption typically stabilises once the graft maintains a normal‐appearing cortical outline in both axial and en‐face views where healing has occurred and remodelling has plateaued [22]. At this final stage, the graft′s structure supports long‐term joint stability and function.
As the use of auto‐ and allografts have become more popularly studied, concerns are highlighted regarding graft osteolysis or resorption [23, 87]. For example, Delgado et al [23] studied four bone augmentation techniques and reported graft osteolysis in 100% of the iliac crest allograft group, 50% in the iliac crest autograft group, 20% following open Latarjet, and 0% following arthroscopic Latarjet. High resorption can have possible surgical and clinical implications, such as prominent hardware leading to pain, stiffness, or instability recurrence [75]. Understanding how different grafts integrate into the anterior glenoid rim in the setting of a bony augmentation procedure is essential to optimise patient outcomes, reduce graft failure, and guide surgical decision making. This paper aims to evaluate resorption characteristics and define remodelling in the setting of bone grafting in shoulder instability using both autografts (i.e., iliac crest and coracoid process) and allografts (i.e., iliac crest and DTA).
Defining and measuring glenoid bone loss
Anterior GBL is one of the most important risk factors for recurrent dislocation; therefore, accurate GBL measurement is crucial in guiding treatment decisions. Advanced imaging with computed tomography (CT) is essential, with three‐dimensional (3D) reconstruction being preferred [42]. Multiple validated techniques have been described to quantify the amount of GBL [43, 53, 66, 70], however inconsistency exists in the literature for reporting GBL due to methodological variation [52, 84, 86]. Low inter‐rater reliability is particularly problematic when measuring GBL by drawing a circle of ‘best‐fit’, where size and placement of this circle on the correct area of cortical bone can be difficult [55]. To develop a more reproducible method for measuring GBL, our group investigated normal glenoid morphology and found a direct relationship between the superior‐inferior distance of the glenoid and the anterior‐posterior glenoid width [70]. By utilising the superior‐inferior and anterior‐posterior measures from the en‐face view of the 3D reconstructed CT, we can reproducibly determine the amount of glenoid missing using the formula: 0.70**H* + 2.53; where H = superior‐inferior glenoid height [41, 70] (Figure 1). From this estimation, we can use a surface area calculation to determine amount of bone missing [8, 67].
Measurement of glenoid bone loss (GBL) using 3D reconstruction and en‐face view demonstrating superior‐inferior (SI, 40 mm) and anterior‐posterior (AP, 24 mm) measurement. Estimated AP glenoid = [0.70 * (40 mm) + 2.53] = 30.53 mm.
Graft options and surgical techniques
Autografts
Coracoid autograft
The Latarjet procedure is one of the most common autograft‐based procedures and historically has been considered the gold standard for treatment of recurrent instability with GBL. The coracoid process is harvested and transferred to the anterior rim of the glenoid to restore the bony architecture, as well as providing a ‘sling effect’ of the conjoint tendon, restoring shoulder stability [32, 54]. The Latarjet procedure was initially described with the use of two screws; however, recently the use of suspensory fixation has been advocated as an alternative technique [13]. Long term follow‐up of the Latarjet show low rates of recurrent instability, especially compared to the soft‐tissue stabilisation procedures [4, 6, 7, 44, 47, 77], but with variable complication reporting in both arthroscopic and open approaches [47]. Reported complications of the open Latarjet range from 7% to 30% [2, 21, 39], with arthroscopic Latarjet procedures having a similar rate (8.4%–23.4%) [18, 27, 44, 58]. While studies vary on what complications are considered, commonly reported complications include screw mispositioning, nerve injury, non‐union, and resorption [40].
Iliac crest bone autograft
The use of an iliac crest bone autograft transfer (ICBGT) has been previously described utilising a bicortical autograft attached via suspensory fixation methods or screws [5, 79]. The ICBGT is a free bone alternative that achieves anatomic glenoid reconstruction without the use of the sling effect. ICBGT has shown comparable outcomes to the Latarjet procedure, including clinical outcomes, frequency of recurrent dislocations, and complication rates [10, 62]. Recurrent instability and complications are reportedly low (<5%), which includes the rate of hardware complications [10, 56].
