Hepatopleural Fistula Secondary to a Persistent Liver Abscess: A Case Report
Juan J Vergara Torrente, Maria Camila Velasquez, Santiago Velasquez, Angelica del Carmen Narvaez Morelo

TL;DR
A rare case of liver abscess leading to a fistula between the liver and pleural cavity is reported, highlighting the importance of timely surgical intervention.
Contribution
The paper presents a novel clinical case of hepatopleural fistula secondary to a persistent liver abscess and emphasizes the importance of surgical management.
Findings
A liver abscess progressed to hepatopleural fistula despite initial drainage.
Surgical intervention resolved the infection and closed the fistula successfully.
The case highlights the need for high clinical suspicion and timely management in similar cases.
Abstract
Hepatopleural fistula (HPF) is an abnormal communication between the pleural cavity and the hepatobiliary system; it is uncommon and carries relevant morbidity. Reported etiologies include thoracoabdominal trauma, liver abscess of different causes, biliary stenosis or obstruction, postsurgical iatrogenesis, and even congenital anomalies. We present the case of a 37-year-old woman with six months of right upper-quadrant pain and intermittent fever. Contrast-enhanced computed tomography (CT) showed a liver abscess; percutaneous drainage achieved initial improvement. One month later, she presented with exertional dyspnoea, productive cough, and fever. Studies demonstrated a loculated right pleural effusion and a persistent abscess, with imaging signs of hepatopleural communication suggestive of HPF. A pleural tube was placed with an initial 2,000 mL output, followed by posterolateral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
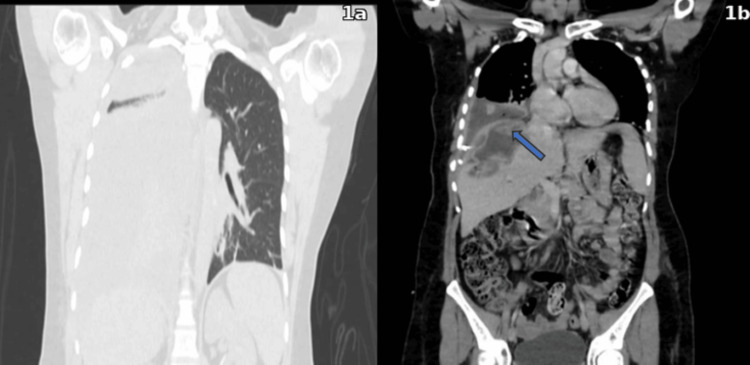 Figure 1
Figure 1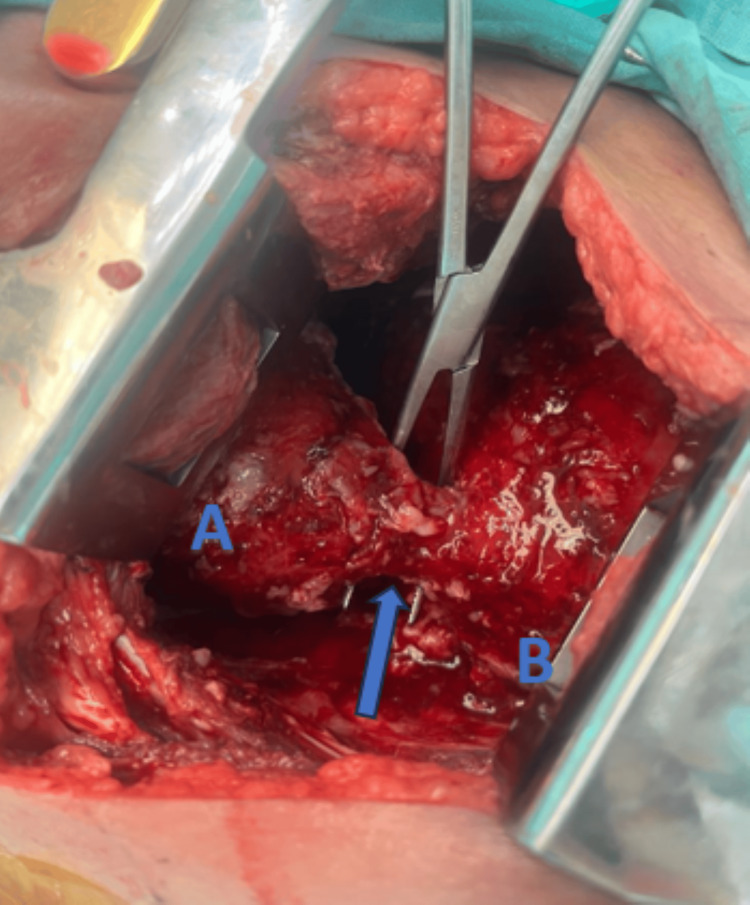 Figure 2
Figure 2| Serum Parameter | Measured Value | Reference Range |
| White blood cell | 19 300 k/µL | 4.0–11.0 k/µL |
| Neutrophils | 92.2 % | 37–80 % |
| C-reactive protein | 15 mg/dL | 0.0–1.0 mg/dL |
| Alanine aminotransferase | 48 U/L | 10–42 U/L |
| Aspartate aminotransferase | 49 U/L | 10–42 U/L |
| Total bilirubin | 2.2 mg/dL | 0.2–1.0 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Gallbladder and Bile Duct Disorders · Pleural and Pulmonary Diseases
Introduction
