Anatomical Variations of the Neurovascular Structures of the Hand and the Clinical Significance
Slobodan Kapor, Predrag Bjelogrlic, Valentina Simic, Drazan Eric, Suncica Kapor, Fraser Chisholm, Enis Cezayirli, Darko Laketic

TL;DR
This study examines anatomical variations in the hand's neurovascular structures and their clinical importance for surgery and diagnostics.
Contribution
The study provides new insights into sex-based differences in hand anatomy and the prevalence of Berrettini anastomoses.
Findings
Complete superficial palmar arches were more common in males, while incomplete arches were more frequent in females.
CDP arteries were significantly farther from Kaplan’s line in males compared to females.
Berrettini anastomoses occurred in 33.3% of hands, with Type III being the most common.
Abstract
Background Anatomical variations in the neurovascular structures of the hand have critical implications for surgical procedures, diagnostic accuracy, and nerve conduction studies. This study examined the morphology of the superficial palmar arch (SPA), the course of common digital palmar (CDP) arteries relative to Kaplan’s line, and the prevalence and types of Berrettini anastomosis. Methods Thirty-six embalmed cadaveric upper limbs (18 right, 18 left) from the Universities of Belgrade and St Andrews were dissected following standard anatomical protocols. Specimens with visible trauma or deformity were excluded. The SPA was classified as complete or incomplete. Origins of CDP artery distances from Kaplan’s line were measured and analyzed for sex differences using the t- test (p < 0.05). Median-ulnar nerve communications were identified and categorized as Type I (ulnar to median),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
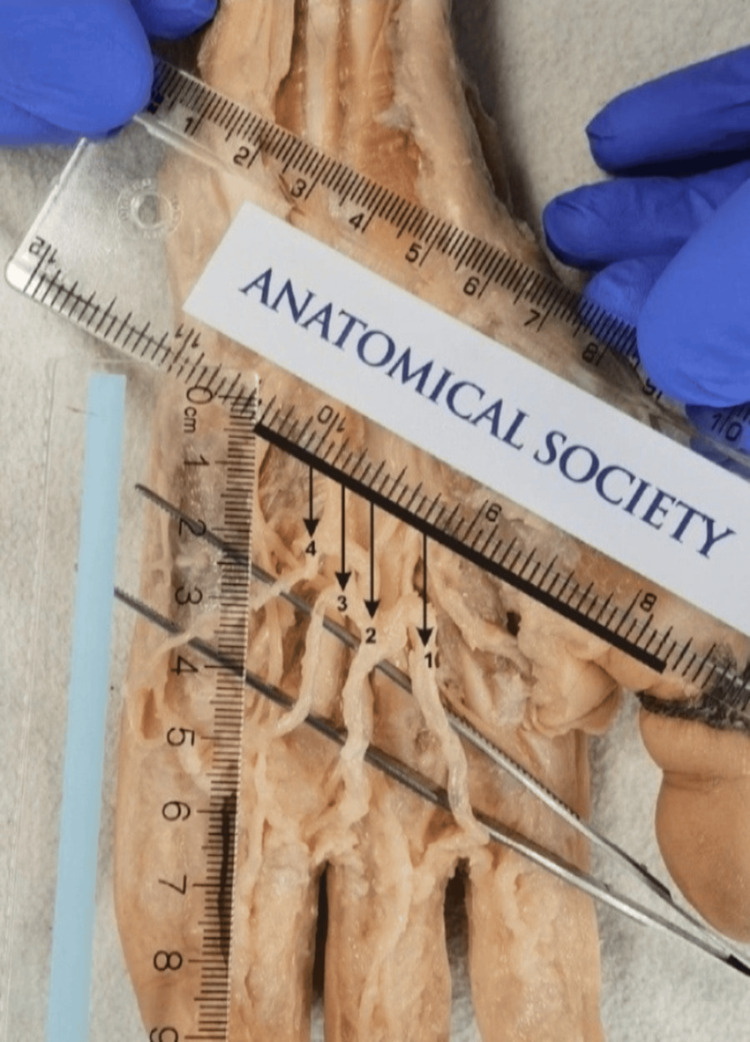 Figure 1
Figure 1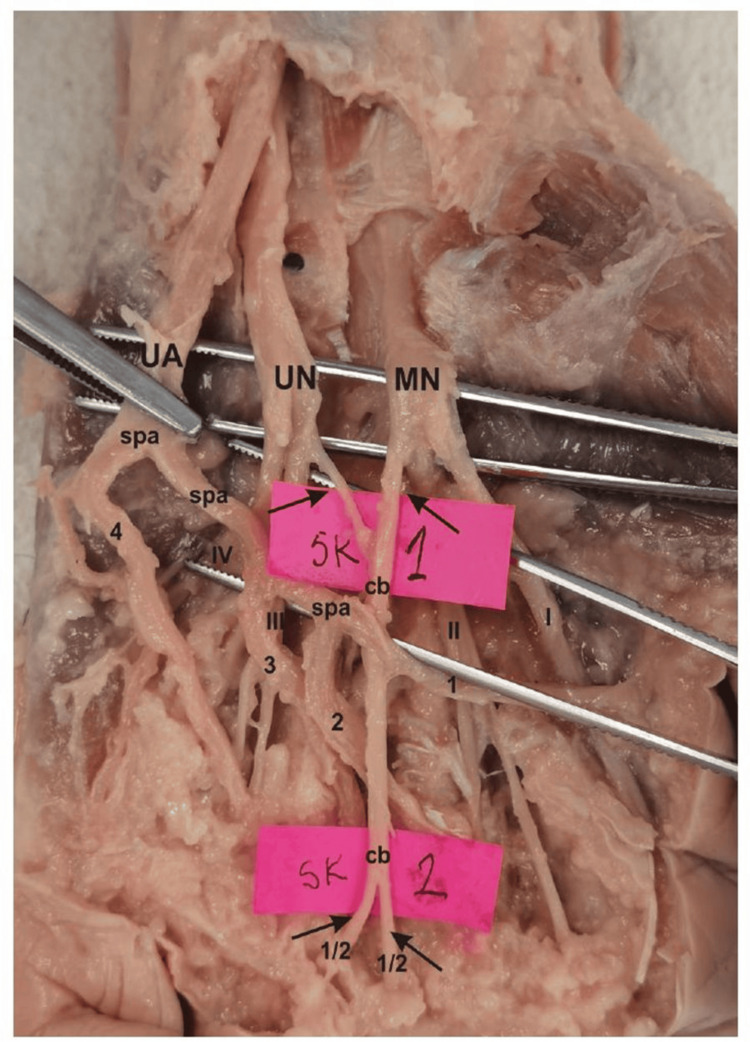 Figure 2
Figure 2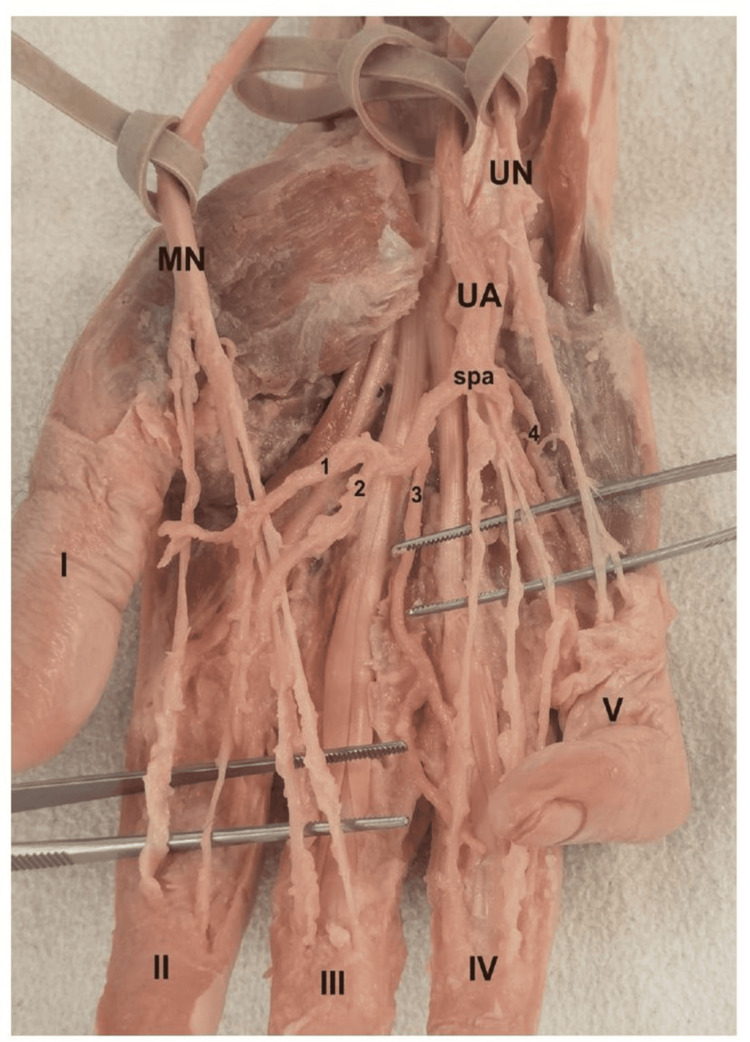 Figure 3
Figure 3| Artery | Female (n=20), mean ± SD | Male (n=16), mean ± SD | p-value | t-test statistic |
