The proportion of chronic periprosthetic joint infection patients with Candida isolates
Samuelson E. Osifo, Adrian Santana, Michael F. Shannon, Victoria R. Wong, Caroline F. Tyndall, Christian Cisneros, Niosha Parvizi, Brian A. Klatt, Johannes F. Plate, Nicolas S. Piuzzi, Kenneth L. Urish

TL;DR
This study estimates that Candida fungi are involved in about 5% of joint infections, with higher rates in chronic cases that don't respond to treatment.
Contribution
The study introduces a novel method to adjust for underreporting biases in fungal joint infection data using imputation techniques.
Findings
Candida involvement in PJI was estimated at 5.1% after adjusting for under-ascertainment biases.
Chronic refractory PJI cases had a likely Candida incidence exceeding 10%.
Adjustment methods revealed a wide range of 1.4% to 13.6% for Candida-associated PJI.
Abstract
Introduction: Fungal periprosthetic joint infection (PJI) has historically been reported in 1 %–2 % of cases, with Candida species accounting for most isolates. However, the true incidence is likely underestimated. Standard aerobic and anaerobic culture techniques have limited sensitivity for detecting fungi, single positive fungal cultures are often excluded or inconsistently classified, culture-negative infections may mask low-burden fungal pathogens, and polymicrobial cultures may obscure the contribution of fungal organisms. The objective of this study was to quantify the burden of potentially unrecognized fungal involvement and provide a more accurate estimate of the incidence of Candida-associated PJI. Methods: Following a systematic literature search, we performed a quantitative sensitivity analysis using imputation with informative missingness odds ratios (IMORs). Reported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
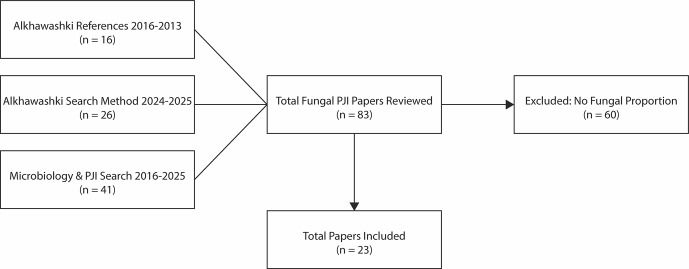 Figure 1
Figure 1| Reason for missingness | ||||
|---|---|---|---|---|
| How missingness was reported | Culture-negative cases | Polymicrobial cases (species not specified) | Single positive | Absence of high-sensitivity microbiologic testing |
| Included in total PJI count and | No imputation | No imputation | No imputation | No imputation |
| Included in total PJI count but not in | Best – Add | Best – Add | | |
| Excluded | Best – Add | Best – Add | Best – Add | Best – Add |
| Not reported | Best – Add | Best – Add 0 Worst – Add | Best – Add 0 Worst – Add | Best – Add 0 Worst – Add |
| Reference | Number | Candida | Candida | Rate of | High- |
|---|---|---|---|---|---|
| of PJI | rate in | rate in | single | sensitivity | |
| cases | culture- | polymicrobial |
| test method | |
| negative | PJI | cultures | |||
| PJI | in PJI | ||||
| Brown et al. (2018) | 3525 | 0.37 | |||
| Tai et al. (2022a) | 2,067 | 0.49 | |||
| Tai et al. (2022b) | 1162 | 0.35 | |||
| van den Bijllaardt et al. (2019) | 90 | 0.30 | |||
| Enz et al. (2021) | 117 | 0.78 | |||
| Cao et al. (2025) | 278 | 0.27 | |||
