Endovascular repair of complex aortic aneurysms: comparison between surgeon-modified endografts and commercial branched devices in a high-complexity center
Roger Conde Moncada, Luis Mariano Ferreira, Ricardo La Mura, Oscar Dávila, W. Samir Cubas

TL;DR
This study compares two endovascular repair methods for complex aortic aneurysms and finds that one has lower mortality and fewer complications.
Contribution
The study provides a comparison of outcomes between surgeon-modified endografts and commercial branched devices in a high-complexity center.
Findings
PMEGs showed lower in-hospital mortality (5.3%) compared to t-BRANCH (23.1%), though not statistically significant.
ASA IV status and prior stroke were significant predictors of in-hospital mortality.
Both methods showed favorable results with low rates of reinterventions.
Abstract
El tratamiento endovascular de los aneurismas aórticos toracoabdominales y paraviscerales complejos, con el desarrollo de nuevos dispositivos, representa uno de los aspectos más desafiantes de la cirugía endovascular. El objetivo de este estudio fue describir la mortalidad perioperatoria a 30 días, las complicaciones mayores posoperatorias y las reintervenciones de los pacientes tratados por aneurismas aórticos complejos mediante dispositivos de endoprótesis ramificadas off-the-shelf (t-BRANCH) y Physician Modified Endografts (PMEGs). El presente trabajo es un estudio observacional, retrospectivo y unicéntrico sobre una base de datos prospectivamente recolectada de cada paciente tratado por aneurisma aórtico complejo registrado en la historia clínica de nuestro centro aórtico de referencia, entre enero de 2020 y diciembre de 2024. Se analizaron 51 pacientes con una media de edad de…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
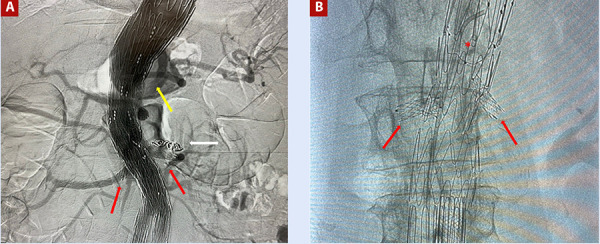 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Aortic aneurysm repair treatments · Infectious Aortic and Vascular Conditions
Introduction
Endovascular treatment of complex thoracoabdominal and paravisceral aortic aneurysms represents one of the most demanding challenges in endovascular surgery. The development of new devices for their appropriate management, such as fenestrated and branched endografts, has enabled successful treatment of patients with complex anatomy, multiple comorbidities, or contraindications to open surgery, achieving acceptable perioperative morbidity and mortality outcomes 1^,^2.
The availability of off-the-shelf branched endografts (t-BRANCH) has proven to be an effective and readily accessible alternative, owing to their standardised configurations, for the urgent or elective treatment of thoracoabdominal aneurysms 3. Conversely, in the absence of commercially available custom-made fenestrated devices (Custom Made Devices, CMDs), which typically require manufacturing times of approximately three months, some centres have developed advanced endovascular techniques such as physician-modified endografts (PMEGs) 4^-^7.
Globally, the study by Robaldo et al. showed that 34.4% of centres perform fewer than ten PMEG cases per year. Italy leads in utilisation, followed by the United States, Canada, and Austria; in Latin America, Brazil ranks first, followed by Colombia and Argentina. These findings highlight the limited availability of this technology in the region and underscore the importance of reporting institutional experiences 8.
The aim of this study was to describe 30-day perioperative mortality, major postoperative complications, and reinterventions among patients treated for complex aortic aneurysms using t-BRANCH devices and PMEGs, as well as the factors associated with these outcomes.
Materials and methods
Design and study population
This is an observational, retrospective, single-centre study based on a prospectively collected database including all patients treated for complex aortic aneurysms recorded in their medical records between January 2020 and December 2024 at our reference aortic centre, Clínica Sagrada Familia, located in Buenos Aires, Argentina. Patients treated for complex thoracoabdominal or paravisceral aneurysms using t-BRANCH or fenestrated endografts employing the PMEGs technique were included. Exclusion criteria comprised aortic repairs not involving fenestrated or branched endografts, hybrid surgeries, procedures converted to open surgery, and patients with incomplete follow-up (less than 30 days without available clinical or imaging data).