| 4th CDP | 1.08 ± 0.17 cm | 1.60 ± 0.15 cm | p< 0.05* | t= -7.56 |
| 3rd CDP | 1.35 ± 0.17 cm | 1.76 ± 0.15 cm | p< 0.05* | t= -6.06 |
| 2nd CDP | 1.58 ± 0.13 cm | 2.96 ± 0.15 cm | p< 0.05* | t= -6.56 |
| 1st CDP | 1.81 ± 0.11 cm | 2.21 ± 0.15 cm | p< 0.05* | t= -9.38 |
| Parameter | Total number | Percentage of 36 Hands | Percentage of 12 Positive Cases |
| Hands with any anastomosis (Type II/III) | 12 | 33.3% | 100% |
| • Type I (U → M) | 0 | 0% | 0% |
| • Type II (M → U) | 4 | 11.1% | 33.3% |
| • Type III (bidirectional/multiple) | 8 | 22.2% | 66.7% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Nerve Disorders · Orthopedic Surgery and Rehabilitation · Reconstructive Surgery and Microvascular Techniques
Introduction
The ulnar artery is a major vessel in the upper limb. It comes from the brachial artery near the cubital fossa and travels along the inner forearm before entering the hand. It passes above the flexor retinaculum near the pisiform bone, mainly supplying blood to the palm and fingers [1-3].
One of its main roles is forming the superficial palmar arch, an arterial network located above the flexor tendons and below the palmar aponeurosis. The superficial palmar arch can vary greatly in structure and completeness. It usually forms mostly from the ulnar artery, supplemented by a branch from the radial artery. However, there are cases where the arch is entirely made by the ulnar artery, or it may be incomplete. Sometimes, the median artery or other branches contribute as well [1,3,4]. These variations are categorized by completeness and the source of arterial supply, which is important for surgical planning to avoid unintended damage to blood vessels [5].
Nearby are the median and ulnar nerves, which provide movement and sensation to the hand. Both nerves create palmar digital branches and have connections between them known as neural anastomoses. The patterns and frequency of these connections differ widely, showing the complex wiring of the hand [6].