| Froschen et al. (2022) | 432 | 0.05 | |||
| Mei et al. (2023) | 91 | 0.14 | |||
| Ull et al. (2020) | 124 | 0.17 | |||
| Goswami et al. (2022) | 301 | 0.08 | |||
| Lin et al. (2025) | 232 | 0.13 | |||
| Weighted average | 0.10 | 0.21 | 0.41 | 0.35 |
| Reference | Number | Number of | Single | Total |
|
|---|---|---|---|---|---|
| of PJI |
| cultures | cases | proportion | |
| cases | cases | excluded | with | ||
| reported | reported |
| |||
| isolates | |||||
| Baecker et al. (2021) | 623 | 20 | 20 | 3.2 % | |
| Lee et al. (2024) | 181 | 13 | 13 | 7.2 % | |
| Lin et al. (2025) | 271 | 16 | 16 | 5.9 % | |
| Lyu et al. (2024) | 219 | 13 | 13 | 5.9 % | |
| Morreel et al. (2025) | 187 | 2 | 2 | 1.1 % | |
| Tai et al. (2022b) | 1162 | 40 | 39 | 79 | 3.4 % |
| Wu et al. (2025) | 201 | 4 | 4 | 2.0 % | |
| Aunon et al. (2025) | 499 | 12 | 12 | 2.4 % | |
| Froschen et al. (2022) | 432 | 17 | 17 | 3.9 % | |
| Jiang et al. (2025) | 255 | 7 | 7 | 2.7 % | |
| Ull et al. (2020) | 124 | 5 | 5 | 4.0 % | |
| Brown et al. (2018) | 3525 | 31 | 18 | 49 | 0.9 % |
| Herndon et al. (2023) | 3989 | 73 | 73 | 1.8 % | |
| Tsai et al. (2019) | 294 | 10 | 10 | 3.4 % | |
| Budin et al. (2025) | 3645 | 47 | 47 | 1.3 % | |
| Cao et al. (2025) | 278 | 28 | 28 | 10.1 % | |
| Kuo et al. (2018) | 1184 | 29 | 29 | 2.4 % | |
| Sidhu et al. (2019) | 1189 | 22 | 22 | 1.9 % | |
| Benito et al. (2016) | 2524 | 30 | 30 | 1.2 % | |
| Ergin et al. (2024) | 2569 | 49 | 49 | 2.0 % | |
| Ergin et al. (2025) | 4261 | 45 | 45 | 1.1 % | |
| Haraldsdottir et al. (2025) | 293 | 6 | 6 | 2.0 % | |
| Yang et al. (2024) | 348 | 14 | | 14 | 4.0 % |
| Totals and grand mean (%) | 28 253 | 533 | 57 | 590 | 2.1 % |
| Imputation for missing data | ||||
|---|---|---|---|---|
| Reference | Culture- | Polymicrobial | Excluded | Absence |
| negative | PJI cases | single | of high- | |
| PJI cases | without | positive | sensitivity | |
| species |
| microbiologic | ||
| specification | isolates | testing | ||
| Missing data for one reason | ||||
| Baecker et al. (2021) | Yes | n/a | n/a | n/a |
| Lee et al. (2024) | Yes | n/a | n/a | n/a |
| Lin et al. (2025) | Yes | n/a | n/a | n/a |
| Lyu et al. (2024) | n/a | n/a | n/a | Yes |
| Morreel et al. (2025) | Yes | n/a | n/a | n/a |
| Tai et al. (2022b) | Yes | n/a | n/a | n/a |
| Missing data for two reasons | ||||
| Wu et al. (2025) | Yes | Yes | n/a | n/a |
| Aunon et al. (2025) | Yes | n/a | Yes | n/a |
| Froschen et al. (2022) | Yes | n/a | Yes | n/a |
| Jiang et al. (2025) | Yes | n/a | Yes | n/a |
| Ull et al. (2020) | Yes | n/a | Yes | n/a |
| Brown et al. (2018) | Yes | n/a | n/a | Yes |
| Herndon et al. (2023) | Yes | n/a | n/a | Yes |
| Missing data for three reasons | ||||
| Tsai et al. (2019) | Yes | n/a | Yes | Yes |
| Budin et al. (2025) | Yes | n/a | Yes | Yes |
| Cao et al. (2025) | Yes | n/a | Yes | Yes |
| Kuo et al. (2018) | Yes | n/a | Yes | Yes |
| Sidhu et al. (2019) | Yes | n/a | Yes | Yes |
