When a Large Left Hemisphere Stroke is All Right for Language, Praxis, and Visual Attention: A Case Report
Elizabeth H.T. Chang, Peter E. Turkeltaub, Anna Seydell-Greenwald

TL;DR
A rare case shows that language, praxis, and visual attention can remain intact after a large left hemisphere stroke due to right hemisphere dominance.
Contribution
This case report presents a rare example of 'crossed non-aphasia' with simultaneous right-hemisphere lateralization of multiple functions.
Findings
The patient had intact language and praxis despite a large left hemisphere stroke.
fMRI showed right-hemisphere dominance for language and preserved visuospatial cognition.
The case supports the possibility of independent lateralization of multiple brain functions.
Abstract
To describe a rare case of large left hemisphere (LH) middle cerebral artery (MCA) stroke with intact language, praxis, visuospatial cognition, and attention, suggesting lateralization of all these functions to the intact right hemisphere (RH). A 53-year-old right-handed woman who had a stroke at age 42 was enrolled in a study of long-term stroke outcomes. She underwent standardized behavioral assessments and functional MRI (fMRI) with a visual field test and an adaptive semantic matching task. Despite a 432 cm3 area of encephalomalacia, encompassing both MCA and posterior anterior cerebral artery territories of the LH, she exhibited intact language both acutely and chronically (Western Aphasia Battery Aphasia Quotient = 99.2) and normal praxis. fMRI demonstrated right-hemisphere dominance for language. Visuospatial cognition and attention were preserved (WASI II-Block Design;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
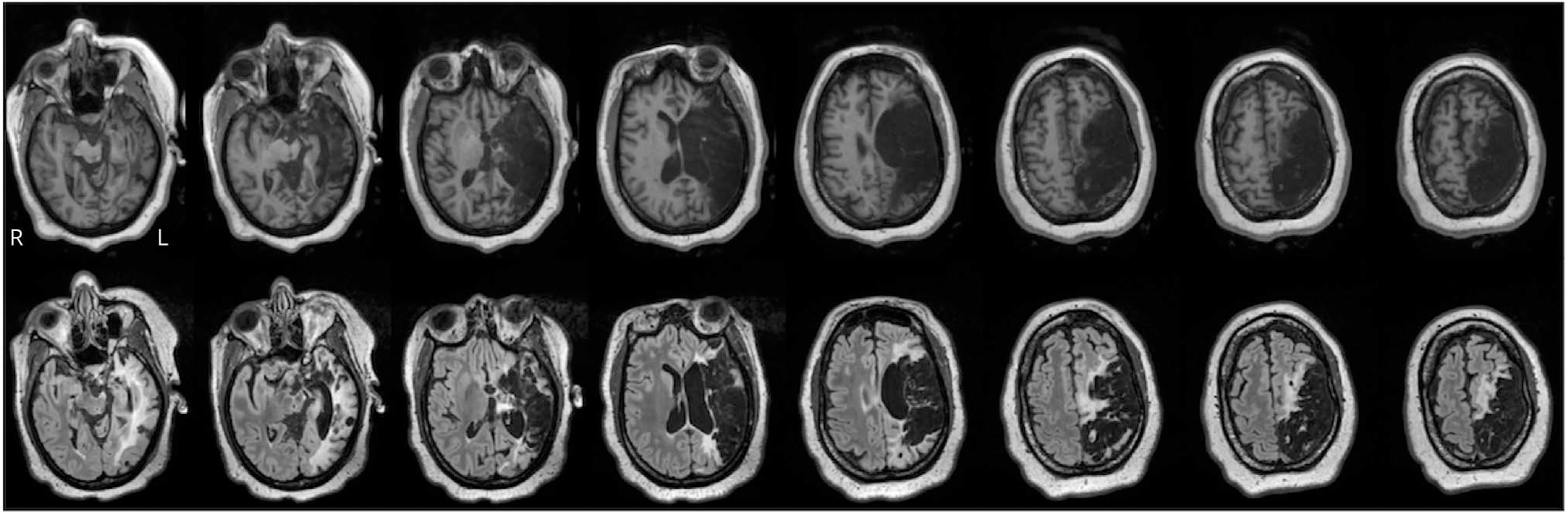 Figure 1
Figure 1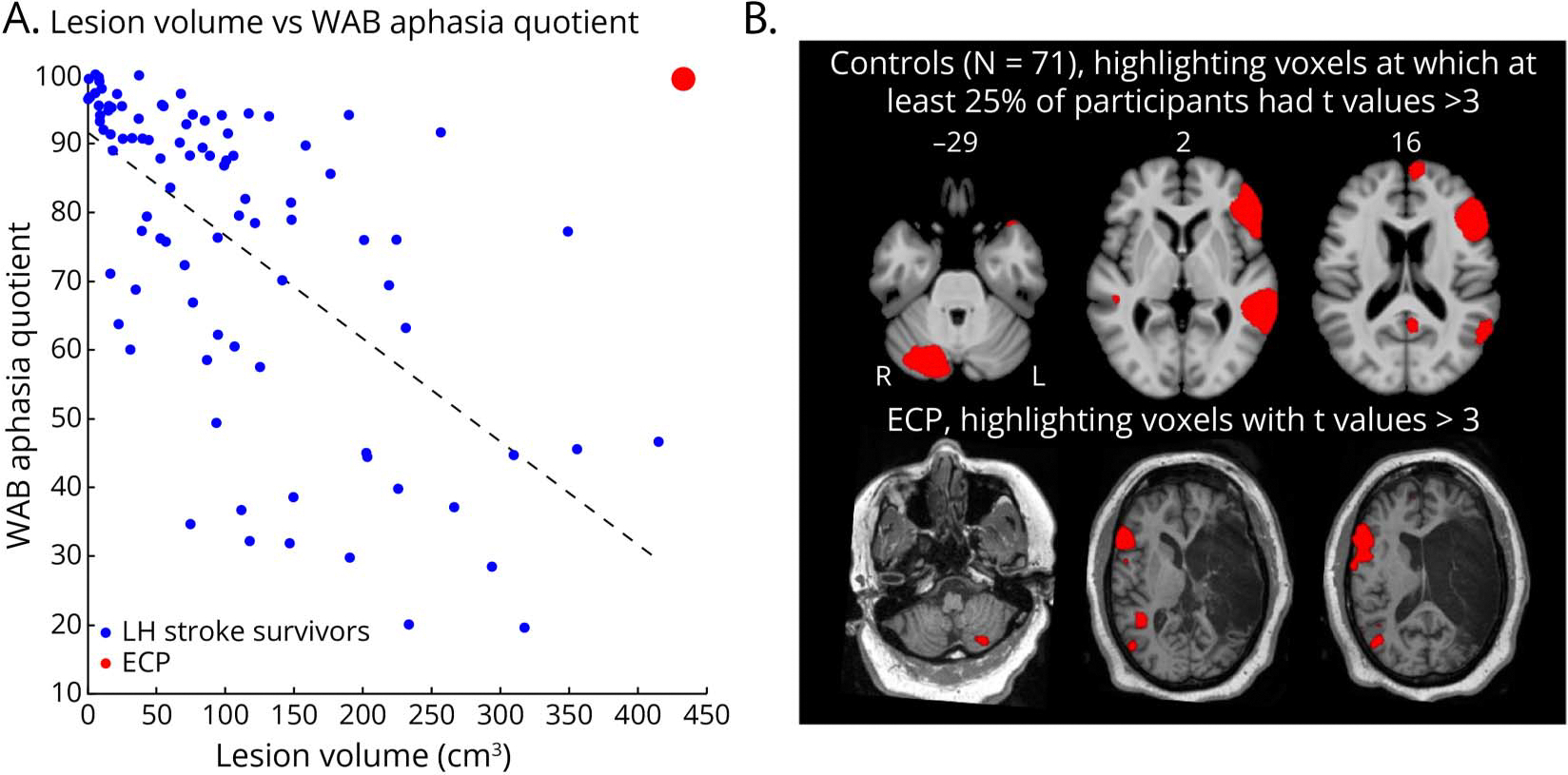 Figure 2
Figure 2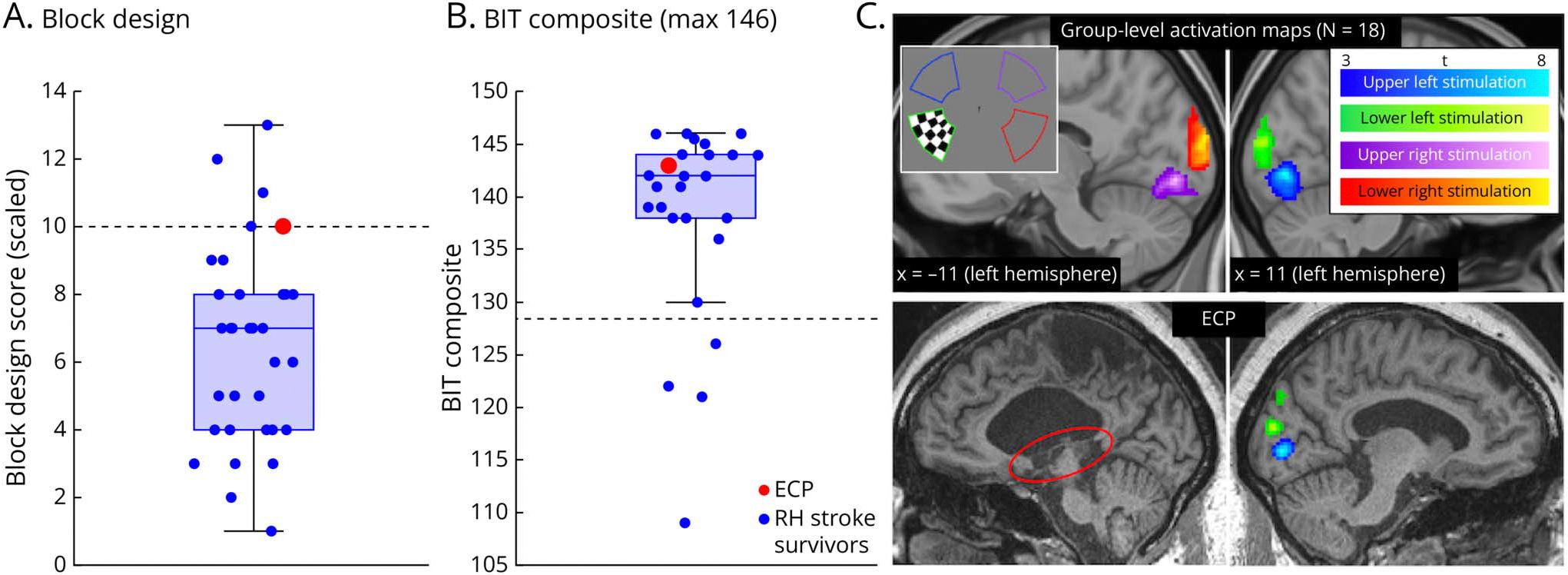 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpatial Neglect and Hemispheric Dysfunction · Neurobiology of Language and Bilingualism · Hemispheric Asymmetry in Neuroscience
Introduction
Left hemisphere (LH) strokes commonly result in language impairments, while right hemisphere (RH) strokes are associated with visuospatial and attentional deficits. Here, we present a case of a woman who had a large LH middle cerebral artery (MCA) ischemic stroke at age 42 and exhibits neither aphasia nor the typical cognitive sequelae of RH stroke. This case highlights a rare instance of simultaneous RH dominance for major cognitive functions typically lateralized to opposite hemispheres.
Methods
Experimental Design
The patient enrolled in two IRB-approved observational studies of chronic stroke outcomes at Georgetown University. Clinical history, including acute presentation, imaging, and past medical history, was obtained through electronic medical records. Standardized behavioral assessments were conducted at 61- and 86-month poststroke. The test battery included Montreal Cognitive Assessment (MoCA), Western Aphasia Battery (WAB), Apraxia Battery for adults, Wechsler Abbreviated Scale of Intelligence-II (WASI-II), Behavioral Inattention Test-conventional subtests (BIT-c), and oral real and pseudoword reading and spelling tasks. Language outcomes were compared with those of 95 LH stroke survivors. Reading and spelling performance was compared with those of 17 education-matched healthy controls. Visuospatial outcomes were compared with those of 32 RH stroke survivors. Demographic information on all three cohorts is summarized in eTable 1. Both studies enrolled adult stroke survivors without other major neurologic conditions >6-months poststroke, as well as demographically matched neurologically healthy adults.