Several types of anastomoses between the median and ulnar nerves exist, including the Berrettini anastomosis, the Riché-Cannieu anastomosis, and the Martin-Gruber anastomosis. The Berrettini anastomosis is the most common palmar neural connection. It forms between the common palmar digital nerves of the ulnar and median nerves, usually found between the third and fourth digits [7,8]. The Riché-Cannieu anastomosis connects the recurrent branch of the median nerve with the deep branch of the ulnar nerve in the thenar muscles, impacting motor control [2,9]. The Martin-Gruber anastomosis connects the median and ulnar nerves in the proximal forearm, affecting motor fibers before they reach the hand [10].
Understanding these anastomoses is crucial because they affect sensory and motor functions, complicate nerve conduction studies, and can lead to unexpected clinical issues during neuropathies or surgeries. The Berrettini anastomosis, in particular, shows variation in its form and frequency and has been grouped by the direction, number, and complexity of its connections [11]. This study examines the detailed anatomical features and variations of the Berrettini anastomosis, along with the vascular structures of the ulnar artery and the superficial palmar arch, to enhance clinical and surgical knowledge.
Materials and methods
This was an anatomical study using cadavers. The cadavers were obtained from the anatomical dissection hall of the Institute of Anatomy, School of Medicine, University of Belgrade, Serbia, and Department of Anatomy, School of Medicine, University of St Andrews. A total of 36 embalmed cadaveric upper limbs (18 right and 18 left) were used in this study.
Dissection process
First, a visual inspection of each limb was performed to exclude specimens with deformities and traces of trauma or surgery. After fixation in formalin solution, the extremities were carefully dissected, following standard procedures from dissection manuals. The limbs were placed in a supine position with the palm facing upward.