| Missing data for four reasons | ||||
| Benito et al. (2016) | Yes | Yes | Yes | Yes |
| Ergin et al. (2024) | Yes | Yes | Yes | Yes |
| Ergin et al. (2025) | Yes | Yes | Yes | Yes |
| Haraldsdottir et al. (2025) | Yes | Yes | Yes | Yes |
| Yang et al. (2024) | Yes | Yes | Yes | Yes |
| Reference | Total | Reported | Reported | Minimum | Maximum |
|---|---|---|---|---|---|
| PJI |
|
| expected | expected | |
| cases | cases | proportion |
|
| |
| proportion | proportion | ||||
| Baecker et al. (2021) | 623 | 20 | 3.2 % | 3.2 % | 4.0 % |
| Lee et al. (2024) | 181 | 13 | 7.2 % | 9.4 % | 9.4 % |
| Lin et al. (2025) | 271 | 16 | 5.9 % | 6.3 % | 6.3 % |
| Lyu et al. (2024) | 219 | 13 | 5.9 % | 5.9 % | 6.4 % |
| Morreel et al. (2025) | 187 | 2 | 1.1 % | 1.9 % | 1.9 % |
| Tai et al. (2022b) | 1162 | 79 | 3.4 % | 7.3 % | 7.3 % |
| Wu et al. (2025) | 201 | 4 | 2.0 % | 5.0 % | 5.0 % |
| Aunon et al. (2025) | 499 | 12 | 2.4 % | 2.4 % | 3.9 % |
| Froschen et al. (2022) | 432 | 17 | 3.9 % | 3.9 % | 5.1 % |
| Jiang, et al. (2025) | 255 | 7 | 2.7 % | 3.9 % | 4.7 % |
| Ull et al. (2020) | 124 | 5 | 4.0 % | 4.8 % | 4.8 % |
| Brown et al. (2018) | 3525 | 49 | 0.9 % | 1.4 % | 2.9 % |
| Herndon et al. (2023) | 3989 | 73 | 1.8 % | 2.7 % | 3.3 % |
| Tsai et al. (2019) | 294 | 10 | 3.4 % | 6.1 % | 6.8 % |
| Budin et al. (2025) | 3645 | 47 | 1.3 % | 2.2 % | 3.5 % |
| Cao et al. (2025) | 278 | 28 | 10.1 % | 12.2 % | 13.6 % |
| Kuo et al. (2018) | 1184 | 29 | 2.4 % | 3.2 % | 4.6 % |
| Sidhu et al. (2019) | 1189 | 22 | 1.9 % | 1.9 % | 4.0 % |
| Benito et al. (2016) | 2524 | 30 | 1.2 % | 5.5 % | 6.9 % |
| Ergin et al. (2024) | 2569 | 49 | 2.0 % | 8.7 % | 9.8 % |
| Ergin et al. (2025) | 4261 | 45 | 1.1 % | 7.1 % | 8.3 % |
| Haraldsdottir et al. (2025) | 293 | 6 | 2.0 % | 5.8 % | 7.1 % |
| Yang et al. (2024) | 348 | 14 | 4.0 % | 10.3 % | 11.7 % |
| Total and grand mean (%) | 28 253 | 590 | 2.1 % | 5.1 % | |
- —National Institute of Arthritis and Musculoskeletal and Skin Diseases
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Musculoskeletal synovial abnormalities and treatments · Antifungal resistance and susceptibility
Introduction
1
Periprosthetic joint infection (PJI) remains the most serious complication of hip and knee arthroplasty globally and the leading cause of early revision in total knee arthroplasty (Del Pozo and Patel, 2009; Kurtz et al., 2007). Fungal PJI has traditionally been considered rare, historically reported in 1 %–2 % of PJI cases (Sambri et al., 2022; Sidhu et al., 2019; Tande and Patel, 2014). However, contemporary evidence from large primary cohorts suggests that fungal organisms may be present in a substantially higher proportion (up to 10 %) of PJI cases (Brown et al., 2018; Cao et al., 2025). Candida species account for approximately 95 % of culture-confirmed fungal PJIs (Benito et al., 2016; Koutserimpas et al., 2022; Herndon et al., 2023; McCulloch et al., 2023).
