Association between HDL-cholesterol subfractions and the risk of major adverse cardiac and cerebrovascular events in patients with acute myocardial infarction: a single-center retrospective observational study
Yu Geng, Xingfei Deng, Yajun Xue, Bin Wang, Qing Liu, Tingting Lv, Changhua Lv, Yifei Wang, Ping Zhang

TL;DR
This study found that higher levels of HDL-3 cholesterol are linked to lower risk of major heart and brain events in patients who had a heart attack.
Contribution
The study identifies HDL-3 as a potential biomarker for cardiovascular risk and therapeutic target in acute myocardial infarction patients.
Findings
Patients with higher HDL-3 levels had significantly lower incidence of major adverse cardiac and cerebrovascular events.
HDL-3 showed discriminative ability for MACCE risk with an AUC of 0.62.
The Gensini score partially mediated the relationship between HDL-3 and MACCEs.
Abstract
This study aimed to evaluate the association between high-density lipoprotein (HDL) subfractions and long-term major adverse cardiac and cerebrovascular events (MACCEs) in patients with acute myocardial infarction (AMI). A total of 1,240 AMI patients admitted to Beijing Tsinghua Changgung Hospital between 2017 and 2023 were included. HDL subfractions, including HDL-2b and HDL-3, were quantified using microfluidic chip electrophoresis. Patients were stratified into tertiles according to HDL-3 levels. The primary endpoint was the occurrence of MACCEs. Kaplan–Meier analysis, Cox proportional hazards models, restricted cubic spline (RCS), and mediation analyses were performed to evaluate the associations between HDL subfractions and MACCEs. During a median follow-up of 52.4 months, 132 MACCEs (10.7%) occurred. Patients in the highest HDL-3 tertile had a lower MACCEs incidence than those…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1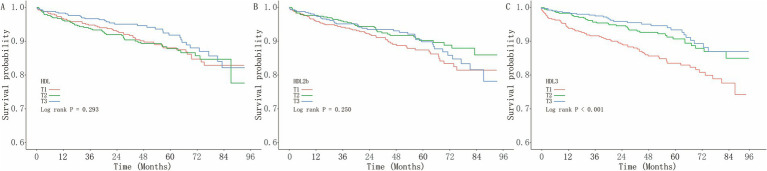 Figure 2
Figure 2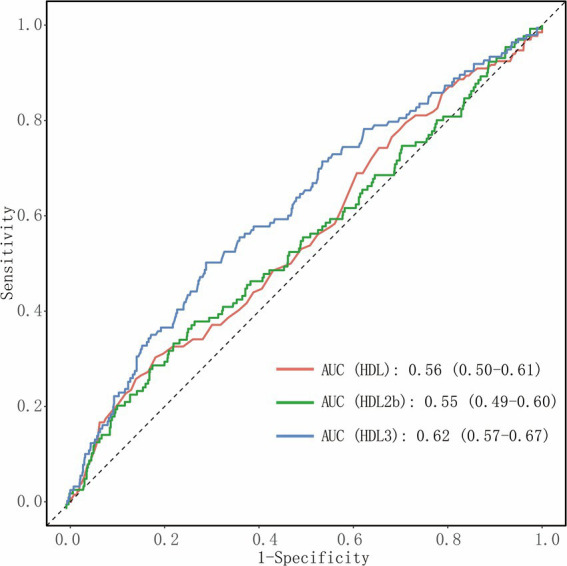 Figure 3
Figure 3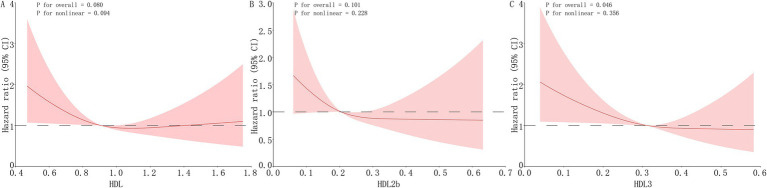 Figure 4
Figure 4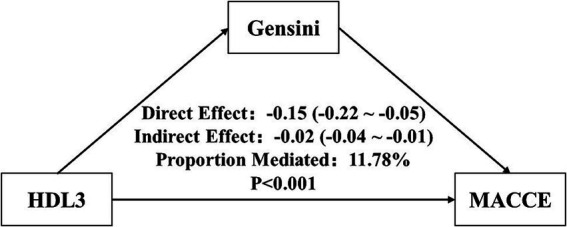 Figure 5
Figure 5| Variables | Total ( | Low ( | Medium ( | High ( |
|
|---|---|---|---|---|---|
| Age, years | 64.00 (55.75, 72.00) | 65.00 (56.00, 76.00) | 62.00 (55.00, 71.00) | 63.00 (54.00, 71.00) | 0.001 |