Data collection and variable assessment
Clinical, anatomical, technical, and perioperative data were collected retrospectively from electronic medical records and diagnostic imaging. Subsequently, a manual review was performed to validate the completeness and consistency of the collected information. Data were coded and organised in a structured database using Microsoft Excel and R software (Microsoft Corp., Redmond, WA, USA).
The following variables were considered in the present study: demographic data (age and sex); comorbidities (hypertension, diabetes mellitus, smoking status, dyslipidaemia, history of stroke, obesity, coronary artery disease, chronic obstructive pulmonary disease, among others); anatomical characteristics of the aorta (diameter, location, and extent of the aneurysm); type of device used (t-BRANCH or PMEGs); technical parameters (number of revascularised vessels); and clinical outcomes.
Perioperative mortality was also assessed and defined as any death occurring during the surgical procedure, within the first 30 days after the intervention, or during the index hospitalisation, regardless of the time elapsed since surgery or hospital discharge. Postoperative cardiovascular complications were defined as adverse postoperative events that significantly compromised the patient’s clinical status, including spinal cord ischaemia, stroke, myocardial infarction, renal failure, heart failure, and cardiogenic shock. Spinal cord ischaemia was defined as a new motor or sensory deficit occurring during or after the endovascular procedure. Reinterventions were defined as any additional endovascular procedure required to correct procedure-related complications, maintain patency of the endograft and its branches or fenestrations along their entire length, or treat new lesions identified during follow-up.
Procedure description
All procedures were performed in the catheterisation laboratory under general anaesthesia and involved invasive monitoring, including a radial arterial line and a central jugular venous catheter. Vascular access was obtained through surgical exposure, with an inguinal incision and layered tissue dissection to expose the common femoral artery, followed by appropriate vascular control using vessel loops. The same procedure was performed on the contralateral side. When the left subclavian artery was used, a left infraclavicular approach was employed. Percutaneous access was not used in any case. Preoperative planning included high-resolution computed tomographic angiography with centreline reconstructions and multiplanar analyses using Horos software (Horos Project, version 4.0.2) to assess aortic morphology and visceral vessel anatomy.
All interventions were guided by fusion imaging (Vessel Navigator, Azurion/Alura Xper FD20, Philips Healthcare) and intraoperative cone-beam computed tomography (Xpert-CT, Philips), allowing precise endograft deployment and accurate identification of target vessels.
In all cases, the type of endograft was selected after multidisciplinary discussion. In the t-BRANCH group, preloaded multibranched off-the-shelf endografts were used without modification. In contrast, in the PMEG group, the selected endografts were manually modified by the surgical team. Fenestrations were created intraoperatively and reinforced with radiopaque snares sutured using 5-0 polyester (Ethibond), followed by the creation of constraining ties; the devices were then re-sheathed for subsequent implantation in the patient.
With regard to the stents used to connect the branches or fenestrations to the visceral arteries (celiac trunk, superior mesenteric artery, and renal arteries), no single brand was specified; selection was based on operator preference.
After completion of each procedure, a final completion angiography was performed in all cases to confirm the correct positioning of the endograft, its extensions, and the stents deployed in the corresponding visceral vessels. The absence of type I or type III endoleaks was also assessed and addressed immediately when detected. Following the procedure, patients were transferred to the coronary care unit for postoperative management.
Patients underwent computed tomography angiography (CTA) prior to discharge to verify aneurysm exclusion, device integrity, and visceral vessel patency. In patients with renal insufficiency, non-contrast CT was performed. For follow-up, scheduled imaging was obtained at 6 and 12 months, followed by annual surveillance thereafter.
Ethical aspects
The present study was approved by the institutional ethics committee. As it did not involve additional interventions or direct contact with patients and used only anonymised clinical records, informed consent was not required. Confidentiality and ethical handling of the data were ensured at all times.
Statistical analysis
Quantitative variables were expressed as mean ± standard deviation or median (interquartile range), according to their distribution, while categorical variables were expressed as absolute frequencies and percentages. The chi-square test or Fisher’s exact test was used to compare proportions, and the Student’s t test or the Mann-Whitney U test was applied for continuous variables. A p-value <0.05 was considered statistically significant. To analyse predictors of adverse events, a multivariable logistic regression model was used, including variables with p <0.10 in the univariable analysis.
Statistical analyses were performed using R software and Microsoft Excel (Microsoft Corp., Redmond, WA, USA).