Distal clavicle autograft
The use of a distal clavicle autograft has been described previously for its combination of being readily available (i.e., harvested from the patient) and osteochondral properties [81]. Tokish in 2014 describes it to compare favourably with the coracoid for its size (‘thickness and bulk’).
Scapular spine autograft
The scapular spine autograft is another option but similar to the distal clavicle autograft is not commonly used. The differentiating advantage of the scapular spine autograft is the donor site is in the same area of arthroscopic portals thereby reducing multisite morbidity [90]. Moroder et al. presented a technical note describing a cerclage technique using a tricortical scapular spine autograft [61]. There is limited research on patient outcomes, but one study with a small sample size shows significant patient reported improvements post‐operatively, with minimal complications and re‐dislocations [90].
Allografts
Distal tibial allograft
The DTA was first introduced by Provencher et al. [69], and has emerged as an alternative to traditional coracoid or iliac crest transfers and chosen for its anatomical fit to the distal glenoid, with dense cortical bone and a native cartilaginous surface that closely conforms to the humeral head [69]. Wong and Urquhart [88] described Arthroscopic Anatomic Glenoid Reconstruction (AAGR), a subscapularis‐sparing arthroscopic technique for reconstruction of the anterior glenoid with DTA [9, 69, 87]. AAGR with DTA has since resulted in positive patient outcomes, low recurrence rates, and low complications [3, 48, 83, 87, 89]. The use of a DTA in an open or arthroscopic approach still has reported complications, albeit low (3.75%) [75], with concerns about the consistency of graft incorporation and the potential for resorption.
Iliac crest allograft
The implantation technique for iliac crest allografts closely resembles that of autografts, except that harvesting from the patient is not required. Few studies examine the implication of iliac crest allografts and non‐rigid fixation methods [78, 79]. This approach has highlighted good patient outcomes, with minimal rates of recurrence, and high optimal graft position and healing rates >90% [80, 92].
Graft resorption
Defining and measuring graft resorption
Graft resorption is a known complication of all bone grafting techniques; however, there is some confusion between normal or expected resorption (resulting in remodelling) and excessive graft resorption (resulting in graft failure). Resorption is the process of the breakdown and removal of bone whereas remodelling is the process of bone being rebuilt and reshaped [33, 34, 72]. Complete resorption is referred to as osteolysis [1]. Often studies report on union or non‐union of the graft as well, which outline the healing of the graft to the native glenoid. A CT scan is the gold standard measurement tool for graft resorption. Views in both the axial and en‐face planes are used to evaluate graft morphology, cortical continuity, and overall volume (Figure 2). Multiple techniques to meausure graft resorption exist [36, 93]. Zhu et al. [93] proposed a classification system using axial CT where resorption was assessed based on the degree of screw exposure, ranging from ‘Grade 0’ as the screw head buried in the graft to ‘Grade III’ as the screw head and shaft are completely exposed with no bone left on the glenoid neck [93].
(a) Three‐dimensional computed tomography (CT) scan en‐face view. (b) Axial two‐dimensional CT scan view of a right shoulder demonstrating continuous cortical structure with the native glenoid. In (b) the anterior rim of the glenoid is in continuity in the axial plane, and the glenoid surface is curved and lacks discontinuity, often seen as sharp angles where the graft was inserted. (c) and (d) Estimation of where the graft would have been placed, to highlight its remodelling. DTA, distal tibia allograft; G, glenoid.