| Age category, years | 0.018 | ||||
| <45 | 112 (9.03) | 34 (8.31) | 44 (10.43) | 34 (8.31) | |
| 45–60 | 555 (44.76) | 159 (38.88) | 200 (47.39) | 196 (47.92) | |
| ≥60 | 573 (46.21) | 216 (52.81) | 178 (42.18) | 179 (43.77) | |
| Female | 311 (25.08) | 89 (21.76) | 116 (27.49) | 106 (25.92) | 0.146 |
| Hypertension | 869 (70.08) | 285 (69.68) | 291 (68.96) | 293 (71.64) | 0.685 |
| Diabetes mellitus | 525 (42.34) | 184 (44.99) | 177 (41.94) | 164 (40.10) | 0.360 |
| CKD | 214 (17.26) | 98 (23.96) | 58 (13.74) | 58 (14.18) | <0.001 |
| Statin use | 1,130 (91.13) | 367 (89.73) | 391 (92.65) | 372 (90.95) | 0.330 |
| HDL, mmol/L | 0.91 (0.77, 1.08) | 0.78 (0.67, 0.96) | 0.87 (0.77, 1.00) | 1.03 (0.91, 1.21) | <0.001 |
| HDL2b, mmol/L | 0.20 (0.15, 0.27) | 0.18 (0.13, 0.25) | 0.20 (0.15, 0.26) | 0.23 (0.18, 0.31) | <0.001 |
| HDL3, mmol/L | 0.31 (0.25, 0.38) | 0.22 (0.17, 0.25) | 0.31 (0.29, 0.33) | 0.40 (0.38, 0.45) | <0.001 |
| CRP, mg/L | 4.63 (1.77, 10.30) | 7.17 (3.00, 20.59) | 4.15 (1.89, 9.07) | 3.13 (1.40, 6.88) | <0.001 |
| TC, mmol/L | 4.31 (3.58, 5.05) | 3.92 (3.33, 4.66) | 4.34 (3.65, 5.00) | 4.66 (3.90, 5.37) | <0.001 |
| LDL, mmol/L | 2.72 (2.08, 3.44) | 2.47 (1.90, 3.07) | 2.78 (2.13, 3.47) | 2.97 (2.25, 3.71) | <0.001 |
| PLT, 10^9/L | 215 (176, 252) | 203 (168, 247) | 223.50 (189, 255) | 214 (182, 254) | <0.001 |
| HbA1c, % | 6.20 (5.70, 7.60) | 6.20 (5.60, 7.65) | 6.25 (5.70, 7.60) | 6.20 (5.70, 7.40) | 0.830 |
| eGFR, mL/min/1.73 m2 | 91.76 (71.97, 102.80) | 87.05 (62.85, 101.13) | 93.91 (78.48, 103.89) | 92.72 (74.09, 103.16) | <0.001 |
| Gensini score | 52.00 (28.00, 82.38) | 58.00 (32.62, 90.00) | 52.00 (28.00, 80.00) | 48.00 (25.00, 80.00) | 0.002 |
| MACCE, | 132 (10.65) | 67 (16.38) | 38 (9.00) | 27 (6.60) | <0.001 |
| Death, | 42 (3.39) | 22 (5.38) | 11 (2.61) | 9 (2.20) | 0.023 |
| Re-MI, | 57 (4.60) | 29 (7.09) | 17 (4.03) | 11 (2.69) | 0.009 |
| Stroke, | 21 (1.69) | 11 (2.69) | 6 (1.42) | 4 (0.98) | 0.144 |
| Bleeding, | 12 (0.97) | 5 (1.22) | 4 (0.95) | 3 (0.73) | 0.826 |
| Variables | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| |
| HDL | ||||||
| Low | Reference | Reference | Reference | |||
| Medium | 1.04 (0.70–1.54) | 0.861 | 0.95 (0.64–1.41) | 0.796 | 1.03 (0.69–1.54) | 0.888 |