Results
Fifty-one patients who underwent endovascular repair of complex thoracoabdominal or paravisceral aortic aneurysms between January 2020 and December 2024 were included. Of these, 38 (74.5%) were treated with PMEGs and 13 (25.5%) with t-BRANCH. The mean age was 69.6 ± 10.3 years, and most patients were male (90.2%).
The most frequent comorbidities were hypertension (90.2%), smoking (76.5%), chronic obstructive pulmonary disease (78.4%), dyslipidaemia (52.9%), and coronary artery disease (47.1%). Diabetes mellitus was present in 27.5%, and a prior history of stroke in 2.0%. According to the American Society of Anesthesiologists (ASA) physical status classification, 70.6% were ASA III and 29.4% were ASA IV (Table 1).
Table 1. Baseline clinical characteristics of the study population.VariableOverall (n=51)PMEGs (n=38)T-BRANCH (n=13)Age (years), mean ± SD69.63 ± 10.3270.45 ± 8.267.23 ± 11.4Male sex46 (90.2%)33 (86.8%)13 (100%)Hypertension46 (90.2%)35 (92.1%)11 (84.6%)Smoking39 (76.47%)30 (78.95%)9 (69.23%)Dyslipidaemia27 (52.9%)20 (52.6%)7 (53.8%)Diabetes mellitus14 (27.5%)3 (7.9%)11 (84.6%)History of cancer36 (70.6%)26 (68.4%)10 (76.9%)Prior stroke1 (2.0%)0 (0%)1 (7.7%)Obesity38 (74.5%)31 (81.6%)7 (53.8%)Ischaemic coronary heart disease24 (47.1%)18 (47.4%)6 (46.2%)COPD40 (78.4%)29 (76.3%)11 (84.6%)Prior EVAR11 (21.6%)11 (28.9%)0 (0%)Prior TEVAR7 (13.7%)6 (15.8%)1 (7.7%)Peripheral arterial disease5 (9.8%)3 (7.9%)2 (15.38%)Prior ruptured aneurysm3 (5.9%)1 (2.6%)2 (15.38%)History of Marfan syndrome2 (3.92%)1 (2.63%)1 (7.69%)ASA III36 (70.6%)29 (76.3%)7 (53.8%)ASA IV15 (29.4%)9 (23.7%)6 (46.2%)Shaggy aorta2 (%)2 (%)0 (0%)In-hospital mortality5 (9.8%)3 (7.89%)2 (15.38%)Postoperative stroke4 (7.8%)2 (5.52%)2 (15.23%)Paraplegia0 (0%)0 (0%)0 (0%)Renal failure33 (64.7%)27 (71.1%)6 (46.2%)Aneurysm diameter (mm), mean ± SD66.1 ± 15.265.11 ± 13.671.0 ± 19.4Length of hospital stay (days), mean ± SD14.6 ± 3.214.03 ± 2.615.54 ± 3.6PMEGs: Physician-Modified Endografts. t-BRANCH: off-the-shelf branched endografts. COPD: chronic obstructive pulmonary disease. EVAR: endovascular abdominal aortic aneurysm repair. TEVAR: thoracic endovascular aortic repair. History of cancer: prior malignancy treated with survival >5 years. ASA: American Society of Anesthesiologists physical status classification. SD: standard deviation.
Seven patients (13.7%) had a history of prior thoracic endovascular aortic repair (TEVAR) and 11 (35.3%) had undergone previous endovascular abdominal aortic aneurysm repair (EVAR). In addition, 5.9% presented with ruptured aneurysms at admission (Table 1).
Before intervention, the mean aneurysm diameter was 66.1 ± 15.2 mm. According to anatomical classification, juxtarenal aneurysms were the most frequent (45.1%), followed by Crawford type IV (15.7%) and pararenal aneurysms (9.8%) (Table 2). Only two patients had Marfan syndrome, and two had aortic dissection.
Table 2. Aneurysm type.VariableFrequency (n)Percentage (%)Thoracoabdominal aneurysms
Crawford type I12.0Crawford type II35.9Crawford type III23.9Complex abdominal aneurysms
Crawford type IV815.7Suprarenal saccular12.0Infrarenal + type IA endoleak47.8Juxtarenal2345.1Juxtarenal + type IA endoleak23.9
Overall, in-hospital mortality was 9.8% Table 1). When comparing endograft types, early in-hospital mortality was higher in the t-BRANCH group (23.1%) compared with PMEGs (5.3%), although this difference did not reach statistical significance (p = 0.0977). Postoperative cardiovascular complications occurred in 7.9% of PMEG-treated patients and 7.7% of those treated with t-BRANCH, with no significant difference (p = 1.000) (Table 3). Only four patients experienced a postoperative stroke, and no cases of paraplegia were recorded (Table 1).