A longitudinal skin incision was made from the distal forearm to the middle of the palm. Skin and subcutaneous tissue were carefully reflected to expose the palmar aponeurosis. The palmar aponeurosis was incised and reflected to reveal the median and ulnar nerves and their common digital branches. The area between the third and fourth common digital nerves was closely examined. Any communicating branches between the median and ulnar nerves were noted. The origin, course, and termination of the anastomotic branch were traced and documented.
After identification of the median and ulnar nerves, we located the ulnar artery as it enters the palm, superficial to the flexor retinaculum (transverse carpal ligament), often just lateral to the pisiform bone. We traced the ulnar artery distally as it curves laterally across the palm, typically forming the superficial palmar arch, and identified contributions from the radial artery or occasionally the median artery joining to complete the arch. After identification of the SPA, we carefully cleared the connective tissue around the arch to fully expose its arc shape and preserved and noted the common digital palmar (CDP) arteries branching off the arch, supplying the fingers.
Kaplan’s line is an important anatomical landmark used in hand surgery and clinical anatomy to help localize structures on the palmar surface of the hand. It is an imaginary transverse line drawn across the palm, extending from the apex of the first interdigital space (the cleft between the thumb and index finger) toward the hook of the hamate bone on the ulnar side. It typically lies proximal to the distal palmar crease. Kaplan’s line serves as a guide to the safe zone during surgical approaches to the palm, particularly in procedures involving the carpal tunnel and the superficial palmar arch. In our study, after identification of the 1st-4th CDA, we measured its distance from Kaplan’s line [12,13] and statistically examined differences between male and female cadavers.
Statistical analysis
All statistical measurements were done in SPSS Statistics for Windows, version 11.0 (Released 2002; SPSS Inc., Chicago, Illinois, United States) using the t-test. p<0.05 was considered statistically significant.
Results
We analyzed 36 cadaveric hands (20 female, 16 male) to assess variations in the SPA and the distribution of CDP arteries (Figures 1-3). Among the hands, 16 (44.4%) demonstrated incomplete SPAs, and 20 (55.6%) showed complete SPAs. A sex-specific distribution was noted: 12 of the 16 incomplete types were from female specimens, while four were from male specimens. Conversely, 12 of the 20 complete arches were from male specimens, with the remaining eight from female specimens. Thus, incomplete types were more prevalent among female specimens, while complete types were more common in males.
Methodology of examined parametersKaplan‘s line is presented with a black, bolded line. Numbers 1-4 are CDP arteries, while the arrows show the distance between Kaplan’s line and the origin of the CDP artery from the superficial palmar arch.CDP: common digital palmarDissection done by: Dr. Slobodan Kapor
Dissection view of superficial palmar arch (complete type), as well as common palmar digital arteries and common digital palmar nerves with Berrettini anastomosis (type III)UA: ulnar artery; MN: median nerve; UN: ulnar nerve; spa: superficial palmar arch; cb: common bidirectional branch; 1-4: common digital palmar arteries ; I-IV: common digital palmar nervesDissection done by: Dr. Slobodan Kapor.
Dissection view of superficial palmar arch (complete type), as well as CDP arteries and CDP nerves with no Berrettini anastomosisMedian nerve innervates I – III fingers, while ulnar nerve is responsible for innervation of last two fingers (IV-V).UA: ulnar artery; MN: median nerve; UN: ulnar nerve; spa: superficial palmar arch; CDP: common digital palmarDissection done by: Dr. Slobodan Kapor.
Distance from Kaplan’s line to CDP arteries
Measurements (in cm) from Kaplan’s line to the first through the fourth CDP arteries are presented in Table 1 and were significantly greater in male specimens than in female specimens (p < 0.05 for all comparisons).
Table 1: Measurements of the distance between the Kaplan‘s line and 1-4 CDP arteries*statistically significant value (p< 0.05)CDP: common digital palmar
Berrettini anastomosis
The Berrettini anastomosis, a communicating neural branch between the median and ulnar nerves, was identified in 12 out of 36 hands (33.3%). We defined three types of communication between median and ulnar nerves: type I (ulnar to median); type II (median to ulnar); type III (multiple or bidirectional connections). These results are presented in Table 2.
Discussion
This study investigated anatomical variations of the SPA, distances from Kaplan’s line to the CDP arteries, and the occurrence of the Berrettini anastomosis in 36 cadaveric hands. Our findings contribute valuable data on hand anatomy with potential clinical implications.