To examine neural correlates of language, we used a well-validated fMRI adaptive semantic matching paradigm^1^ in which participants see pairs of written words and decide whether the words are semantically related, contrasted with a control condition during which participants judge visual similarity between pairs of nonlinguistic symbol strings. Visual field mapping was performed using a flickering checkerboard stimulus.
MRI was acquired on a 3T Siemens Prisma scanner. High-resolution T1-weighted MPRAGE and FLAIR sequences were obtained to visualize anatomy and assist in lesion tracing. Lesions were manually segmented on coregistered MPRAGE and FLAIR images using ITK-SNAP imaging and segmentation software by a board-certified neurologist (P.E.T.). Images and lesion masks were normalized to MNI space using the Clinical Toolbox Older Adult Template.^2^
Standard Protocol Approvals, Registrations, and Patient Consents
The participant provided written informed consent under Georgetown University IRB-approved protocols: IRB2017–0305 and IRB2013–0964. She also reviewed the manuscript and signed a consent-to-disclose form. To protect confidentiality, a randomly generated three-letter code (ECP) is used instead of patient initials, and data not published within this article are not shared.
Results
ECP was a 42-year-old right-handed high school graduate who presented with right-sided hemiparesis, partial left gaze deviation, dysarthria, and altered mental state following a motor vehicle accident. She was found to have an occlusion of the left proximal internal carotid artery causing acute left middle and anterior cerebral artery (ACA) territory ischemia with a significant mass effect. ECP was ineligible for tissue plasminogen activator treatment or mechanical thrombectomy due to last seen normal being well outside the therapeutic window. She was instead treated with mannitol to manage cerebral edema. The NIH Stroke Scale (NIHSS) was 13 on admission. She was enrolled in an observational study of chronic stroke outcomes 61 months after the stroke. At this time, her NIHSS was 10 for right hemianopsia, facial droop, hemiparesis, hemisensory loss, and tactile extinction. Imaging revealed substantial area of encephalomalacia of 432 cm^3^ affecting left frontal, temporal, and parietal regions encompassing the entire MCA territory and the posterior portion of the ACA territory (Figure 1).
Despite the lesion’s size and considerable overlap with tissue typically associated with language function,^3–5^ ECP displayed no language deficits in the acute phase based on both medical records and retrospective history provided by ECP and family members. Language assessments at 61- and 86-month post-stroke also revealed no aphasia. On the WAB,^6^ where a score greater than 93.8 indicates no aphasia and a score of 100 indicates perfect performance, ECP scored 99.2. Among a cohort of 95 LH stroke survivors who participated in the same study, the median score was 87.5. All other participants with scores above 93.8 had lesions less than half the size of that of ECP (Figure 2A). ECP performed within 1 SD of the mean of an education-matched healthy control group on reading and spelling tasks (real word reading: z = 0.26; pseudoword reading: z = 0.15; typing to dictation: z = −0.66). Limb and oral praxis, which are typically left-lateralized,^7^ were also intact based on the Apraxia Battery for Adults^8^; Limb 50/50, Oral 48/50.
On the adaptive semantic matching fMRI paradigm,^1^ where neurologically healthy adults showed the expected pattern of activation in the left inferior gyrus (IFG), temporal regions, and right cerebellum (Figure 2B), ECP demonstrated robust activation in the right IFG and right temporal regions, along with the left cerebellum, showing a mirror reversal of the typical activation pattern (Figure 2B). Premorbidly, ECP was right-handed (retrospective Edinburgh Handedness Inventory Index = 70),^9^ and she denied having left-handed first-degree relatives. She also denied any history of symptoms indicative of left-hemisphere injury or dysfunction early in life that could have explained her atypical language dominance.