Several factors likely contribute to systematic underestimation of fungal involvement in chronic PJI. Conventional aerobic and anaerobic culture methods have reduced sensitivity for Candida, particularly in low-burden infections or polymicrobial communities, making both single isolates and mixed fungal–bacterial infections difficult to detect (Watanabe et al., 2024). Underreporting may also occur in culture-negative cases, especially in institutions without optimized fungal culture protocols or prolonged incubation. Diagnostic uncertainty is further compounded when a single Candida isolate is dismissed as contamination, leading to misclassification. Additionally, many published series further aggregate acute and chronic PJI, although fungal infections occur predominantly in chronic refractory cases.
The objective of this study was to assess how these diagnostic and reporting limitations influenced the observed incidence of fungal PJI. Specifically, we aimed to (1) establish the baseline proportion of Candida isolates among confirmed PJI cases; (2) identify the frequency of missing, excluded, or misclassified variables that could obscure true fungal involvement; and (3) quantify the adjusted incidence of Candida-associated PJI after correcting for potential underreporting.
Methods
2
Study design
2.1
This study was a quantitative sensitivity analysis of published clinical series reporting microbiologic findings in confirmed periprosthetic joint infection (PJI). The primary outcome was the proportion of PJI cases with evidence of Candida involvement. The analysis was designed to evaluate the impact of incomplete or inconsistently reported microbiologic data on observed estimates of Candida involvement across heterogeneous clinical studies.
Data sources and study selection
2.2
A recent meta-analysis identified English-language publications reporting outcomes on patients with diagnosed hip or knee fungal PJI between 2009 and 2023 (Alkhawashki et al., 2025). All studies published between 2016 and 2023 included in this meta-analysis were reviewed. To extend capture beyond this cohort, a structured literature search was independently conducted for studies published from January 2024 through October 2025 using PubMed. The primary search string was “fungal periprosthetic joint infection”, applied to titles and abstracts. In parallel, a secondary PubMed search was performed, following the methodology described by Tai et al. (2022a), using the Boolean search strategy “hip” OR “knee” AND “periprosthetic joint infection” AND “microbiology aetiology” for publications from 2016 through October 2025. Reviewed studies were included if they reported microbiologic results from preoperative or intraoperative samples and allowed calculation of the proportion of PJI cases with evidence of Candida involvement. Studies were excluded if microbiologic data were insufficient to determine Candida involvement. This process yielded 23 studies for inclusion (Fig. 1).
Flow diagram of literature search and study selection.
Identification of missing microbiologic data
2.3
The proportion of PJI patients with Candida-positive preoperative or intraoperative cultures was calculated for each study included. Review of included studies revealed inconsistent methodology and reporting practices, resulting in missing diagnostic data relevant to the calculated proportion of Candida involvement. Four prespecified sources of missingness were identified:
- Culture-negative PJI cases included without clarification of fungal assessment;
- Polymicrobial PJI cases without species-level reporting, where fungal organisms may have been present but not specified;
- Exclusion of single positive Candida isolates, commonly dismissed as contaminants;
- Variable sensitivity of microbiologic methods, with potential under-detection of fungal organisms.
Sensitivity analysis and imputation strategy
2.4
A quantitative sensitivity analysis was conducted using imputation with informative missingness odds ratios (IMORs) for each missingness category, following methods for imputing missing outcome data in meta-analyses of clinical trials (Higgins et al., 2008). For each study, the expected number of missed Candida cases was estimated under both best-case and worst-case scenarios. These expected cases were added to the reported number of Candida infections, and minimum and maximum adjusted proportions were calculated. A sample size-weighted mean and range of expected Candida proportions was generated across all included studies.