Table 3. Comparison between PMEGs and t-BRANCHVariablePMEGs (n = 38)t-BRANCH (n = 13)p-valuePostoperative cardiovascular complications3 (7.9%)1 (7.7%)1.000Early reintervention (<30 days)2 (5.3%)1 (7.7%)1.000 Early in-hospital mortality2 (5.3%)3 (23.1%)0.098 Length of hospital stay (days), mean ± SD14.03 ± 6.9715.54 ± 3.720.457 t-BRANCH: off-the-shelf branched endografts. PMEGs: Physician-Modified Endografts. SD: standard deviation.
Early reinterventions occurred in 5.3% of PMEG-treated patients and 7.7% of those treated with t-BRANCH (p = 1.000). There was no significant difference in mean hospital length of stay between PMEGs (14.0 ± 26.9 days) and t-BRANCH (15.5 ± 33.7 days) (Table 3).
To identify predictors of mortality, univariable analysis was performed (Table 4), identifying ASA IV physical status (odds ratio [OR] = 11.98; 95% confidence interval [CI]: 1.46-98.7; p = 0.022) and a history of stroke (OR = 13.07; 95% CI: 1.06-161.5; p = 0.043) as strong predictors of in-hospital mortality. In multivariable adjusted analysis, only a history of stroke remained independently associated with mortality (OR = 30.48; 95% CI: 1.58-1390.36; p = 0.034) (Table 5). Coronary artery disease and renal dysfunction were notable but did not reach statistical significance (p = 0.120 and p = 0.144, respectively). No associations were found between late complications and aneurysm diameter, renal dysfunction, or coronary artery disease.
Table 4. Univariable analysis of clinical characteristics predicting in-hospital mortality.VariableFrequency n (%)OR (95% CI)p-valueASA class IV (vs. ASA III)14 (27.5%)11.98 (1.46-98.7)0.022History of stroke (vs. no stroke)6 (11.8%)13.07 (1.06-161.5)0.043ICHD (vs. none)10 (19.6%)4.60 (0.68-31.1)0.120eGFR <60 mL/min/1.73 m² (vs. ≥60)8 (15.7%)4.11 (0.66-25.7)0.144History of cancer (vs. no history of cancer)3 (5.9%)0.00 (0.00-15.4)0.305Sex (male vs. female)32 (62.7%)0.50 (0.06-4.20)0.480Dyslipidaemia (vs. no dyslipidaemia)12 (23.5%)0.73 (0.08-6.58)1.000Diabetes Mellitus (vs. no Diabetes Mellitus)5 (9.8%)0.00 (0.00-8.94)1.000Obesity (vs. no obesity)9 (17.6%)1.18 (0.13-10.7)1.000Aortic dissection (vs. no aortic dissection)2 (3.9%)0.00 (0.00-20.2)1.000Previous endograft (vs. no previous endograft)4 (7.8%)0.00 (0.00-10.7)1.000OR: odds ratio. CI: confidence Interval. ASA: American Society of Anesthesiologists physical status classification. ICHD: ischaemic coronary heart disease. eGFR: estimated glomerular filtration rate (KDIGO).
Table 5. Multivariable logistic regression of key baseline characteristics of the study population.VariableAdjusted OR95% CI p-valueAge (per 1-year increase)1.07(0.89-1.39)0.563ASA class IV (vs. ASA III)4.54(0.21-192.06)0.352History of stroke (vs no history of stroke)30.48(1.58-1390.36)0.034ICHD (vs. none)3.95(0.34-95.87)0.297eGFR <60 mL/min/1.73 m² (vs ≥60)2.14(0.12-70.60)0.616OR: odds ratio. CI: confidence Interval. ICHD: ischaemic coronary heart disease. ASA: American Society of Anesthesiologists physical status classification. ICHD: ischaemic coronary heart disease. eGFR: estimated glomerular filtration rate (KDIGO).
The mean number of visceral stents used was 2.6 (range: 1-5) in PMEG-treated patients and 3.8 (range: 2-4) in those treated with t-BRANCH. PMEG devices required a mean of 2.7 fenestrations per patient, whereas t-BRANCH devices did not require fenestrations due to their branched design.