| High | 0.75 (0.48–1.16) | 0.193 | 0.57 (0.36–0.89) | 0.014 | 0.64 (0.40–1.02) | 0.060 |
| 0.212 | 0.015 | 0.066 | ||||
| Per 0.1 mmol/L increase | 0.97 (0.90–1.04) | 0.357 | 0.93 (0.86–0.99) | 0.043 | 0.95 (0.88–1.02) | 0.151 |
| HDL-2b | ||||||
| Low | Reference | Reference | Reference | |||
| Medium | 0.71 (0.46–1.07) | 0.100 | 0.61 (0.40–0.93) | 0.023 | 0.68 (0.45–1.04) | 0.078 |
| High | 0.83 (0.55–1.25) | 0.370 | 0.58 (0.38–0.88) | 0.010 | 0.65 (0.43–1.00) | 0.050 |
| 0.336 | 0.010 | 0.047 | ||||
| Per 0.1 mmol/L increase | 0.92 (0.78–1.10) | 0.373 | 0.81 (0.68–0.97) | 0.020 | 0.86 (0.72–1.03) | 0.093 |
| HDL-3 | ||||||
| Low | Reference | Reference | Reference | |||
| Medium | 0.56 (0.37–0.83) | 0.004 | 0.62 (0.42–0.93) | 0.022 | 0.76 (0.50–1.14) | 0.186 |
| High | 0.43 (0.28–0.68) | <0.001 | 0.48 (0.31–0.75) | 0.001 | 0.58 (0.37–0.91) | 0.019 |
| <0.001 | <0.001 | 0.016 | ||||
| Per 0.1 mmol/L increase | 0.72 (0.61–0.85) | <0.001 | 0.76 (0.65–0.90) | 0.001 | 0.83 (0.70–0.98) | 0.028 |
| Variables | HR (95% CI) |
| |
|---|---|---|---|
| Age | 0.504 | ||
| <45 | 0.39 (0.11–1.38) | 0.144 | |
| 45–60 | 0.70 (0.49–1.01) | 0.058 | |
| ≥60 | 0.80 (0.67–0.97) | 0.022 | |
| Sex | 0.799 | ||
| Male | 0.75 (0.61–0.93) | 0.009 | |
| Female | 0.82 (0.63–1.06) | 0.127 | |
| Hypertension | 0.712 | ||
| No | 0.86 (0.58–1.27) | 0.453 | |
| Yes | 0.76 (0.64–0.92) | 0.004 | |
| Diabetes mellitus | 0.001 | ||
| No | 1.05 (0.82–1.34) | 0.705 | |
| Yes | 0.60 (0.48–0.75) | <0.001 | |
| CKD | 0.681 | ||
| No | 0.86 (0.69–1.07) | 0.169 | |
| Yes | 0.80 (0.61–1.05) | 0.105 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes, Cardiovascular Risks, and Lipoproteins · Lipoproteins and Cardiovascular Health · Cardiovascular Function and Risk Factors
Introduction
1
Cardiovascular disease remains the leading cause of death worldwide, with ischemic heart disease (IHD) representing the dominant contributor, accounting for 8.99 million deaths in 2021 (1). Among the modifiable risk factors, metabolic disturbances are major determinants of IHD, responsible for 46.21% of IHD-related deaths in 2021 (2). Over the past three decades, the global burden attributable to metabolic risk factors has increased by 1.6 to 3 times (3), highlighting their significance as key therapeutic targets in cardiovascular prevention.
