An Unusual Case of Intrapulmonary Placement of a Thoracic Drain
Akram Assadiki, Hamraoui Salima, Doaae El Ouaddane, Ahdadi Ahmed, Rachid Marouf

TL;DR
A man with COPD suffered lung injury from a misplaced chest tube, requiring surgery and emphasizing the need for proper technique and imaging.
Contribution
A case report highlighting rare but serious lung injury from chest tube insertion and the importance of proper technique and imaging.
Findings
A chest tube traversed lung tissue in a COPD patient, causing persistent pneumothorax and subcutaneous emphysema.
Surgical intervention, including mini thoracotomy and lung resection, was necessary for recovery.
The case underscores the need for accurate imaging and proper technique to prevent iatrogenic lung injury.
Abstract
Chest tube insertion for pneumothorax and other pleural diseases is a common and relatively minor procedure but carries risks such as iatrogenic lung injury, particularly in patients with preexisting lung disease or pleural adhesions. We present a case of lung injury following chest tube insertion in a Moroccan man with chronic obstructive pulmonary disease (COPD) and emphysematous lung disease. The chest tube traversed lung tissue, causing a persistent pneumothorax and subcutaneous emphysema. Surgical intervention, including mini thoracotomy, adhesiolysis, and lung resection, was required. The patient recovered satisfactorily. This report highlights the importance of correct