Further testing at 86-month poststroke revealed no visuospatial or attentional deficits. On the WASI-II Block Design,^10^ ECP’s scaled score of 10 corresponded to the healthy norming sample and exceeded the mean of 32 other RH stroke survivors enrolled in the same study (Figure 3A). ECP scored 29/30 on the MoCA, with a 3/3 on the serial sevens section. On the Behavioral Inattention Test conventional subset (BIT-c),^11^ she scored 143/146, with no lateralized deficits on cancellation, line bisection, or drawing tasks (Figure 3B). A computerized line bisection task with reversed motor mapping^12^ also revealed no motor-intentional neglect.
Visual field testing confirmed a right homonymous hemianopsia. fMRI showed absent activation in the left occipital cortex in response to right visual field stimulation (Figure 3C), and structural imaging revealed damage to the left optic radiation and lateral geniculate nucleus. Given this combination of right hemianopsia and lack of lateralized deficits on neglect tests with free visual exploration, the presence of tactile extinction on the NIHSS likely reflects partial hemisensory loss or tactile inattention without visuospatial neglect.
Discussion
This case presents a rare instance of preserved cognitive performance for language, praxis, and visuospatial functions following a large left MCA ischemic stroke. The absence of aphasia and the presence of right-lateralized language activation suggest premorbid RH dominance for language in this right-handed individual. Although this conclusion is inferential, it is consistent with epidemiologic evidence that a minority of right-handed individuals (~7.5%) demonstrate right-hemisphere language.^13^
Most published examples of atypical lateralization describe crossed aphasia after right-hemisphere stroke in right-handed individuals (eTable 2). Selnes et al.^14^ reported a case in which a left MCA infarct spared language but produced neglect and other deficits, typically associated with right-hemisphere injury. This is consistent with neuroimaging work showing that atypical lateralization of the RH is often accompanied by lateralization of typically right-lateralized functions (such as visuospatial processing) to the left, maintain a functional hemispheric segregation.^15^ In violation of this mirror pattern, ECP preserved both language and right-hemisphere functions. These findings support the view that lateralization biases for different cognitive domains can vary independently, allowing, in rare instances, lateralization of language, praxis, and visuospatial functions to the same hemisphere.
Clinically, atypical lateralization is often noted based on crossed deficits (e.g., aphasia resulting from RH stroke). This case demonstrates that alternative patterns of hemispheric organization may also occur and should be considered during assessment and treatment planning when anticipated cognitive deficits are absent.
Supplementary Material
eTables1and2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilson SM, Yen M, Eriksson DK. An adaptive semantic matching paradigm for reliable and valid language mapping in individuals with aphasia. Hum Brain Mapp. 2018;39(8):3285–3307. doi:10.1002/hbm.2407729665223 PMC 6045968 · doi ↗ · pubmed ↗
- 2Rorden C, Bonilha L, Fridriksson J, Bender B, Karnath H-O. Age-specific CT and MRI templates for spatial normalization. Neuroimage. 2012;61(4):957–965. doi:10.1016/j.neuroimage.2012.03.02022440645 PMC 3376197 · doi ↗ · pubmed ↗
- 3Wernicke C (1874). Der aphasische Symptomencomplex: eine psychologische Studie auf anatomischer Basis. Cohn.
- 4Price CJ. A review and synthesis of the first 20years of PET and f MRI studies of heard speech, spoken language and reading. Neuroimage. 2012;62(2):816–847. doi:10.1016/j.neuroimage.2012.04.06222584224 PMC 3398395 · doi ↗ · pubmed ↗
- 5Broca P Sur la faculté générale du language, dans ses rapports avec la faculté du language articulé. Bull de La Société d’Anthropologie (Deuxième Série) 1866;1:377–382.
- 6Kertesz A The Western aphasia battery: a systematic review of research and clinical applications. Aphasiology. 2022;36(1):21–50. doi:10.1080/02687038.2020.1852002 · doi ↗
- 7Vingerhoets G, Alderweireldt A-S, Vandemaele P, Praxis and language are linked: evidence from co-lateralization in individuals with atypical language dominance. Cortex. 2013;49(1):172–183. doi:10.1016/j.cortex.2011.11.00322172977 · doi ↗ · pubmed ↗
- 8Dabul B Apraxia Battery For Adults, Examiner’s Manual 2000.