The incidence of postoperative endoleaks was higher in the t-BRANCH group (38.5%) compared with the PMEG group (13.2%). Although most were type II endoleaks, not all cases required immediate reintervention.
Discussion
This single-centre observational study describes our institution’s experience with the endovascular treatment of complex aortic aneurysms. The results demonstrate low in-hospital mortality and a low incidence of major complications and reinterventions, highlighting the safety and effectiveness of PMEGs and t-BRANCH devices in a highly complex setting. In Latin America, documented experience with endovascular treatment of complex aortic aneurysms remains limited, largely due to restricted access to commercial devices because of their high cost and the limited availability of technical expertise, underscoring the need for regional studies. Recent reports from Argentina have described encouraging outcomes with these devices, supporting the feasibility of these therapies even in the context of structural and logistical constraints 9^,^10. A report by Gómez et al. from Colombia on several cases treated with fenestrated endografts described a mortality rate of 10%, predominantly among patients with advanced renal disease, and a 10% rate of spinal cord ischaemia. Nevertheless, despite multiple comorbidities that precluded open surgery, follow-up outcomes were satisfactory 11.
PMEGs represent a valid alternative for the endovascular treatment of complex aneurysms. Although their use remains heterogeneous, there is a clear association between case volume and outcomes, as demonstrated in the report by O’Donnell et al., where PMEG performance was comparable to that of commercial devices 12. Higher procedural volumes are associated with improved outcomes in terms of mortality and complications.
The population in our study consisted predominantly of patients aged around 70 years, mostly men, a pattern consistent with reports from the United States and Europe, where male sex and smoking have been identified as significant risk factors for the development of abdominal aortic aneurysms 13^,^14. In many cases, these lesions are initially infrarenal; however, in our region, unlike countries with more robust healthcare systems, screening is less rigorous and preventive health culture is limited, contributing to delayed diagnosis.
Regarding comorbidities, hypertension, smoking, and dyslipidaemia predominated, findings consistent with other studies of patients treated with complex endografts in centres across the United States and Western Europe 6. The ASA classification was particularly relevant, as most patients classified as ASA IV belonged to the group that experienced mortality, emphasising the importance of optimising perioperative management in this subgroup.
The overall mortality in our series is consistent with that reported in comparable studies, such as the Norwegian multicentre study by Harda et al. (9%) 15 and the retrospective study by Kölbel et al. (8.5% in elective patients) 13. In the PMEG subgroup, mortality was 5.3%, slightly higher than that reported in the Zenith trial by Oderich et al. (1.5%) and by Starnes et al. (2%) 16^,^17. These differences may be explained by the fact that those studies included only juxtarenal aneurysms, whereas our cohort also included thoracoabdominal and paravisceral aneurysms. In the t-BRANCH group, early in-hospital mortality was 23.1%, without reaching statistical significance, likely due to greater anatomical complexity and the small sample size in this subgroup. Georgiadis et al. reported mortality rates of 3.2% for off-the-shelf devices and 1.1% for PMEGs, confirming the safety of both strategies in elective and urgent settings 18. Overall, an early in-hospital mortality rate of 5.3% for PMEGs appears acceptable and comparable to international series, despite the limited number of cases.
In terms of neurological complications, Juszczak et al. reported a paraplegia rate of 1.9% in patients treated with PMEGs, attributed to their spinal cord protection protocol and staged repair with temporary aneurysm sac perfusion 19, findings comparable to ours, as our centre also performs staged repair. For t-BRANCH, spinal cord ischaemia remains the main concern. A meta-analysis by Konstantinou et al. reported a rate of 12.2% (95% CI: 4.1%-23.2%), with only one case of major stroke (20), figures consistent with our experience.
Regarding reinterventions, the t-BRANCH group showed a rate of 7.7%, similar to that reported in the European meta-analysis (5.7%; 95% CI: 1.7%-11.4%) 22, whereas the PMEG group had a rate of 5.3%, lower than the 13.8% reported in a multicentre study of 1,274 patients 21, likely reflecting differences in sample size.
Among predictors of mortality, ASA IV physical status (OR = 11.98; 95% CI: 1.46-98.7; p = 0.022) and a history of stroke (OR = 13.07; 95% CI: 1.06-161.5; p = 0.043) were identified as significant factors. Although not statistically significant, coronary artery disease and arterial dysfunction warrant attention, as they may be associated with increased perioperative risk, as demonstrated in the multicentre study by Tsilimparis et al., which identified peripheral arterial disease and reduced glomerular filtration rate as independent predictors of major adverse events 21.