Conversely, when suspensory fixation is used, resorption can be evaluated by comparing the dimensions of a perfect circle on immediate post‐op CT and final CT scans [14]. However, neither of these methods provide information about graft stability or indicate when graft remodelling is complete. Instead, graft stability can be inferred when the cortical outline of the glenoid surface appears continuous and anatomically restored on both the axial and en‐face CT scan (Figure 2) [22]. We define this radiographic appearance as indicative of full remodelling, suggesting that the graft has integrated and the glenoid structure is unlikely to undergo further change, unless a re‐dislocation occurs, impacting the remodelled anterior glenoid rim.
Research and clinical expertise point to the fact that resorption will occur to some level when using an autograft or allograft [22, 23, 59, 87]. Authors attribute resorption and remodelling following bone augmentation to Wolff′s law, a ‘hot topic’. In its simplest form, Wolff′s law states that a bone adapts to the loads under which it is placed [33, 34]. Following a bony procedure for GBL, Wolff′s law would hold true if enough load is applied at the level of the glenohumeral joint to adapt. Therefore, the surface of the glenoid will reshape to its natural form under stress [20]. In bony procedures, it is important to place the graft accurately. A medially placed graft could increase the resorption due to inadequate mechanical stress placed across the graft. Conversely, a laterally placed graft has the potential to increase the joint forces and thereby lead to arthritis. In addition to mechanical loading being a factor in graft resorption, biological factors, including poor vascularisation, immune response, and reduced osteogenic potential of the graft can influence the level of resorption [11, 38, 87].
Autograft resorption
Graft resorption for the Latarjet with coracoid autograft transfer is variable, where complete resorption has been reported to be as low as 5% [19], and as high as 100% [23, 77, 93]. In one example, Tanaka et al. [77] reported 100% incidence of bone resorption following the Latarjet procedure with screw fixation in rugby players. By one year, all cases showed resorption at the superior screw (severe in 50%), while only 20% showed resorption at the inferior screw [77]. Moreover, open Latarjet procedures with screw fixation have reported high rates of graft union (88‐100%) [50, 76], but one study has shown about 12% non‐union [50]. When comparing these results to the arthroscopic Latarjet procedure with screw fixation, healing or union is reportedly similar [37, 50, 85], but Kordasiewicz et al. showed less non‐union (1.7%) and development of osteolysis (0%) in arthroscopic procedures [50]. However, it is important to note that while higher non‐union was reported following open Latarjet, compared to the arthroscopic Latarjet with screws, the follow‐up was more than twice as long in the open group, giving more time for resorption or osteolysis to occur.
This resorption phenomenon further differs regarding screw or suture button fixation across Latarjet procedures. Some literature supports superior graft healing and union rates when rigid‐screw fixation was used, with follow up ranging from 6 months to 3 years [15, 37, 63, 85]. However, higher resorption or osteolysis is often reported when screw fixation is used [37, 63, 85]. Di Giacomo et al. explain that increasing compression is not enough to achieve less coracoid bone graft osteolysis [35], whereas Wang et al. describe that the more flexible fixation pattern of suture buttons helps with good bone contact with less compressive stress, leading to union and, not necessarily osteolysis [85].
Following ICBGT procedures, Boehm et al. [12] in a series of 14 patients had CT imaging confirm complete graft ‘consolidation’ in all cases, with an initial overcorrection of glenoid surface area that remodelled over time toward a normal anatomic shape, indicating successful graft remodelling without significant resorption. Additionally, in a small cohort (n = 11), Wong et al. [64] found that six patients exhibited <25% resorption, four experienced 25%–50% resorption, and one experienced >50% resorption. These findings align with Delgado et al. [23] who reported that approximately half of their patients had >20% of graft resorption. These results suggest that while varying degrees of graft resorption are common following ICBGT, the remodelling process is often sufficient to restore glenoid anatomy. Importantly, the presence of resorption does not appear to compromise clinical outcomes, underscoring the robustness of the technique.