Lipid-lowering therapy, particularly statin treatment, remains the cornerstone for reducing low-density lipoprotein cholesterol (LDL-C) and preventing major adverse cardiac and cerebrovascular events (MACCEs) (4, 5). However, despite the substantial benefits of LDL-C reduction, a considerable residual cardiovascular risk persists (6). This persistent risk has renewed attention on high-density lipoprotein cholesterol (HDL-C), traditionally regarded as “good cholesterol” owing to its potential protective effects against atherosclerosis (7).
Nevertheless, accumulating evidence has challenged this traditional paradigm. Several cohort studies have reported a U-shaped association between HDL-C and both all-cause and cardiovascular mortality among patients with IHD (8), while randomized controlled trials aimed at pharmacologically increasing HDL-C levels failed to show reductions in cardiovascular events (9). These inconsistencies suggest that HDL-C functionality, rather than total HDL-C concentration, may better reflect cardiovascular protection.
HDL particles are highly heterogeneous, comprising distinct subfractions that differ in density, diameter, and biological function (10, 11). Large, cholesterol-rich HDL-2 particles (HDL-2a, HDL-2b) primarily facilitate reverse cholesterol transport, whereas small, dense HDL-3 particles (HDL-3a, HDL-3b, and HDL-3c) exhibit potent antioxidative and anti-inflammatory effects (12, 13). Previous studies have demonstrated that small HDL particles are inversely associated with coronary disease severity and mortality among patients with IHD (14–16).
Acute myocardial infarction (AMI), a major clinical manifestation of IHD, continues to be associated with substantial risks of recurrent events and long-term mortality despite advances in reperfusion therapy and secondary prevention (17, 18). However, evidence directly linking HDL subfractions to long-term outcomes in AMI remains limited. Moreover, variability in HDL subfraction measurement techniques across studies may contribute to heterogeneous findings. Therefore, this study used microfluidic chip electrophoresis to precisely quantify HDL subfractions (HDL-2b and HDL-3) and to evaluate their association with long-term MACCE risk in patients with AMI.
Method
2
Study population
2.1
This retrospective observational study included patients diagnosed with AMI who were admitted to Beijing Tsinghua Changgung Hospital between September 2017 and June 2023. Both ST-elevation myocardial infarction and non-ST-elevation myocardial infarction were eligible for inclusion. Patients were excluded if they met any of the following criteria: (1) missing serum samples for HDL subfraction measurement; (2) missing blood cholesterol data; (3) presence of active infection, autoimmune disease, severe hepatic or renal insufficiency, or malignancy; and (4) incomplete follow-up information.
A total of 1,240 patients were included in the final analysis (Figure 1). The study protocol was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Tsinghua Changgung Hospital (Approval No. 23578-4-01). Given the retrospective design, the requirement for written informed consent was waived.
Flowchart of patient inclusion and exclusion criteria.
Measurement of HDL subfractions
2.2
Fasting venous blood samples were collected within 24 h of hospital admission. Serum was separated and stored at −80 °C until analysis. HDL subfractions were quantified using a microfluidic chip capillary electrophoresis system (MICEP-30, Ardent BioMed, Guangzhou, China) in accordance with the manufacturer’s instructions (19). Briefly, this technique separates HDL particles based on size and electrical charge, allowing quantification of HDL-2b and HDL-3 subfractions as percentages (%) of total HDL particles, from which corresponding concentrations were calculated. The intra-assay and inter-assay coefficients of variation were both <5%. Conventional lipid parameters, including total cholesterol (TC), LDL-C, and HDL-C, were measured using standard enzymatic methods in the central laboratory of Beijing Tsinghua Changgung Hospital.
Clinical data and definitions
2.3
Demographic characteristics, comorbidities, laboratory data, and coronary angiographic findings were extracted from the hospital’s electronic health record system. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or current use of antihypertensive drugs. Diabetes mellitus was defined as fasting glucose ≥7.0 mmol/L, HbA1c ≥ 6.5%, or current use of antidiabetic therapy. Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m^2^. Statin use was recorded if the patient was prescribed statin therapy at discharge. The severity of coronary artery stenosis was assessed using the Gensini score. Coronary angiograms were independently evaluated by two cardiologists who were blinded to patient outcomes, and discrepancies were resolved by consensus.