technique, imaging for accurate tube placement, and timely surgical intervention in complicated cases. Although rare, lung injury caused by chest tube insertion is serious and warrants careful attention from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
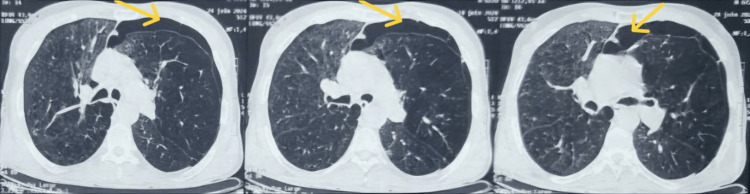 Figure 1
Figure 1 Figure 2
Figure 2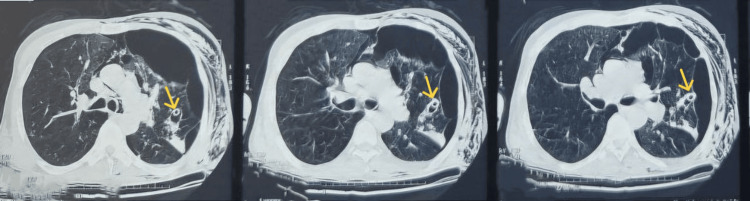 Figure 3
Figure 3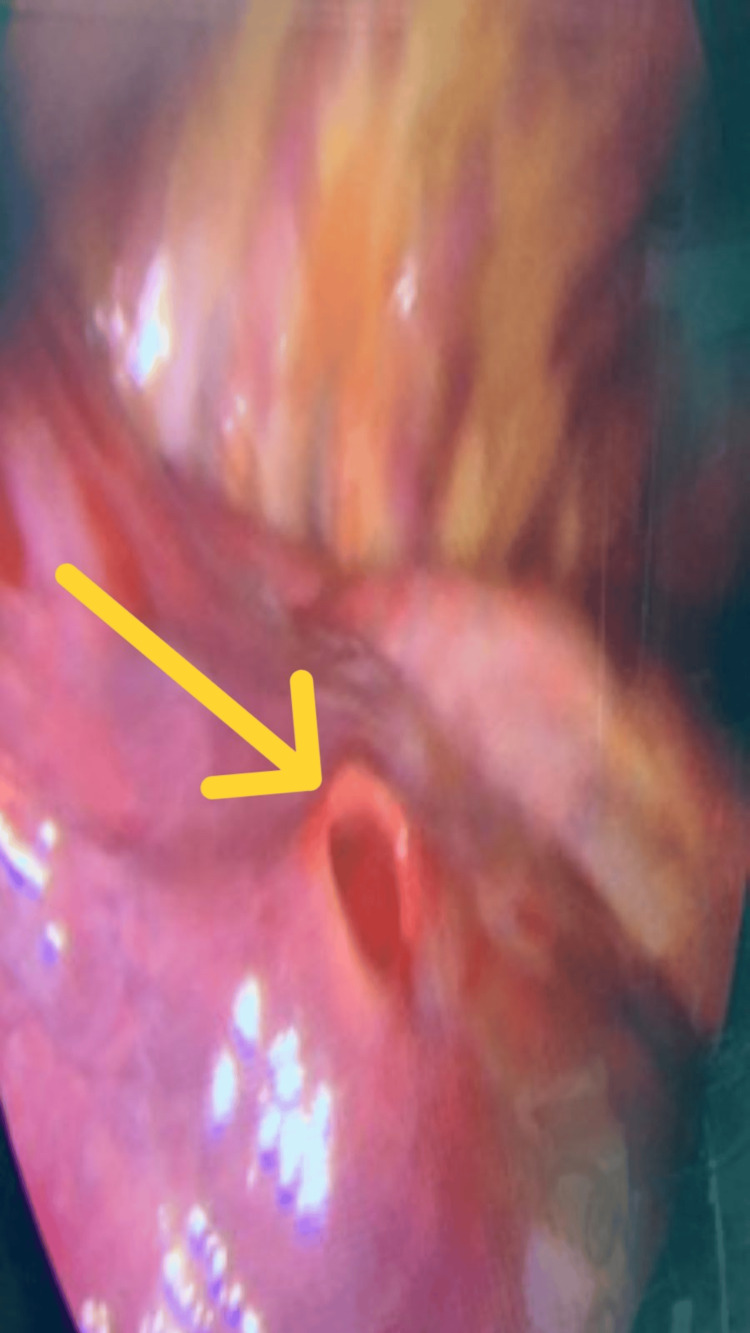 Figure 4
Figure 4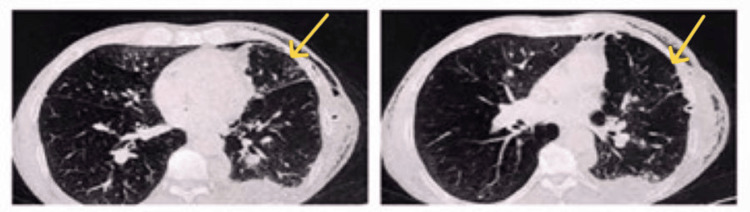 Figure 5
Figure 5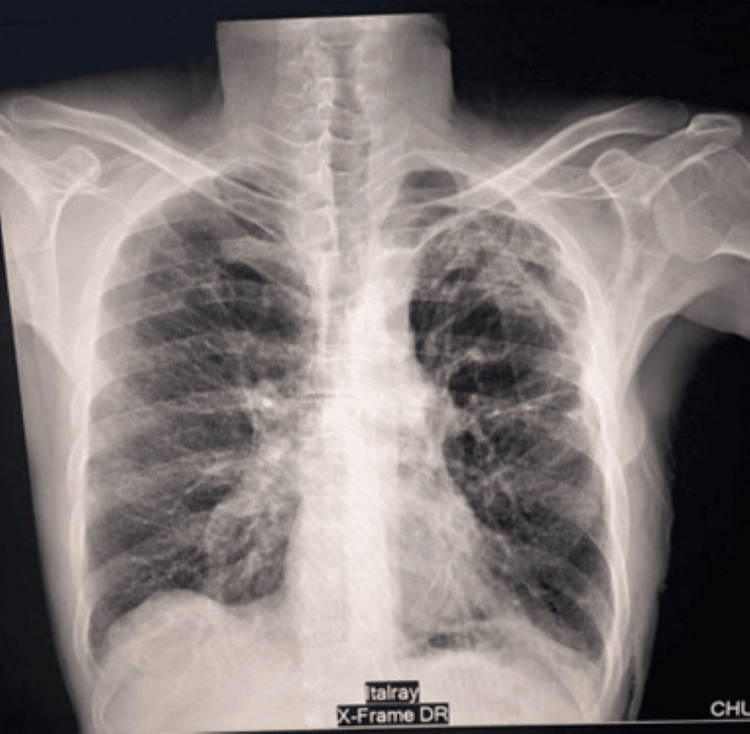 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Congenital Diaphragmatic Hernia Studies · Pneumothorax, Barotrauma, Emphysema
Introduction
The placement of a chest tube is a common technique adopted in the management of hemothorax, empyema, and pneumothorax. Even though technically simple, chest tube placement has a significant risk of complications, of which iatrogenic lung injury has been reported in approximately 3% of patient cases [1]. Such a situation is more probable when pleural adhesions and underlying lung disease are involved [2]. This intraparenchymal injury may lead to a bronchopleural fistula, a rare but documented complication [3]. These complications most typically occur during inexperienced physician procedures, although even skilled practitioners are vulnerable, and management ranges from conservative measures to surgical intervention, including anatomical lung resection [4].
