Adrenal Insufficiency due to Disseminated Cryptococcus in an Immunocompetent Individual
Jeremy A. Knott, Zoran Apostoloski

TL;DR
A rare case of adrenal insufficiency caused by Cryptococcus in an immunocompetent man is reported, emphasizing the need for early diagnosis and treatment.
Contribution
This case report highlights disseminated cryptococcosis as a rare cause of adrenal insufficiency in immunocompetent individuals.
Findings
Adrenal enlargement and insufficiency were caused by Cryptococcus neoformans in an immunocompetent patient.
FDG-PET imaging showed increased peripheral metabolic activity with central necrosis in the adrenal glands.
Treatment with antifungal therapy improved symptoms and confirmed the importance of early diagnosis.
Abstract
Primary adrenal insufficiency due to infiltrative fungal infections, such as Cryptococcus neoformans, is rare, particularly in immunocompetent patients. We present a case of an immunocompetent 61‐year‐old man who presented with bilateral adrenal enlargement and adrenal insufficiency, with a 3‐month history of generalised fatigue, weight loss and dizziness, as well as initial hyponatraemia and hyperkalaemia. Adrenal computed tomography (CT) revealed bilaterally enlarged adrenals, and fluorodeoxyglucose positron emission tomography (FDG‐PET) revealed increased peripheral metabolic surrounded by a photopenic core suggestive of central necrosis. Adrenal biopsies were consistent with Cryptococcus. Serum cryptococcal antigen (CrAg) testing was strongly positive (titres 1:1280) as was cerebrospinal fluid analysis (titre 1:160). The patient was commenced on hydrocortisone and fludrocortisone,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
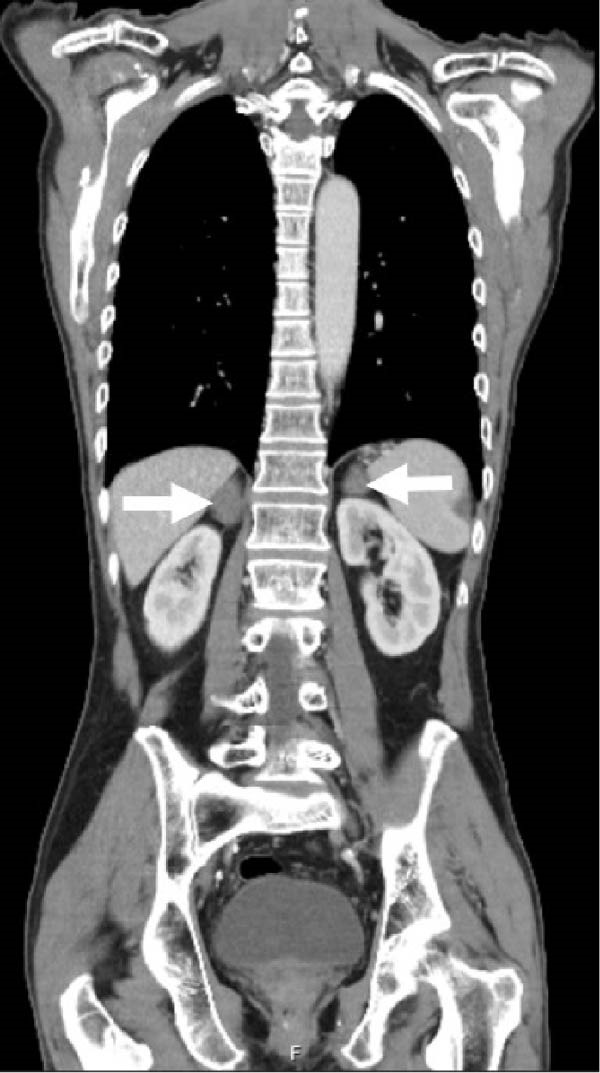 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Adrenal Hormones and Disorders
1. Introduction
Primary adrenal insufficiency is a potentially life‐threatening condition with the most common cause attributed to autoimmune adrenalitis in developed countries [1]. Differentiating the underlying cause of adrenal insufficiency can be challenging due to the nonspecific clinical presentation and broad range of aetiologies. Infiltrative fungal infections, such as Cryptococcus neoformans, causing adrenal insufficiency due to direct adrenal involvement are exceedingly rare, particularly in immunocompetent patients. This case outlines an immunocompetent 61‐year‐old man who presented with adrenal insufficiency and persistent bilateral adrenal enlargement due to disseminated Cryptococcus infection.
2. Case Report
A 61‐year‐old Caucasian male presented with a 3‐month history of generalised weakness, fatigue, weight loss and postural dizziness. There were no infective symptoms. He had no significant background medical history and was not on any medications. On physical examination, he appeared fatigued and was afebrile, hypotensive (blood pressure 92/73 mmHg) and had dry oral mucosa. His body mass index was 17 kg/m^2^.