Consistent with Higgins et al. (2008), the analysis did not assume that missing patients were either entirely “all Candida” or “no Candida.” Instead, each category of missingness was assigned a relative risk (RR) of Candida involvement based on published clinical data. Applying these literature-derived probabilities provides more realistic estimates and reduces the standard error compared with traditional all-or-none assumptions. The additional number of expected Candida cases for each missingness category was calculated as , where represents the number of PJI cases affected by that specific source of missingness.
The number of PJI patients with missing data for Candida is often reported directly in the paper (e.g., number of culture-negative patients). If such patients are excluded, or not reported and assumed to be excluded in worst-case sensitivity calculations, the number of missing patients ( ) was calculated by multiplying the total number of PJI patients in the study ( ) by the proportion ( ) of PJI patients in the literature with the same reason for missingness (e.g., percentage of culture-negative PJI cases): .
The relative risk of Candida for each missingness category (RR_ i _) was derived from the literature. For missed cases attributable to insensitive microbiologic test methods, RR was calculated as the difference in the probability of detecting Candida using high-sensitivity methods compared with conventional culture techniques reported in the publication. Imputation was restricted to Candida involvement because fungal organisms are inconsistently assessed and variably reported across published PJI series, with frequent exclusion of single positive cultures, lack of species-level reporting in polymicrobial infections, and heterogeneous use of high-sensitivity diagnostic methods. These factors introduce systematic uncertainty in estimates of fungal involvement that cannot be addressed by standard reporting alone.
Best-case and worst-case scenarios
2.5
Best-case and worst-case scenarios were defined to bound the plausible range of Candida involvement under varying assumptions regarding missing microbiologic data. The best-case and worst-case scenarios of the sensitivity analysis for each missingness reason were determined (Table 1). These scenarios depend on whether PJI patients were included in the study without microbial data, specifically excluded from the study, or not reported (and therefore potentially included or excluded). When patients with expected Candida involvement were known to be missing, they were added to both the best-case and worst-case scenarios. If the number of PJI patients affected by a missingness category was not reported, no imputation was performed for the best-case scenario (Add 0). When PJI patients were excluded or assumed to be excluded in worst-case scenarios, the number of missing PJI patients for that reason ( ) was added to the total number of PJI patients before recalculating the proportion of patients expected to have Candida involvement, to avoid overestimation.
Informative missingness odds ratios (IMORs)
2.6
The relative risks associated with each missingness category were derived from published literature reporting the proportion of cases with Candida isolates associated with each source of missingness, including the following:
- Detection of Candida in culture-negative PJI using next-generation sequencing (NGS).
- The proportion of Candida in polymicrobial PJI.
- The frequency of single positive Candida cultures in PJI.
- The detection of Candida by high-sensitivity microbial assays missed by conventional cultures.
The IMOR for each category was calculated as a weighted average across included studies (Table 2).
Results
3
A total of 23 studies met inclusion criteria, reporting a combined total of 28 253 PJI patients (Table 3). Candida PJI was identified in 533 patients (1.9 %). When patients with a single positive Candida culture were included, the total increased to 590 patients (2.1 %). Across all included studies, the reported incidence of Candida PJI ranged from 0.9 % to 10.1 %.
Each study was assessed for missing diagnostic data that could lead to underestimation of Candida involvement (Table 4). The major sources of missingness included (1) culture-negative PJI cases in which fungal involvement could not be excluded, (2) polymicrobial PJI cases where the full microbial profile was not reported, (3) exclusion or non-classification of single positive Candida isolates, and (4) the absence of high-sensitivity microbiologic testing such as fungal cultures, next-generation sequencing (NGS), or sonication.
Among all included studies, only the series by Lyu et al. (2024), which used NGS to detect Candida in culture-negative cases, did not require imputation for the culture-negative category. Missingness due to unreported polymicrobial species required imputation in 6 studies, exclusion of single positive Candida isolates in 13 studies, and absence of high-sensitivity culture methods in 12 studies. The incidence of Candida PJI was then recalculated after applying imputation for each missingness category (Table 5).