The prevalence of complete (55.6%) and incomplete (44.4%) SPAs in our sample aligns with previous literature, which reports SPA completeness rates ranging from 40% to 90% depending on the population studied and methodology used [13-19]. Some researchers observed complete arches in about 52.2% of hands, with 47.8% being incomplete [12], while Rodriguez-Niedenfuhr and colleagues reported complete SPAs in 50-60% of adult specimens [20].
The sex-related difference observed, with incomplete SPAs more common in females and complete SPAs more prevalent in males, has been reported less frequently [1,2,5,19,20], but was also noted by Tubbs et al. [7,8] as well as Zarzecki et al. [21], suggesting sexual dimorphism in hand vascular anatomy. This variation is important for surgical planning, as incomplete arches may increase the risk of ischemic complications during hand surgery, particularly in females.
Our data revealed significantly greater distances from Kaplan’s line to the CDP arteries in male specimens compared to female specimens (p < 0.05 for all arteries). This finding confirms previously described sexual dimorphism in hand anatomy, including vascular and neural structures [14]. Kaplan’s line remains a crucial landmark for surgeons to avoid vascular injury during procedures such as carpal tunnel release and digital artery dissection [12]. Although previous studies have measured distances of arterial branches in the palm, data specific to Kaplan’s line distances and sex differences are limited, underscoring the novelty and clinical relevance of our results [12,16-18].
Berrettini anastomosis was present in 33.3% of hands, consistent with prior studies reporting a prevalence between 20% and 70% [1,11,22]. The predominance of Type III anastomoses (66.7%) in our sample concurs with Zolin et al.'s classification, which highlights the frequent presence of multiple or bidirectional communications [10]. The absence of Type I (ulnar- to- median) connections in our sample may be due to population variation or sample size limitations. These neural connections have important clinical implications since they may affect sensory innervation patterns and complicate the diagnosis and treatment of median and ulnar nerve pathologies [15,16].
Knowledge of these variations is essential for surgeons performing nerve decompression or repair in the hand to avoid inadvertent injury. The study was limited by a modest sample size of 36 cadaveric hands and lacked ethnic diversity, which may limit the generalizability of findings. Future investigations combining anatomical, imaging, and electrophysiological techniques in larger, diverse populations would provide deeper insight into the functional significance of these anatomical variations.
Conclusions
Our findings highlight clinically significant variations in hand neurovascular anatomy, with notable sex-based differences in SPA configuration and arterial topography. The frequent occurrence of complex Berrettini anastomoses underscores the importance of detailed anatomical awareness to avoid complications in hand surgeries and enhance diagnostic procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A morphometric study on the superficial palmar arch of the hand Surg Radiol Anat Bilge O Pinar Y Ozer MA Gövsa F 3433502820061664228110.1007/s 00276-006-0109-9 · doi ↗ · pubmed ↗
- 2Communications between the palmar digital branches of the median and ulnar nerves: a study in human fetuses and a review of the literature Clin Anat Unver Dogan N Uysal II Karabulut AK Seker M Ziylan T 2342412320102001439710.1002/ca.20906 · doi ↗ · pubmed ↗
- 3Gray’s Anatomy: The Anatomical Basis of Clinical Practice Standring S Gray H Anand N Tunstall R Amsterdam, Netherlands Elsevier 2021 https://archive.org/details/graysanatomyanat 0000 unse_c 5d 4/page/n 1583/mode/2up
- 4Moore's Clinically Oriented Anatomy Moore KL Dalley AF Agur AM Philadelphia, PA Wolters Kluwer 2023 https://search.worldcat.org/title/1260173449
- 5Variations in superficial palmar arch: case series with clinico-anatomical perspective Medeni Med J Borthakur D Kumar R Singh S 3463513720223657816910.4274/MMJ.galenos.2022.82598 PMC 9808850 · doi ↗ · pubmed ↗
- 6Arterial patterns in the hand based upon a study of 650 specimens Surg Gynecol Obstet Coleman SS Anson BJ 4094241131961 https://pubmed.ncbi.nlm.nih.gov/13694610/13694610 · pubmed ↗
- 7Anatomical landmarks to the superficial and deep palmar arches Plast Reconstr Surg Tubbs RS Shoja MM Loukas M 129212220081882767910.1097/PRS.0b 013e 3181845 a 46 · doi ↗ · pubmed ↗
- 8Bergman's Comprehensive Encyclopedia of Human Anatomic Variation Tubbs RS Shoja MM Loukas M Hoboken, NJ John Wiley & Sons, Inc 2016 https://onlinelibrary.wiley.com/doi/book/10.1002/9781118430309