Outcomes and follow-up
2.4
The primary endpoint was the occurrence of MACCEs, defined as a composite of all-cause death, recurrent myocardial infarction (Re-MI), stroke, and major bleeding events (intracranial hemorrhage or gastrointestinal tract bleeding).
Follow-up information was obtained through outpatient visits, hospital records, and structured telephone interviews conducted every 6–12 months. The follow-up period was calculated from the date of the index AMI admission to the date of the first MACCE event or the last available contact.
Statistical analysis
2.5
Continuous variables were expressed as medians (Q1, Q3), and categorical variables were presented as counts (percentages). Differences among HDL subfraction tertile groups were compared using the Kruskal–Wallis test for continuous variables and the χ^2^ test for categorical variables.
Receiver operating characteristic (ROC) curve analysis was conducted to evaluate the discriminative ability of HDL-C, HDL-2b, and HDL-3 for predicting MACCEs. The area under the curve (AUC) and 95% confidence intervals (CIs) were calculated using DeLong’s non-parametric method, and AUCs were compared across HDL subfractions. Event-free survival was evaluated with Kaplan–Meier curves, and between-group differences were assessed with the log-rank test.
To examine the association between HDL subfractions and MACCEs, Cox proportional hazards regression models were constructed, and hazard ratios (HRs) with 95% CIs were estimated. HDL subfractions were analyzed both as tertiles and as continuous variables (per 0.1 mmol/L increment). Three hierarchical models were fitted, and the proportional hazards assumption was tested using Schoenfeld residuals and was satisfied for all models:
Model 1: unadjusted;Model 2: adjusted for age and sex;Model 3: further adjusted for hypertension, diabetes mellitus, CKD, and statin use. Restricted cubic spline (RCS) models with four knots were applied to evaluate potential non-linear relationships between HDL subfractions and MACCEs risk. To explore potential mechanisms, mediation analysis was performed to assess whether the Gensini score mediated the association between HDL-3 and MACCEs, using a bias-corrected bootstrap approach with 1,000 replications. Subgroup analyses were further conducted according to age, sex, hypertension, diabetes, and CKD status, and multiplicative interaction terms were included to test for effect modification.
All analyses were performed using R software (version 4.4.3), with two-tailed p < 0.05 considered statistically significant.
Results
3
Baseline characteristics
3.1
Among the 1,240 patients included in this study, the median age was 64 years, and 25.1% were women (Table 1). Patients were stratified into three groups according to HDL-3 tertiles for comparison. Individuals in the lowest HDL-3 tertile were significantly older (p = 0.001) and had a higher prevalence of CKD (p < 0.001). In contrast, the distributions of sex, hypertension, and diabetes mellitus were comparable across HDL-3 tertiles. In addition, patients with lower HDL-3 levels had substantially reduced eGFR values (p < 0.001) and elevated C-reactive protein levels (p < 0.001), suggesting more pronounced renal dysfunction and systemic inflammation.
Association between HDL subfractions and MACCEs risk
3.2
During a median follow-up of 52.4 months, 132 patients (10.7%) experienced MACCEs, including 42 deaths (3.4%) and 57 recurrent myocardial infarctions (4.6%) (Table 1).
The Kaplan–Meier analysis showed no significant differences in MACCEs risk across tertiles of total HDL-C or HDL-2b (log-rank p > 0.05; Figures 2A,B). In contrast, the cumulative incidence of MACCEs decreased progressively across increasing HDL-3 tertiles (log-rank p < 0.001; Figure 2C).
Kaplan–Meier survival curves for MACCEs by HDL subfraction tertiles. Kaplan–Meier survival curves showing the cumulative incidence of MACCEs across tertiles of (A) total HDL-C, (B) HDL-2b, and (C) HDL-3. Differences among tertile groups were evaluated using the log-rank test.