After adjusting for missing data, the expected proportion of Candida PJI increased to 5.1 % across all studies (range: 1.4 %–13.6 %). This estimate was derived by adding the expected number of additional Candida cases for each missingness variable (Table A1). Most adjustments were attributable to unreported microbial species in polymicrobial cases (53 %) and unknown microbiology in culture-negative PJI cases (30 %).
As a sensitivity check, the subset of six studies requiring only one imputation correction, representing the lowest potential risk of error from multiple imputations, yielded an expected Candida incidence of 5.9 % (range: 1.9 % to 9.4 %). This is consistent with the overall adjusted estimate and supports the robustness of the findings.
Discussion
4
This quantitative sensitivity analysis suggests that the contribution of Candida to PJI is substantially underestimated in the published literature. After imputing missing microbiologic data across 28 253 confirmed PJI cases from 23 clinical studies, the expected proportion of Candida-associated PJI increased to approximately 5 %–6 % (range: 1.4 %–13.6 %). This estimate is more than double the conventionally reported incidence of 1 %–2 % and represents a clinically meaningful difference for diagnosis, treatment planning, and prognostication. By explicitly accounting for multiple, well-described sources of microbiologic under-ascertainment, this analysis provides an adjusted estimate of Candida involvement that complements existing epidemiologic reports. Notably, more than half of the included studies were published within the past decade, with a marked increase in reports from 2024–2025, reflecting growing recognition of fungal involvement in PJI.
Missing data were common and required imputation for all of the 23 studies. The most frequent source of missingness was failure to report organism-level microbiology in polymicrobial infections. Because polymicrobial PJI appears to carry a relatively high expected proportion of Candida, greater than 20 % in this analysis, failure to characterize all identified organisms may substantially underestimate fungal involvement.
Although the expected proportion of Candida was calculated for all reported PJI cases, fungal pathogens are most frequently encountered in chronic refractory infections and in sub-populations with risk factors associated with chronic PJI treatment failure. In a recent series of 193 chronic PJI cases treated with two-stage exchange, Candida accounted for 7.2 % of infections, increasing to 9.4 % when adjusted with the current methodology (Lee et al., 2024). Multiple studies have demonstrated strong associations between Candida PJI and clinical factors characteristic of chronic refractory infection, including prolonged infection duration, multiple prior surgeries, obesity, diabetes mellitus, presence of a draining sinus, polymicrobial infection, and recent antibiotic exposure. The reported odds ratios range from 2.2 to 7.2 (Aunon et al., 2025; Ergin et al., 2024, 2025; Gross et al., 2021; Kuo et al., 2018; Luo et al., 2025; Riaz et al., 2020). These data collectively support an expected Candida proportion of approximately 10 % in chronic refractory PJI cases, the upper estimate of our quantitative analysis.
An important consideration is whether imputation of missing microbiologic data selectively inflates estimates of Candida involvement or instead reflects broader limitations in microbiologic characterization within published PJI series. Staphylococcal species, particularly Staphylococcus aureus and S. epidermidis, account for more than half of reported PJI cases and are more consistently identified and reported in routine clinical practice. However, even for bacterial pathogens, culture-negative and polymicrobial cases remain common, indicating that missingness reflects incomplete or heterogeneous microbiologic reporting rather than organism-specific bias. This analysis does not suggest that Candida replaces bacterial pathogens within culture-negative infections but rather that fungal involvement is under-recognized within a subset of these cases. Collectively, these findings underscore that missingness imputation does not “create” fungal infections but instead quantifies uncertainty arising from inconsistent application and reporting of microbiologic diagnostic methods.