Allograft resorption
Graft union and resorption are critical considerations in the success of DTA augmentation for anterior shoulder instability. In a recent meta‐analysis, Singh et al. [75] highlighted 36.47% prevalence of graft resorption across eight DTA studies. In one of the earliest clinical reports, Provencher et al. [69] described an open anatomic glenoid reconstruction with DTA in 10 patients with recurrent instability and significant GBL. At a minimum 15‐month follow‐up, all grafts appeared to be united radiographically, and no cases of significant resorption were identified, although a major limitation was that CT imaging was not systematically used. In a larger cohort of 41 patients, Provencher et al. [68] used CT imaging and revealed full graft union in 87% of patients, but 41% exhibited some degree of graft resorption, typically at the anterior‐inferior margin. Amar et al. reported low levels of resorption at short‐term (6.31 months) follow‐up of an arthroscopic DTA technique with rigid screw fixation using CT imaging, supporting DTA′s potential for stable osseointegration [3]. Specifically, full osseous union was achieved in 83% of patients, while 17% showed partial union. Importantly, resorption was minimal, with 87% of grafts maintaining >75% of original volume. This study highlighted the role of arthroscopic technique and rigid fixation in promoting graft stability and minimising resorptive change [3]. Similarly, Wong et al. [89] reported on 35 patients with CT assessment at a mean of 12.8 months. They observed complete graft union in 91% of patients and partial resorption in 14%, with only 6% demonstrating >25% volume loss [89].
In comparison, resorption following fixation of iliac crest allograft, either using screws or non‐rigid suture button fixation, reveal high resorption rates [11, 23, 29, 92]. In Espejo Reina et al. and Delgado et al., with study samples of 14 and 10, respectively, arthroscopic iliac crest allograft fixation using suture buttons resulted in over 90% of the population having >20% of resorption and high rates of osteolysis [23, 29]. When screws are used for fixation of the iliac crest allograft, Boehm et al. reported ‘excessive’ graft resorption [11], and Mascarenhas et al. highlighted that 80% had osseous union at six months follow up and only 20% demonstrating some degree of osteolysis [57]. The lower resorption rates observed with DTAs compared to iliac crest allografts may be attributed to the osteochondral composition of the DTA, which allows restoration of the articular hyaline cartilage surface, in contrast to the osseous iliac crest graft [17, 73].
Recurrent instability remains low when using DTA in an open or arthroscopic approach [68, 75, 83, 89]. Tucker et al. reported a significantly lower rate of recurrent instability in DTA patients (5%) compared to those undergoing Bankart repair (27%), suggesting that even in the presence of partial resorption, clinical stability can be maintained [83]. In the short to medium term (<2 years) Wong et al. and Singh et al. found that functional scores were high, and recurrence rates remained low, again when partial resorption was observed [75, 89]. Boehm et al. concur with these results showing no re‐dislocations [11]. This finding may be due to the restoration of the glenoid arc and capsulolabral tension, which remain protective against dislocation [11]. Furthermore, it has been suggested that re‐dislocation rates remain low despite the high resorption, particularly seen in the iliac crest allograft due to the formation of stabilising scar tissue [11]. However, severe or progressive resorption may compromise the graft′s ability to prevent humeral head translation, particularly in high‐demand athletes [32]. In these DTA and iliac crest allograft studies, clinical outcomes remained favourable, with minimal subluxations or dislocations throughout the studies leading authors to conclude that resorption did not correlate with clinical failure or recurrence [11, 29, 68, 87].