ROC analysis showed that HDL-C (AUC = 0.56; 95% CI: 0.50–0.61) and HDL-2b (AUC = 0.55; 95% CI: 0.49–0.60) showed limited discriminative ability for predicting MACCEs (Figure 3). In comparison, HDL-3 demonstrated stronger predictive performance (AUC = 0.62; 95% CI: 0.57–0.67).
ROC curves of HDL subfractions for predicting MACCEs. ROC curves illustrating the discriminative performance of total HDL-C, HDL-2b, and HDL-3 for predicting long-term MACCEs in patients with AMI.
In univariate Cox regression analysis, neither higher HDL-C nor HDL-2b levels were significantly associated with MACCEs risk compared with the lowest tertile (p > 0.05). In contrast, higher HDL-3 levels were associated with a lower MACCEs risk (Table 2). The HRs for MACCEs across HDL-3 tertiles were 0.56 (95% CI: 0.37–0.83) for the middle tertile and 0.43 (95% CI: 0.28–0.68) for the highest tertile. When analyzed as a continuous variable, each 0.1 mmol/L increment in HDL-3 was associated with a 28% reduction in MACCEs risk (HR = 0.72; 95% CI: 0.61–0.85).
The inverse association between HDL-3 and MACCEs remained significant after adjusting for potential confounding factors (Table 2). In the fully adjusted model (Model 3: adjusted for age, sex, hypertension, diabetes, CKD, and statin use), patients in the highest HDL-3 tertile had a significantly lower risk of MACCEs compared with those in the lowest tertile (HR = 0.58; 95% CI: 0.37–0.91). In the continuous model, each 0.1 mmol/L increase in HDL-3 was associated with a 17% reduction in the risk of MACCEs (HR = 0.83; 95% CI: 0.70–0.98).
Linear relationship between HDL-3 and MACCEs
3.3
RCS models adjusted for all covariates in Model 3 were used to evaluate the dose–response relationships between HDL subfractions and MACCEs risk. Neither HDL-C nor HDL-2b showed a significant association with MACCEs (p for overall > 0.05; Figures 4A, B). In contrast, HDL-3 demonstrated a linear inverse association with MACCEs (p for non-linearity = 0.356; Figure 4C).
RCS analyses for the association between HDL subfractions and MACCEs. RCS analyses illustrating the dose–response relationships between HDL subfractions and MACCEs risk. Models were adjusted for all covariates included in Model 3 (age, sex, hypertension, diabetes mellitus, chronic kidney disease, and statin use). Panels show (A) total HDL-C, (B) HDL-2b, and (C) HDL-3.
Mediation and subgroup analyses
3.4
Mediation analysis indicated that the Gensini score partially mediated the association between HDL-3 and MACCEs. Higher HDL-3 levels were inversely associated with the Gensini score, and this mediation pathway accounted for 11.8% of the overall protective effect of HDL-3 on MACCEs risk (Figure 5).
Mediation analysis of the association between HDL-3 and MACCEs. Mediation analysis evaluating the indirect effect of the Gensini score on the association between HDL-3 and MACCEs.
Subgroup analyses were performed to assess potential effect modification by demographic factors (age and sex) and comorbidities (hypertension, diabetes mellitus, and CKD). The inverse association between HDL-3 and MACCEs was consistent across age, sex, hypertension, and CKD subgroups (all p for interaction > 0.05). Notably, the protective association was stronger among patients with diabetes mellitus (p for interaction = 0.001; Table 3).
Cox proportional hazards models examining the association between HDL-3 levels and MACCEs across subgroups defined by age, sex, hypertension, diabetes mellitus, and CKD.
Discussion
4
In this single-center longitudinal cohort of patients with AMI, lower levels of the HDL-3 subfraction were significantly associated with a higher risk of long-term MACCEs, whereas total HDL-C and HDL-2b showed no independent predictive value. The inverse association between HDL-3 and MACCEs was linear and was partially mediated by the severity of coronary atherosclerosis, as quantified by the Gensini score. Notably, the protective effect of HDL-3 was most pronounced in patients with diabetes mellitus.