Hepatopleural fistula (HPF) is a rare entity defined by a communication between the pleura and the hepatobiliary system, traditionally reported as a complication of infectious hepatic processes, trauma, and biliary tract obstruction [1,2,3-5]. Recognition may be delayed due to clinical overlap with other causes of pleural effusion and is associated with adverse outcomes if the infectious focus persists [1,3,4].
HPF typically develops when a persistent liver abscess or elevated biliary pressure erodes the diaphragm, establishing a tract from the hepatic parenchyma/biliary tree into the pleural space, a process facilitated by the thoracoabdominal pressure gradient and local inflammation. Clinical features include bilothorax, pleural effusion most often on the right side, and cough with bilious sputum when a bronchobiliary communication is present. Nevertheless, HPF remains underrecognized and often mimics common pleural or pulmonary conditions, which frequently delays diagnosis.
Series and case reports describe different therapeutic strategies: percutaneous drainage of the liver abscess, pleural drainage with thoracentesis, video-assisted thoracoscopic surgery (VATS) or thoracotomy with decortication, and, when biliary obstruction exists, endoscopic decompression via endoscopic retrograde cholangiopancreatography (ERCP) [4-6]. We report HPF secondary to a persistent liver abscess after percutaneous drainage that required open surgical management with good outcomes.
Case presentation
A 37-year-old woman, with no relevant medical history, presented with right upper quadrant abdominal pain for six months without clear triggers and intermittent subjective fever. She was initially evaluated by her family physician, who ordered blood tests and an upper abdominal ultrasound. Laboratory tests showed no acute phase reactants and no abnormalities in liver function tests or bilirubin levels. Ultrasound revealed an oval lesion in segment VIII with a well-defined wall, measuring approximately 500 mL, suggestive of a hepatic abscess. Given clinical stability, ultrasound-guided percutaneous drainage was performed, yielding 300 mL of purulent material, and culture-directed antibiotic therapy was initiated. Over the following days, drainage remained around 50 mL per day; in the absence of symptoms and with decreased purulence, the catheter was removed.