Allograft vs. autograft
Comparisons between graft types have also shed light on their behaviour over time. Wong et al. [87] performed a radiographic analysis comparing coracoid autograft and DTA reconstructions. In the DTA group, mean graft volume decreased by 11.8% from immediate postoperative imaging to final follow‐up (average 13.4 months), while the coracoid group showed only a 3.2% decrease. In a matched cohort study, Frank et al. [30] found radiographic evidence of partial resorption in 39% of DTA grafts versus only 11% of Latarjet grafts. Similarly, in a direct comparison study, Delgado et al. showed allograft bone (iliac crest) had greater resorption than that of the iliac crest autograft or open and arthroscopic Latarjet procedures [23]. These findings underscore the importance of understanding the biological behaviour of allograft and autograft bone, particularly the remodelling potential of non‐vascularised constructs such as distal tibial or iliac crest grafts. While both allograft‐based (e.g., DTA) and autograft‐based (e.g., Latarjet) procedures are susceptible to osteolysis [36, 49], the osteochondral nature of DTA may better replicate the native glenoid contour and reduce joint contact pressures [31]. In contrast, the coracoid graft benefits from partial preservation of vascularity through the conjoint tendon, which may mitigate resorption at its inferior aspect. Nonetheless, superior regions of the coracoid may remain prone to resorption due to limited vascularisation and mechanical loading. Ultimately, both techniques share comparable remodelling dynamics and remain vulnerable to partial graft resorption despite differing biological and mechanical characteristics.
Distal tibia allograft – remodelling timeline and factors
Biomechanical and imaging‐based studies offer further context on the timeline of the remodelling nature of bone grafts in the treatment of anterior shoulder instability. The application of Wolff′s law in DTA reconstruction was recently further explored by Dawe et al. [22], who demonstrated that resorption following AAGR with DTA results in a return to anatomic glenoid width by an average 6.9 months post‐operation. Their findings highlight that graft remodelling, consistent with Wolff′s law, plays a key role in restoring the native glenoid size and architecture.
Ultimately, radiographic studies have demonstrated that allografts undergo a natural remodelling process upon implantation, including vascular invasion, osteoclastic activity, and eventual incorporation [34]. However, this process is not always complete. Partial or even significant resorption of DTA has been documented, particularly in patients with poor graft fixation or suboptimal mechanical loading due to a medialized graft [75, 89]. Due to this variability, we highlight the importance of reporting final anterior‐posterior width of the graft and glenoid on a post‐operative CT at a minimum of 7 months following surgery [22], to define remodelling.
Understanding remodelling
While authors have reported rates of resorption and estimated amounts of bone loss following that resorption, less is reported on remodelling. We note from Wolff′s law that the bone will remodel based on the stress that is applied to it, and therefore, we would expect the glenoid to remodel back to the estimated native size, as determined using the superior‐inferior and anterior‐posterior methodology [70]. We define remodelling as stabilised or finished when the axial and en‐face views have complete normal cortical structure (Figure 2a,b) [22]. From these figures of a remodelled DTA, the bone graft is completely healed and remodelled back to both the size and shape of the normal glenoid. We suggest that reporting anterior‐posterior glenoid and graft dimensions are more clinically meaningful than focusing solely on the degree of resorption, as often described previously. The extent of resorption is largely influenced by the initial graft size, and oversized grafts tend to undergo more resorption but ultimately remodel to produce a glenoid of normal dimensions. We aim to discuss if and how we can influence remodelling and what we have learned through clinical and research applications of arthroscopic bone grafting with DTA for shoulder instability with anterior GBL.
Remodelling timeline and factors
The use of DTA in the management of anterior shoulder instability has evolved significantly since its initial open adaptation by Provencher et al. [69]. Through the development of AAGR with DTA [88], the early stages of DTA implementation involved larger grafts being used under the rationale that greater bone loss warranted more substantial bony reconstruction to restore glenoid concavity and stability (see Figure 3a). Early postoperative CT scans of these patients, typically obtained around 3‐months post‐operatively, did not show clear evidence of graft integration or remodelling (Figure 3b). This period, characterised by relatively static imaging findings, coincided with minimal patient symptoms highlighting that patients′ shoulders were now considered stable following this procedure. It wasn′t until closer to the 12‐month follow‐up that some patients began reporting symptoms potentially related to hardware irritation, prompting further imaging (Figure 3c).
(a) Pre‐operative, (b) early (4 months) post‐operative computed tomography (CT) scan, and (c) 13‐month post‐operative CT scan demonstrating increased remodelling over time and increased hardware prominence at final graft remodelling with dotted lines representing superior‐inferior measurement as 37.3 mm. Solid lines represent anterior‐posterior glenoid width measurements.