Case presentation
A 56-year-old Moroccan man, a chronic smoker with a history of chronic obstructive pulmonary disease (COPD) and emphysematous lungs, presented with shortness of breath and chest pain. He was diagnosed with a left-sided secondary pneumothorax. On admission, his vital signs were stable: heart rate of 80 beats per minute (bpm), blood pressure of 120/71 mmHg, and oxygen saturation of 93% while receiving 8 L/minute of oxygen. He showed signs of respiratory distress with paradoxical thoracoabdominal movement, and clinical examination revealed a left-sided air effusion syndrome. A chest X-ray, followed by computed tomography (CT), confirmed the left pneumothorax (Figure 1).
Computed tomography before chest tube insertionThe admission chest computed tomography scan revealed an anterior left-sided pneumothorax (indicated by yellow arrows)
The patient was admitted to pulmonology, and a 24 Fr Jolly (Vygon, Swindon, United Kingdom) chest tube was placed in the fourth intercostal space. A follow-up chest X-ray showed persistent pneumothorax with extensive subcutaneous emphysema (Figure 2), and air leaks continued.
Chest X-ray taken one hour after chest tube insertionThe chest X-ray shows a persistent pneumothorax associated with significant subcutaneous emphysema
A computed tomography performed the next day revealed the chest tube tip lodged within the upper lobe of the left lung, creating a parenchymal-pleural fistula and worsening subcutaneous emphysema (Figure 3).
Computed tomography performed a day after chest tube insertionThe scan shows the chest tube positioned in the left upper lobe (indicated by yellow arrows), with lung collapse appearing more severe than prior to the insertion
As drainage was ineffective in controlling the air leak, the patient was transferred to thoracic surgery.
The following day, video-assisted thoracoscopic surgery (VATS) was performed via the fifth intercostal space, with an additional 2 cm camera port in the seventh intercostal space. Thoracoscopic exploration (Figure 4) identified the intrapulmonary drain tract, with entry at the drainage port site and exit at the apex. Adhesions between the chest wall and left upper lobe were dissected using Harmonic scissors (Ethicon, Raritan, NJ). Apical lung resection was completed with four Echelon (Ethicon, Raritan, NJ) stapler cartridges, and an additional parenchymal resection was performed at the inlet port with two cartridges. Hemostasis was secured; two chest tubes, one apical and one basal, were placed, and the wound was closed in layers.
Intraoperative imageThe wound tract was readily identified through thoracoscopic exploration (indicated by the yellow arrow)
Postoperatively, no further air leakage was observed, and the lung expanded fully. The recovery was uneventful. The patient was discharged in good condition following chest tube removal, with satisfactory control computed tomography imaging (Figure 5) and a proper follow-up chest X-ray (Figure 6).
A follow-up thoracic computed tomographyFollow-up chest computed tomography obtained on postoperative day 5 shows the appropriate re-expansion of the lung, with the left lung adequately opposed to the thoracic wall (yellow arrows)
The discharge chest X-rayThe patient's discharge chest X-ray was satisfactory
Discussion
Chest tube thoracostomy remains a vital intervention in critically injured patients, as it allows for the evaluation of intrathoracic bleeding, facilitates the evacuation of pleural blood, prevents the development of tension pneumothorax, and promotes lung re-expansion; in addition, it contributes to the stabilization of low-pressure pulmonary vessels and enhances overall respiratory function [5]. Reported complications include insertional (7.9%), positional (11.8%), and infectious (2.6%), with overall complication rates ranging from 1.2% to 15% [6,7]. Although complications are more frequent among trainees, they may occasionally occur even with experienced specialists.
The most frequent complications are bleeding from intercostal vessel injury, lung parenchymal damage, and persistent air leaks. Rare but serious events have also been described, including accidental placement of the tube into the diaphragm or the phrenic nerve [8]. In exceptional cases, injuries to major structures such as the aorta, pulmonary arteries, cardiac chambers, or even the stomach and abdominal cavity through the diaphragm have been reported [9].