Our findings are comparable with those of the most recent multicentre study from the International Multicenter Aortic Research Group, which included 27 centres and 3,634 patients treated for thoracoabdominal aortic aneurysms with fenestrated endografts, reporting a 5% in-hospital mortality rate and a significantly higher rate of adverse events in low-volume centres (fewer than 11 cases) compared with high-volume centres (33% vs. 20%; p<0.001). Similar predictors of mortality were identified, including age, chronic kidney disease, ASA class ≥3, prior aortic repair, symptomatic or ruptured aneurysm, and Crawford types I-III 22.
With regard to reinterventions, although they were more frequent in the t-BRANCH group, no major complications were observed after correction, except for type II endoleaks managed on an outpatient basis, confirming the effectiveness of both procedures.
The main limitations of this study include its single-centre design and small sample size, particularly in the off-the-shelf device subgroup, which limits statistical power to detect significant differences between groups. In addition, the lack of randomisation and device selection based on availability and anatomical characteristics may introduce selection bias.
In conclusion, endovascular repair of complex thoracoabdominal and paravisceral aortic aneurysms using PMEGs and t-BRANCH devices yields comparable outcomes in terms of mortality and major postoperative complications, with a low rate of reintervention. Although outcomes tended to favour PMEGs, with lower mortality and reintervention rates, albeit without statistical significance, both devices proved effective, even in urgent settings. These findings underscore the need for multicentre series and regional registries to further validate these results.
Figure 1. Image A shows a branched endograft to the coeliac trunk (yellow arrow), superior mesenteric artery, and renal arteries (red arrows), with additional embolisation of the left polar artery (white arrow). Image B demonstrates a surgeon-modified endograft with a scallop for the superior mesenteric artery (red asterisk) and two fenestrations for the renal arteries (red arrows).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wanhainen A Van Herzeele I Bastos F Bellmunt S Berard X Boyle JR European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms Eur J Vasc Endovasc Surg 202467219233110.1016/j.ejvs.2023.11.00238307694 · doi ↗ · pubmed ↗
- 2Pratesi C Esposito D Apostolou D Attisani L Bellosta R Benedetto F Guidelines on the management of abdominal aortic aneurysms updates from the Italian Society of Vascular and Endovascular Surgery (SICVE)J Cardiovasc Surg (Torino)202263332835210.23736/S 0021-9509.22.12330-X 35658387 · doi ↗ · pubmed ↗
- 3Gallitto E Faggioli G Spath P Pini R Mascoli C Logiacco A Urgent endovascular repair of thoracoabdominal aneurysms using an off-the-shelf multibranched endograft Eur J Cardiothorac Surg 20226151087109610.1093/ejcts/ezab 55334964451 · doi ↗ · pubmed ↗
- 4Gallitto E Faggioli G Spath P Pini R Mascoli C Ancetti S The risk of aneurysm rupture and target visceral vessel occlusion during the lead period of custom-made fenestrated/branched endograft J Vasc Surg 2020721162410.1016/j.jvs.2019.08.27332063442 · doi ↗ · pubmed ↗
- 5Gouveia E Melo R Fernández Prendes C Caldeira D Stana J Rantner B Wanhainen A Systematic Review and Meta-analysis of Physician Modified Endografts for Treatment of Thoraco-Abdominal and Complex Abdominal Aortic Aneurysms Eur J Vasc Endovasc Surg 2022642-318819910.1016/j.ejvs.2022.04.01535483575 · doi ↗ · pubmed ↗
- 6Chait J Tenorio ER Hofer JM De Martino RR Oderich GS Mendes BC Five-year outcomes of physician-modified endografts for repair of complex abdominal and thoracoabdominal aortic aneurysms J Vasc Surg 202377237438510.1016/j.jvs.2022.09.01936356675 · doi ↗ · pubmed ↗
- 7Oderich GS Commentary Physician-Modified vs Off-the-Shelf Fenestrated and Branched Endografts: Is This a Fair Comparison?J Endovasc Ther 201623111011410.1177/152660281561352026763258 · doi ↗ · pubmed ↗
- 8Robaldo A Ruffino MA Garbero E Amrein E Giovannacci L Giorno del R Indications, planning, and technical aspects in physician-modified endografts based on a cross-sectional global survey J Vasc Surg 202582376076910.1016/j.jvs.2025.05.01940404023 · doi ↗ · pubmed ↗