Follow‐up CT scans of these initial patients at the 12‐month mark revealed more substantial remodelling of the graft (see Figure 3c), with progressive rounding of the graft margins and cortical continuity suggestive of osseous integration. Axial images revealed restoration of the native glenoid concavity, with the grafts adopting a triangular morphology, which further indicated the remodelling process. In some cases, the initially oversized DTA grafts led to prominent screw heads becoming exposed as the bone remodelled (Figure 3c), contributing to anterior shoulder pain and stiffness. This occasionally necessitated secondary arthroscopic procedures, including hardware removal. In patients who required arthroscopic screw removal, a well‐integrated triangular shaped graft remained under the Bankart repair, confirming successful osseous integration (Figure 4). These findings prompted a shift toward using smaller, more anatomically matched grafts, particularly as clinical outcomes remained favourable despite partial graft resorption and re‐dislocation rates remained low [3, 83, 89]. This experience raised important biomechanical and biological considerations, including: how much graft is truly necessary to restore function, and to what extent can resorption be tolerable without compromising long‐term joint stability?
Remodelled distal tibia allograft (DTA) demonstrating (a) triangular remodelled shape axially and (b) continuity of the cortex and healing of the Bankart repair over the graft. (c) and (d) Overlay estimated graft placement to highlight remodelling.
Suspensory fixation has gained traction, largely for its ease of use in teaching environments and potential to minimise hardware‐related complications. However, comparing DTA fixation with screws and suspensory methods showed that on average, suspensory fixation results in greater bone resorption and subsequently smaller postoperative glenoid anterior‐posterior width than screw fixation (Figure 5) [65]. Additionally, these findings corresponded with an increased re‐dislocation rate compared to screw fixation. This finding contrasts with good long‐term outcomes achieved with suspensory fixation in the Latarjet procedure [24]. We theorise that due to the slower osseointegration of allograft compared to autograft, graft resorption and remodelling may occur before full incorporation to the anterior glenoid neck. This early remodelling could lead to de‐tensioning of the suspensory fixation, resulting in medial graft displacement and severe resorption. Moreover, suspensory fixation does not handle shear forces well, making it very difficult to recreate the glenoid′s concavity that normally helps load the graft and drive remodelling through Wolff′s law. Over time, this fixation method likely leads to graft erosion, increased subluxation events, recurrent bone loss, and possible redislocation. Despite these findings, questions persist regarding the long‐term implications of graft resorption and hardware design. For instance, does the type of screw or even its positioning impact remodelling? Could surface‐treated or bioresorbable screws mitigate complications without sacrificing stability?
Suspensory fixation method demonstrating high level of resorption where remodelled glenoid anterior‐posterior width remains smaller than estimated glenoid width.
Looking ahead, a key question remains: can we actively influence graft remodelling through surgical technique? With DTA, surgeons have control over both fixation method and graft size, variables that may shape the biological response and long‐term outcomes. In cases where full graft resorption occurs without recurrent instability, it is often because there was no true bone loss to begin with. This nuance underscores the importance of appropriate patient selection and highlights the potential for tailoring surgical technique, such as opting for specific fixation methods or customising the graft size to optimise remodelling while minimising complications. As the field moves forward, refining these decisions could enhance surgical outcomes and personalise care for patients with shoulder instability.
CONCLUSION
Bony augmentation procedures may be considered in the setting of anterior shoulder instability with critical GBL. While the Latarjet procedure remains a widely used autograft technique, complications and graft resorption remain concerns. Meanwhile, DTA represents a biomechanically favourable alternative with excellent clinical outcomes. To better characterise graft remodelling, final glenoid width should be assessed with CT scans at least seven months post‐operatively to show when the cortex has remodelled to the native glenoid. Future studies should report not only resorption but also remodelling patterns across techniques and graft types and determine how these relate to long‐term outcomes and clinical failure.