Multiple factors contribute to technical difficulties, particularly when chest tubes are inserted by junior physicians without close supervision. The site of entry plays a critical role: the safest location is usually the fifth intercostal space in the midaxillary line, where the intercostal space is widest and away from vital structures. Positioning the patient semi-recumbent or upright improves landmark identification and reduces the risk of misplacement into breast tissue. Although trocar tubes allow easier insertion, they must be carefully controlled to avoid injury, especially in patients with adhesions.
The blind insertion of a chest tube in cases of loculated empyema or areas with pleural adhesions should be avoided, as it often leads to ineffective drainage and increased risk of complications. Furthermore, the misdiagnosis of conditions such as bullae, lung abscesses, or diaphragmatic eventration carries the risk of improper chest tube placement, including possible insertion into the abdominal cavity [10].
Lung perforation remains a recognized complication, though uncommon in adults due to blunt dissection. Such injuries are more likely in patients with reduced lung compliance or dense pleural adhesions and may evolve into persistent parenchymal-pleural fistulas. Clinically, a malpositioned intrapulmonary tube often presents with subcutaneous emphysema and crepitus from persistent air leaks, though some patients may remain asymptomatic and without radiographic evidence. Ideally, tubes for pneumothorax should be placed anteriorly and superiorly. On chest radiographs, they typically follow a smooth curvilinear path into the rib cage, convex laterally if posterior and medially if anterior. CT imaging offers the most accurate assessment, often revealing intraparenchymal tube placement, associated hematoma, residual pneumothorax, and subcutaneous emphysema. Surgical repair is rarely necessary, except in cases of uncontrolled air leaks or major hemorrhage.
Conclusions
Chest tube-related lung parenchymal injury is rare, with limited guidance available for its management. While many cases resolve with conservative treatment, patients with preexisting lung disease may require surgery. This case highlights the successful surgical management of an inadvertent intrapulmonary chest tube placement and underlines the need for thoracic surgeons to be prepared for such uncommon but serious complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chest tube complications: how well are we training our residents?Can J Surg Ball CG Lord J Laupland KB 450458502007 https://pubmed.ncbi.nlm.nih.gov/18053373/18053373 PMC 2386217 · pubmed ↗
- 2Errors and complications in chest tube placement Thorac Surg Clin Filosso PL Guerrera F Sandri A Roffinella M Solidoro P Ruffini E Oliaro A 5767272017 https://doi.org/10.1016/j.thorsurg.2016.08.009.2786532810.1016/j.thorsurg.2016.08.009 · doi ↗ · pubmed ↗
- 3Air leaks, pneumothorax, and chest drains Cont Educ Anaesth Crit Care Pain Paramasivam E Bodenham A 20420982008 https://doi.org/10.1093/bjaceaccp/mkn 038
- 4Chest tube injury to left ventricle: complication or negligence?Ann Thorac Surg Haron H Rashid NA Dimon MZ Azmi MH Sumin JO Zabir AF Abdul Rahman MR 308309902010 https://doi.org/10.1016/j.athoracsur.2010.01.0752060981010.1016/j.athoracsur.2010.01.075 · doi ↗ · pubmed ↗
- 5The risk of percutaneous chest tube thoracostomy for blunt thoracic trauma Ann Emerg Med Daly RC Mucha P Pairolero PC Farnell MB 865870141985402598410.1016/s 0196-0644(85)80635-1 · doi ↗ · pubmed ↗
- 6Wrong-side/wrong-site, wrong-procedure, and wrong-patient adverse events: are they preventable?Arch Surg Seiden SC Barach P 9319391412006 https://doi.org/10.1001/archsurg.141.9.931.1698303710.1001/archsurg.141.9.931 · doi ↗ · pubmed ↗
- 7Complications of tube thoracostomy in trauma J Accid Emerg Med Bailey RC 111114172000 https://doi.org/10.1136/emj.17.2.111.1071823210.1136/emj.17.2.111PMC 1725338 · doi ↗ · pubmed ↗
- 8Acute diaphragmatic paralysis caused by chest-tube trauma to phrenic nerve Pediatr Radiol Nahum E Ben-Ari J Schonfeld T Horev G 444446312001 https://doi.org/10.1007/s 002470100428.1143689310.1007/s 002470100428 · doi ↗ · pubmed ↗