This study has several limitations. The inability to stratify results by specific risk factors limits granularity and reflects a broader challenge in fungal PJI research: microbiologic data are inconsistently reported and often aggregated across heterogeneous patient populations. Additional limitations include reliance on retrospective studies, the relatively small cohort of confirmed fungal PJI cases, and the limited number of publications with sufficient detail to calculate risk ratios for each category of missing data. The imputed expected proportions represent extrapolations based on available information rather than true corrections derived from recovered data, and errors may be magnified in studies with multiple sources of missing data.
Conclusion
5
A quantitative sensitivity analysis of missing microbiologic data suggests that the contribution of Candida to PJI is likely underestimated. The expected proportion of Candida-associated PJI is at least 5 % of all confirmed PJI cases and closer to 10 % among patients with chronic refractory infections. The discrepancy between reported and expected incidence highlights the need for prospective, multi-center studies that incorporate high-sensitivity fungal diagnostics, including prolonged culture, molecular testing, and standardized reporting of polymicrobial infections. More accurate estimates of Candida involvement in PJI will strengthen risk stratification and better inform surgical and antimicrobial decision-making, particularly for patients with complex or treatment-resistant infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alkhawashki H Benevenia J Drago L Kadkoy Y A One- or Two-Stage Revision of Fungal Prosthetic Joint Infection: A Review of Current Knowledge, Pitfalls and Recommendations Antibiotics (Basel)1465810.3390/antibiotics 14070658202540723961 PMC 12291646 · doi ↗ · pubmed ↗
- 2Aunon A Ortiz I Penarrubia S Alvaro C Torrecilla-Sadaba E Garcia-Canete J Esteban J Polymicrobial Prosthetic Joint Infections: Unraveling Risk Factors and Outcomes in a Single-Center Study Microorganisms 13167910.3390/microorganisms 13071679202540732188 PMC 12298575 · doi ↗ · pubmed ↗
- 3Baecker H Frieler S Gessmann J Pauly S Schildhauer TA Hanusrichter Y Three-stage revision arthroplasty for the treatment of fungal periprosthetic joint infection: outcome analysis of a novel treatment algorithm: a prospective study Bone Jt Open 267167810.1302/2633-1462.28.BJO-2021-0002.R 2202134406077 PMC 8384437 · doi ↗ · pubmed ↗
- 4Benito N Franco M Ribera A Soriano A Rodriguez-Pardo D Sorli L Fresco G Fernandez-Sampedro M Dolores Del Toro M Guio L Sanchez-Rivas E Bahamonde A Riera M Esteban J Baraia-Etxaburu JM Martinez-Alvarez J Jover-Saenz A Duenas C Ramos A Sobrino B Euba G Morata L Pigrau C Coll P Mur I Ariza J the REIPI (Spanish Network for Research in Infectious Disease) Group for the Study of Prosthetic Joint Infections Time trends in the aetiology of prosthetic joint infections: a multicentre cohort study Clin Microbiol Infect 2273173810.101 · doi ↗ · pubmed ↗
- 5Brown TS Petis SM Osmon DR Mabry TM Berry DJ Hanssen AD Abdel MP Periprosthetic Joint Infection With Fungal Pathogens J. Arthroplasty 332605261210.1016/j.arth.2018.03.003201829636249 · doi ↗ · pubmed ↗
- 6Budin M Sandiford NA Gehrke T Citak M Body mass index matters: morbid obese patients have different microorganism profiles in the setting of periprosthetic hip joint infections Int Orthop 491309131710.1007/s 00264-025-06513-4202540183945 · doi ↗ · pubmed ↗
- 7Cao Q Fan P Feng J Cheng T Wang X Cheng C Dai Z Comprehensive analysis of the pathogen spectrum and antibiotic resistance profiles in periprosthetic joint infections: a single center retrospective study Front Surg 12156668910.3389/fsurg.2025.1566689202540182306 PMC 11966497 · doi ↗ · pubmed ↗
- 8Del Pozo JL Patel R Clinical practice. Infection associated with prosthetic joints N Engl J Med 36178779410.1056/NEJ Mcp 0905029200919692690 PMC 2850113 · doi ↗ · pubmed ↗