These results extend previous cross-sectional findings by demonstrating the long-term prognostic relevance of HDL subfractions in AMI patients. Earlier studies have reported that both HDL-2b and HDL-3 are inversely correlated with the severity of coronary stenosis, whereas total HDL-C did not display a consistent pattern (15, 20). Additional clinical studies across diverse cardiovascular populations also support the prognostic value of HDL-3. For instance, Kim et al. observed that HDL-3 exhibited a stronger protective association than HDL-2 in patients with carotid artery disease (21). Similarly, among individuals with heart failure, HDL-3, but not HDL-2 or total HDL-C, was significantly associated with reduced 3-month mortality (22). In two independent AMI cohorts (n = 2,465 and 2,414, respectively), HDL-3 was inversely associated with long-term adverse cardiac events (23). Furthermore, several studies focusing on HDL particle size have emphasized that smaller HDL particles provide better predictive power for mortality among patients with cardiovascular disease (24, 25).
HDL-3 represents the small, dense HDL particles enriched with functional proteins such as paraoxonase-1 and apolipoprotein A-I, which confer potent antioxidative and anti-inflammatory properties (26–28). Mechanistically, HDL-3, often described as small-sized HDL particles, can inhibit low-density lipoprotein oxidation, reduce endothelial adhesion molecule expression, and promote cholesterol efflux via ATP-binding cassette transporter A1 (ABCA1) (29–31). These biological effects limit macrophage foam-cell formation, suppress vascular inflammation within the arterial wall, and stabilize vulnerable plaques, thereby reducing the likelihood of recurrent ischemic events (32, 33). The mediation effect of the Gensini score observed in our study supports these classical anti-atherogenic pathways, suggesting that higher HDL-3 levels may help reduce atherosclerotic burden and promote coronary stability.
Nevertheless, mediation analysis showed that only 11.8% of the association between HDL-3 and clinical outcomes was explained by the Gensini score, implying that the majority of HDL-3’s protective effects are mediated through non-atherosclerotic pathways. Beyond plaque-related pathways, HDL-3 exerts systemic anti-inflammatory and antioxidative effects beyond the arterial plaque. By scavenging reactive oxygen species, modulating toll-like receptor signaling, and suppressing NLRP3 inflammasome activation, HDL-3 dampens post-infarction sterile inflammation and ventricular remodeling independent of plaque burden (34–37). In addition, HDL can improve endothelial function and microvascular perfusion via a sphingosine-1-phosphate-dependent pathway, further enhancing prognosis. More importantly, sphingosine-1-phosphate has been reported to be preferentially enriched in small, dense HDL3 particles (38, 39). Additionally, HDL-3 demonstrates antithrombotic and antiplatelet properties, reducing platelet aggregation and tissue-factor expression while enhancing endothelial prostacyclin and nitric oxide release, thereby decreasing the likelihood of thrombosis-driven recurrent events (40, 41). Collectively, these pleiotropic functions, including anti-inflammatory, vasodilatory, and antithrombotic effects, provide a biologically plausible explanation for the prognostic benefit of HDL-3 that is not mediated by coronary atherosclerosis.
A notable finding from this study is the significant interaction between HDL-3 and diabetes mellitus in determining the long-term prognosis of patients with AMI. Previous studies have reported associations between HDL subfractions and metabolic syndrome in individuals with premature coronary heart disease (42, 43). In diabetes, chronic hyperglycemia leads to oxidative modification and non-enzymatic glycation of HDL-associated proteins, including apolipoprotein A-I and paraoxonase-1, resulting in impaired cholesterol efflux capacity, reduced antioxidative activity, and a shift toward a pro-inflammatory HDL phenotype. Recent reviews further highlight that these compositional and enzymatic alterations contribute to the formation of dysfunctional HDL, characterized by reduced capacity to suppress vascular inflammation and preserve endothelial function (44). The stronger protective effect of HDL-3 observed in diabetic patients in our study may therefore reflect that, in a metabolically stressed environment, individuals with relatively preserved HDL-3 functionality derive the greatest cardiovascular benefit. In contrast, among non-diabetic individuals, who generally exhibit lower oxidative and inflammatory burden and experience fewer events, the functional gradient across HDL subfractions may be less pronounced, potentially explaining the absence of a significant association in this subgroup.