One month later, she experienced a recurrence of symptoms characterized by abdominal pain, progressively worsening exertional dyspnea, productive cough, and fever, suggesting persistence or complication of the underlying infection. On physical examination, lung auscultation revealed coarse crackles at the right lung base. The abdomen was soft, with mild deep tenderness to palpation in the right upper quadrant, without peritoneal signs. Admission laboratory studies demonstrated leukocytosis with neutrophil predominance, elevated C-reactive protein, abnormalities in liver function tests, and hyperbilirubinemia (Table 1). Chest radiography showed a right pleural effusion. Contrast-enhanced thoracoabdominal computed tomography (CT) confirmed a loculated right pleural effusion occupying approximately 50% of the hemithorax (Figure 1a), a hepatic abscess in segments VII and VIII, and imaging findings suggestive of a hepatodiaphragmatic communication consistent with an HPF (Figure 1b).
Contrast-enhanced chest CT1a. Coronal section showing a right pleural effusion; 1b. Coronal section demonstrating a communication between the diaphragm and the right hepatic lobe, suggestive of a hepatopleural fistula (blue arrow).
A right pleural drainage tube was placed, with 2,000 mL of purulent fluid drained in the first 24 hours. Based on the anatomical characteristics, pleural thickening, and our team’s experience, a right posterolateral thoracotomy with decortication was selected as the surgical approach, along with fistula closure and placement of two pleural drains.
Intraoperatively, pleural thickening of at least 1 cm with fibrinopurulent empyema and a fistulous tract extending from the right diaphragmatic dome to the ipsilateral lower lobe were observed (Figure 2). The culture of the drained fluid grew Escherichia coli; targeted antibiotic therapy with piperacillin-tazobactam was initiated. The percutaneous abdominal drain was reinserted (output 100 mL/day), and the pleural drain was maintained (400 mL/day), both showing a progressive decline. After a joint evaluation with the hepatobiliary and thoracic surgery services, the pleural and abdominal drains were removed on postoperative day seven. The patient was discharged in good condition with follow-up; abdominal CT showed no evidence of hepatopleural fistula or pleural effusion and no hepatic abscess.
Intraoperative findingsThe blue arrow indicates the fistulous tract; A denotes the lower lung lobe; B denotes the diaphragmatic dome.
Discussion
HPF is an abnormal communication between the biliary tree or hepatic parenchyma and the pleural space. It usually arises in the setting of persistent hepatic infection, especially pyogenic abscesses, with *Klebsiella *as a frequent pathogen, as well as after diaphragmatic or hepatic injury due to trauma or surgical interventions. It may also be associated with biliary tract obstruction and, less commonly, with tumorous infiltration (e.g., hepatocellular carcinoma) or congenital anomalies; advanced liver disease, such as portal hypertension and cirrhosis, can coexist [7]. Physiopathologically, the thoracoabdominal pressure gradient and local inflammation promote fistulous-tract formation, resulting in biliothorax or right-sided empyema [2, 8, 9].
Management should prioritize source control: pleural and abscess drainage with culture-directed antibiotics. Where biliary obstruction or intraductal hypertension is present, endoscopic decompression via ERCP may hasten clinical resolution. In the setting of loculated effusions, pleural fibrosis, or failure of conservative measures, thoracic intervention, either VATS or open thoracotomy, allows decortication and fistula closure with high success rates; the choice depends on team experience and anatomical complexity. Timely source control and technical expertise are pivotal to outcomes [2,4-6,10]. This case illustrates HPF secondary to a persistent liver abscess with progression to empyema and the need for definitive surgical intervention despite initial percutaneous drainage.
We adopted a staged, mixed approach: an initial open thoracic procedure for empyema control, decortication, and fistula closure, followed by a second percutaneous abdominal intervention for complementary hepatic drainage, plus targeted antibiotics. Indications were based on the persistent hepatic focus and refractory loculated effusion limiting pulmonary re-expansion and perpetuating local sepsis. Early intervention enabled effective source control, progressive decline in outputs, timely drain removal, and an uncomplicated discharge, consistent with contemporary recommendations for complicated HPF.