Preliminary serology revealedhyponatraemia (Na 123 mmol/L; reference interval [RI],135–145 mmol/L), hyperkalaemia (K 5.5 mmol/L; RI, 3.5–5.2 mmol/L) and low morning cortisol (205 nmol/L; RI, 166–507 nmol/L), with elevated ACTH (216.2 ng/L; RI, 7.2–63.3 ng/L) confirming primary adrenal insufficiency. Initial abdominal computed tomography (CT) demonstrated bilateral adrenal enlargement of unclear cause (Figure 1). Steroid replacement with hydrocortisone (20 mg morning and 10 mg midday) and fludrocortisone (100 mcg daily) led to resolution of symptoms and biochemical correction.
An abdominal computed tomography (CT) scan revealed bilateral adrenal enlargement (arrows) of unclear cause on initial imaging.
Repeat imaging as an outpatient showed persistent adrenal enlargement of unclear cause. A further fluorodeoxyglucose positron emission tomography (FDG‐PET)/CT scan revealed increased FDG uptake (SUVmax 5.1 on the right, 3.3 on the left), with increased peripheral metabolic uptake surrounded by a relatively photopenic core region suggestive of central necrosis (Figure 2). Phaeochromocytoma was excluded prior to biopsy with normal plasma metanephrines (<50 pmol/L; RI <447 pmol/L), normetanephrines (152 pmol/L; RI <1010 pmol/L) and 3‐methoxytyramine (<25 pmol/L; RI <100 pmol/L). CT‐guided adrenal biopsies revealed Cryptococcus organisms (Figure 3), and Cryptococcus neoformans DNA was detected by PCR. Serum cryptococcal antigen (CrAg) testing was strongly positive (titres 1:1280) as was cerebrospinal fluid analysis (titre 1:160), indicating disseminated infection.
Figure 2A FDG‐PET scan revealed avidity in the right (SUVmax 5.1) and left (SUVmax 3.3) adrenal glands (arrows) with increased peripheral metabolic uptake surrounded by a relatively photopenic core region suggestive of central necrosis. (A) Coronal maximum‐intensity projection image. (B) Axial PET/CT fusion image.(A)(B)
Figure 3. Diagnostic adrenal biopsies revealed Cryptococcus organisms present on Grocott methenamine silver stain (A). The Cryptococcus polysaccharide capsule can be visualised on mucicarmine stain (B). Haematoxylin and eosin stain (C) revealed areas of diffusely necrotic tissue.(A)(B)(C)
The patient had normal absolute neutrophil (3.63 × 10^9^/L; RI, 1.7–7.0 × 10^9^/L) and total lymphocyte counts (2.52 × 10^9^/L; RI, 1.5–4.0 × 10^9^/L), with no evidence of chronic illness such as diabetes mellitus (HbA1c 5.4%; RI, 4%–6%) to suggest secondary immunosuppression. HIV antigen/antibody serology and an interferon‐gamma release assay for Mycobacterium tuberculosis were negative. Further immunological evaluation performed by the infectious diseases team demonstrated normal T‐cell subsets, including a preserved CD4^+^ count (0.93 × 10^9^/L; RI, 0.7–1.2 × 10^9^/L) and CD4/CD8 ratio (4.5), which was not suggestive of a primary T‐cell defect. Tests for anti‐granulocyte–macrophage colony‐stimulating factor antibodies and anti‐interferon gamma autoantibodies, which have been associated with increased susceptibility to cryptococcal infection, were negative.
Treatment involved induction therapy with intravenous liposomal amphotericin‐B 4 mg/kg daily and 5‐flucytosine 25 mg/kg four times daily for 2 weeks, followed by consolidation and maintenance therapy with fluconazole for 12–18 months. At the time of writing, the patient remains on maintenance hydrocortisone (20 mg morningand 10 mg midday) and fludrocortisone 100 mcg morning, with resolution of symptoms of their adrenal insufficiency.
3. Discussion
Disseminated Cryptococcus with adrenal involvement causing primary adrenal insufficiency is rare, particularly in immunocompetent individuals. Cryptococcus neoformans typically occurs in immunocompromised hosts as meningoencephalitis or lung disease [1]. In Australia, the leading cause of primary adrenal insufficiency is autoimmune adrenalitis, but infectious, infiltrative and metastatic causes may also be considered, particularly in the presence of bilateral adrenal enlargement [2].
The role of functional imaging in differentiating a potential infiltrative cause of adrenal insufficiency is not yet established. The destructive infiltrative process from Cryptococcus may reveal a distinct pattern on FDG‐PET/CT imaging with significant metabolic uptake along the adrenal peripheries with areas of central necrosis [3], as seen in our case. FDG‐PET/CT may also be useful to assess disease distribution and in guiding biopsy. This pattern may also help differentiate from malignancy or lymphoma, which often present with more homogeneous or diffuse uptake [3, 4].