The findings of this study suggest that HDL subfractions, particularly the small, dense HDL-3 particles, may serve as practical and sensitive biomarkers for risk stratification in patients after AMI. Unlike total HDL-C, which represents a heterogeneous assemblage of HDL particles differing in size and function, HDL-3 directly reflects the most bioactive fraction with antioxidative and anti-inflammatory potential (33). Incorporating HDL-3 measurement into routine lipid profiling may help identify high-risk patients with elevated residual risk who could benefit from intensified lipid-lowering or anti-inflammatory therapies.
Several limitations of this study should be acknowledged. First, as an observational single-center cohort, causal relationships cannot be established, and unmeasured confounding factors may still exist despite multivariable adjustment. Second, HDL-3 was measured only at baseline, and longitudinal changes in HDL subfractions during follow-up were not assessed. Third, information on non-statin lipid-lowering therapies was not included because their prescription rates were extremely low, although a residual effect cannot be fully excluded. Finally, external validation in multicenter, prospective cohorts is needed to confirm the generalizability of these findings.
Conclusion
5
In this retrospective cohort of patients with AMI, lower HDL-3 subfraction levels were independently and linearly inversely associated with a higher long-term risk of MACCEs, whereas total HDL-C and HDL-2b did not demonstrate significant prognostic value. Part of the association between HDL-3 and cardiovascular outcomes was mediated by the severity of coronary atherosclerosis, as reflected by the Gensini score. These findings suggest that HDL-3 represents a functionally relevant component of HDL metabolism and may more accurately reflect residual cardiovascular risk than conventional lipid parameters.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Naghavi M Ong KL Aali A Ababneh HS Abate YH Abbafati C . Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2100–32. doi: 10.1016/S 0140-6736(24)00367-2, 38582094 PMC 11126520 · doi ↗ · pubmed ↗
- 2Wang Y Li Q Bi L Wang B Lv T Zhang P. Global trends in the burden of ischemic heart disease based on the global burden of disease study 2021: the role of metabolic risk factors. BMC Public Health. (2025) 25:310. doi: 10.1186/s 12889-025-21588-9, 39856644 PMC 11763131 · doi ↗ · pubmed ↗
- 3Zhang H Zhou X-D Shapiro MD Lip GYH Tilg H Valenti L . Global burden of metabolic diseases, 1990–2021. Metabolism. (2024) 160:155999. doi: 10.1016/j.metabol.2024.155999, 39151887 · doi ↗ · pubmed ↗
- 4Almeida SO Budoff M. Effect of statins on atherosclerotic plaque. Trends Cardiovasc Med. (2019) 29:451–5. doi: 10.1016/j.tcm.2019.01.001, 30642643 · doi ↗ · pubmed ↗
- 5KytöV Rautava P Tornio A. Initial statin dose after myocardial infarction and long-term cardiovascular outcomes. Eur Heart J Cardiovasc Pharmacother. (2023) 9:156–64. doi: 10.1093/ehjcvp/pvac 064, 36385668 PMC 9892868 · doi ↗ · pubmed ↗
- 6Hoogeveen RC Ballantyne CM. Residual cardiovascular risk at low LDL: remnants, lipoprotein(a), and inflammation. Clin Chem. (2021) 67:143–53. doi: 10.1093/clinchem/hvaa 252, 33257928 PMC 7793228 · doi ↗ · pubmed ↗
- 7Superko HR King S. Lipid management to reduce cardiovascular risk: a new strategy is required. Circulation. (2008) 117:560–8. doi: 10.1161/CIRCULATIONAHA.106.667428, 18227396 · doi ↗ · pubmed ↗
- 8Madsen CM Varbo A Nordestgaard BG. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: two prospective cohort studies. Eur Heart J. (2017) 38:2478–86. doi: 10.1093/eurheartj/ehx 163, 28419274 · doi ↗ · pubmed ↗