The literature indicates that HPF commonly arises from persistent or unresolved liver abscesses and that, in the setting of loculated pleural collections, pleural fibrosis, or failure of initial percutaneous drainage, thoracic interventions (VATS or open thoracotomy with decortication) and direct closure of the fistulous tract, combined with drainage of the hepatic source and culture-directed antibiotics, are associated with improved outcomes; furthermore, when biliary hypertension or obstruction is present, endoscopic decompression can expedite recovery. In our case, clinical relapse after percutaneous drainage, a loculated right empyema, and the absence of biliary obstruction prompted a staged approach consisting of decortication and fistula closure plus complementary hepatic drainage and targeted antimicrobial therapy, yielding a favorable course consistent with these recommendations.
Conclusions
HPF is an infrequent complication of liver abscess with potential progression to empyema. Timely diagnosis requires a high index of suspicion and imaging correlation. Treatment selection should be individualized according to the predominant pathophysiology, raised biliary pressure versus a direct hepatopleural communication, ranging from biliary decompression to decortication and fistula closure, where a loculated effusion and a persistent infectious focus predominate. A multidisciplinary and early approach is associated with better outcomes. In addition, microbiological confirmation and targeted antibiotic therapy optimize infection control, while postoperative clinical and imaging surveillance allow early detection and treatment of recurrences or residual collections. This case supports a stepwise algorithm (drainage, source control, and, where necessary, surgical intervention). Although a single report, the findings align with available evidence and support early evaluation by thoracic and hepatobiliary teams to reduce morbidity and accelerate recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hepatopulmonary fistula: a rare complication of liver abscess. Description of a case Respirar Arévalo C Rodríguez J Bustillo C Remolina C 492018 https://alatorax.org/pt/publicacoes/respirar/22/36/download/36_file_es_Gis 2E 2_respirar-alat-vol 10num 1jun 2018-web-4-9.pdf
- 2A CARE-compliant article: a case report of pleural empyema secondary to Klebsiella pneumoniae liver abscess with a hepatopleural fistula Medicine (Baltimore) Lee EJ Lee KH Kim JH Jeon YS Kim JS 099202010.1097/MD.0000000000019869 PMC 722018532312012 · doi ↗ · pubmed ↗
- 3Bronchobiliary fistulas in adults Ann Surg Gugenheim J Ciardullo M Traynor O Bismuth H 90942071988333756710.1097/00000658-198801000-00017 PMC 1493242 · doi ↗ · pubmed ↗
- 4Management of acquired bronchobiliary fistula: 3 case reports and a literature review J Cardiothorac Surg Eryigit H Oztas S Urek S Olgac G Kurutepe M Kutlu CA 52220071805319210.1186/1749-8090-2-52PMC 2217537 · doi ↗ · pubmed ↗
- 5Surgical management of hydatid bilio-bronchial fistula by exclusive thoracotomy Int J Surg Rabiou S Lakranbi M Ouadnouni Y Panaro F Smahi M 1121184120172836362410.1016/j.ijsu.2017.03.074 · doi ↗ · pubmed ↗
- 6Hydatid hepatopleural fistula causing biliothorax: minimally invasive approach with ERCP stent placement and chest tube drainage: a case report Ann Med Surg (Lond) Mainali S Sapkota P Koirala P K CN Bhandari M Neupane PK 626662738520233809853710.1097/MS 9.0000000000001438 PMC 10718347 · doi ↗ · pubmed ↗
- 7Pleural interventions in the management of hepatic hydrothorax Chest Gilbert CR Shojaee S Maldonado F 27628316120223439070810.1016/j.chest.2021.08.043 · doi ↗ · pubmed ↗
- 8Thoracobiliary fistula complications following concomitant diaphragm and liver injury J Surg Res Kim NY Sadowsky MG Woodyard De Brito KC Williams C Janowak CF 16317030520253970089210.1016/j.jss.2024.11.009 · doi ↗ · pubmed ↗