Histopathology remains the gold standard for diagnosing adrenal cryptococcosis, but non‐invasive diagnostics play a pivotal role in raising clinical suspicion. CrAg testing is highly sensitive and specific, particularly in disseminated disease, and should be routinely considered in patients with bilateral adrenal enlargement and biochemical adrenal insufficiency of unclear cause [2, 5]. In our case, CrAg testing from serum was strongly positive (titre 1:1280), and earlier recognition for CrAg testing may expedite diagnosis, reduce reliance on invasive procedures and enable prompt initiation of antifungal therapy, potentially improving outcomes.
Despite antifungal clearance, recovery of adrenal function is often unlikely in infiltrative fungal infections due to irreversible destruction of adrenal tissue. In patients with bilateral adrenal disease, it is not always clear if antifungal cryptococcal therapy will result in recovery of adrenal function. In cases where primary adrenal insufficiency is secondary to a destructive disease process, adrenal recovery is unusual [5].
This case underscores the importance of considering fungal infections in the differential diagnosis of bilateral adrenal disease—even in immunocompetent patients. Functional imaging, tissue biopsy and targeted antigen testing are complementary tools that guide accurate and timely diagnosis. Early recognition and a suggested low threshold for CrAg testing, are critical to avoid delays in initiating antifungal therapy.
3.1. Learning Points
- 1.Bilateral adrenal enlargement in the context of primary adrenal insufficiency should prompt consideration of atypical infections such as Cryptococcus neoformans, even in immunocompetent patients.
- 2.Functional imaging (FDG‐PET/CT) may aid in distinguishing infiltrative infectious processes from malignancy and can help guide biopsy.
- 3.In cases of cryptococcal adrenalitis, adrenal function rarely recovers despite antifungal treatment, and long‐term steroid replacement is typically required.
Author Contributions
Jeremy A. Knott: writing – original draft. Zoran Apostoloski: patient diagnosis, treatment, management.
Funding
No funding was received for this manuscript.
Disclosure
Our case report was presented as a conference poster presentation at the Endocrine Society Australia in 2024, which can be viewed here: https://esa-srb-anzbms-2024.p.asnevents.com.au/days/2024-11-11/abstract/107311 [6].
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coussement J. , Heath C. H. , and Roberts M. B. , et al.Current Epidemiology and Clinical Features of Cryptococcus Infection in Patients Without Human Immunodeficiency Virus: A Multicenter Study in 46 Hospitals in Australia and New Zealand, Clinical Infectious Diseases. (2023) 77, no. 7, 976–986, 10.1093/cid/ciad 321.37235212 · doi ↗ · pubmed ↗
- 2Erichsen M. M. , Løvås K. , and Skinningsrud B. , et al.Clinical, Immunological, and Genetic Features of Autoimmune Primary Adrenal Insufficiency: Observations From a Norwegian Registry, The Journal of Clinical Endocrinology and Metabolism. (2009) 94, no. 12, 4882–4890, 10.1210/jc.2009-1368, 2-s 2.0-73249138400.19858318 · doi ↗ · pubmed ↗
- 3Jain T. K. , Karunanithi S. , Bal C. , and Kumar R. , 18F-FDG PET/CT Imaging in Adrenal Cryptococcosis, Clinical Nuclear Medicine. (2017) 42, no. 4, e 194–e 195, 10.1097/RLU.0000000000001214, 2-s 2.0-85010916114.28114222 · doi ↗ · pubmed ↗
- 4Baomo L. , Guofen Z. , Jie D. , Liu X. , Shuru C. , and Jing L. , Disseminated Cryptococcosis in a Patient With Idiopathic CD 4 + T Lymphocytopenia Presenting as Prostate and Adrenal Nodules: Diagnosis From Pathology and m NGS, a Case Report, BMC Infectious Diseases. (2024) 24, no. 1, 10.1186/s 12879-023-08926-1.PMC 1076344538166809 · doi ↗ · pubmed ↗
- 5Price C. E. , Burns C. , and Aloi J. A. , Primary Adrenal Insufficiency due to Cryptococcus With Persistent Adrenal Enlargement and Insufficiency, AACE Clinical Case Reports. (2023) 9, no. 6, 189–192, 10.1016/j.aace.2023.09.002.38045798 PMC 10690418 · doi ↗ · pubmed ↗
- 6Knott J. and Apostoloski Z. , Primary Adrenal Insufficiency due to Disseminated Cryptococcosis in an Immunocompetent Individual: Case Report, Poster Presentation ESA-SRB-ANZBMS 2024, 2024.