AUTHOR CONTRIBUTIONS
All authors contributed to the conceptualisation and development of the manuscript. Sarah Remedios conducted the literature review and synthesised the evidence. The first draft was written by Sarah Remedios, and all authors critically reviewed and revised subsequent versions. All authors approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
Sarah Remedios declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Jillian Karpyshyn declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Dr. Ivan Wong reports a relationship with DePuy Mitek Inc that includes: consulting or advisory and speaking and lecture fees. Dr. Ivan Wong reports a relationship with Smith and Nephew Inc that includes: consulting or advisory and speaking and lecture fees. Dr. Ivan Wong reports a relationship with CONMED Corp that includes: consulting or advisory and speaking and lecture fees. Dr. Ivan Wong reports a relationship with Bioventus LLC that includes: speaking and lecture fees. Dr. Ivan Wong is an editorial board member for the American Journal of Sports Medicine (AJSM) and Arthroscopy: The Journal of Arthroscopic and Related Surgery (ARTH), and The HIVE Musculoskeletal Journal; and is a board of committee member for AANA, ISAKOS and AAC. Is an associate editor for the Orthopaedic Journal of Sports Medicine (OJSM). If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
ETHICS STATEMENT
There is no institutional review board (IRB) approval required for this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agarwal S . Osteolysis—basic science, incidence and diagnosis. Curr Orthop. 2004;18:220–231.
- 2Alkaduhimi H , Willigenburg NW , Wessel RN , Wolterbeek N , Veen EJD , Koorevaar RCT , et al. Ninety‐day complication rate based on 532 Latarjet procedures in Dutch hospitals with different operation volumes. J Shoulder Elbow Surg. 2023;32:1207–1213.36586507 10.1016/j.jse.2022.11.015 · doi ↗ · pubmed ↗
- 3Amar E , Konstantinidis G , Coady C , Wong IH . Arthroscopic treatment of shoulder instability with glenoid bone loss using distal tibial allograft augmentation: safety profile and short‐term radiological outcomes. Orthop J Sports Med. 2018;6:232596711877450.10.1177/2325967118774507 PMC 597139329854863 · doi ↗ · pubmed ↗
- 4An VVG , Sivakumar BS , Phan K , Trantalis J . A systematic review and meta‐analysis of clinical and patient‐reported outcomes following two procedures for recurrent traumatic anterior instability of the shoulder: Latarjet procedure vs. Bankart repair. J Shoulder Elbow Surg. 2016;25:853–863.26809355 10.1016/j.jse.2015.11.001 · doi ↗ · pubmed ↗
- 5Auffarth A , Schauer J , Matis N , Kofier B , Hitzl W , Resch H . The J‐bone graft for anatomical glenoid reconstruction in recurrent posttraumatic anterior shoulder dislocation. Am J Sports Med. 2008;36:638–647.18006673 10.1177/0363546507309672 · doi ↗ · pubmed ↗
- 6Aurich M , Hofmann GO , Best N . Clinical outcome and return to sports activity after surgical treatment for recurrent shoulder instability with a modified Latarjet procedure. Orthop Traumatol Surg Res. 2021;107:102977. 10.1016/j.otsr.2021.102977 34091084 · doi ↗ · pubmed ↗
- 7Bessière C , Trojani C , Carles M , Mehta SS , Boileau P . The open latarjet procedure is more reliable in terms of shoulder stability than arthroscopic bankart repair. Clin Orthop Relat Res. 2014;472:2345–2351.24615422 10.1007/s 11999-014-3550-9PMC 4079884 · doi ↗ · pubmed ↗
- 8Bhatia S , Saigal A , Frank RM , Bach BR , Cole BJ , Romeo AA , et al. Glenoid diameter is an inaccurate method for percent glenoid bone loss quantification: analysis and techniques for improved accuracy. Arthrosc ‐ J Arthrosc Relat Surg. 2015;31:608–614.e 1.10.1016/j.arthro.2015.02.02025842231 · doi ↗ · pubmed ↗