Digital Infrastructure for Antimicrobial Susceptibility Testing and Surveillance: A CLSI and EUCAST-Based Model for Resource-Limited Settings
Djibril Mbarushimana, Taofeek Tope Adegboyega, Gatera Jean Damascene, Muritala Issa Bale, Buregeya Jean Damascene, Kayitesi Marie Francoise, Itangishaka Innocent, Rugamba Alexis, Rasheed Omotayo Adeyemo, Bagirinshuti Issa, Saheed Adekunle Akinola, Ahmed Adebowale Adedeji

TL;DR
This paper presents a digital system for antimicrobial testing in Rwanda, improving data accuracy and real-time surveillance in resource-limited settings.
Contribution
A scalable, web-based LIS model integrating CLSI and EUCAST standards for AMR surveillance in low-resource environments.
Findings
The enhanced LIS improved AST data capture and standardization at CHUB.
The system enables real-time AMR surveillance and integrates with electronic medical records.
The model supports scalability and metadata consistency across multiple facilities.
Abstract
Antimicrobial resistance (AMR) poses a significant global health threat, requiring effective antimicrobial susceptibility testing (AST) and surveillance systems. At the University Teaching Hospital of Butare (CHUB) in Rwanda, a baseline Laboratory Assessment of Antibiotic Resistance Testing Capacity (LAARC) identified critical gaps in the Laboratory Information System (LIS), including low capture rates for culture observation (60%) and AST data (25%), no standardization of AST panels (0%), and limited cumulative antibiogram generation (17%). Existing AMR surveillance platforms, such as the Information System for Monitoring Antimicrobial Resistance by the World Health Organization (WHO) Collaborating Center for Surveillance of Resistance to Antimicrobial Agents (WHONET), and the District Health Information System, operate as standalone systems separate from clinical workflows, which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
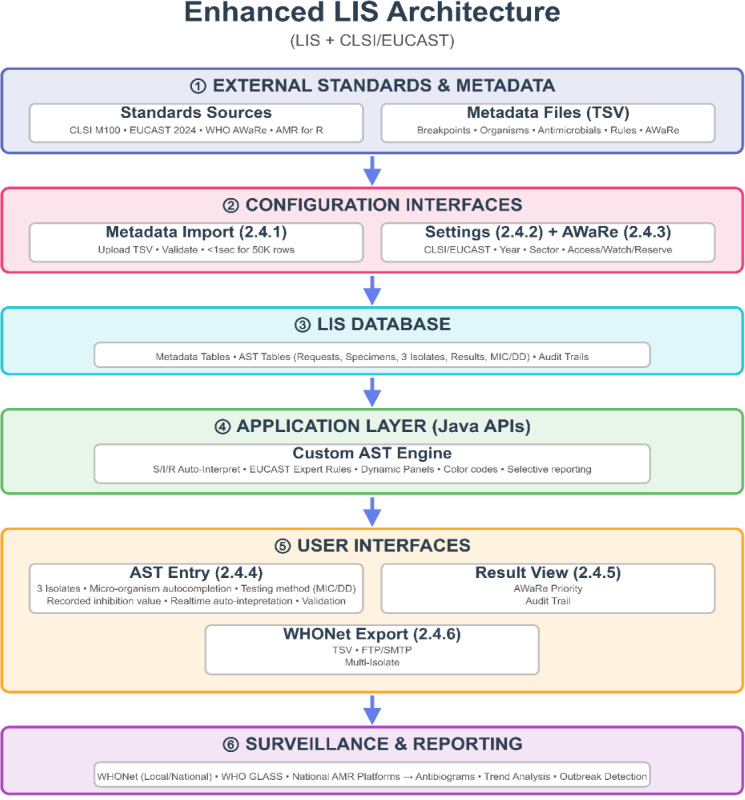 Figure 1
Figure 1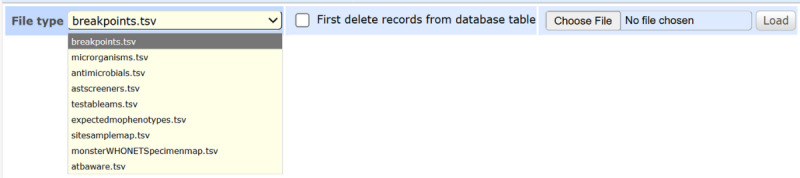 Figure 2
Figure 2 Figure 3
Figure 3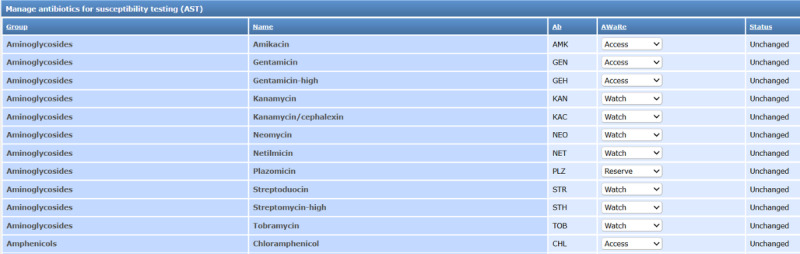 Figure 4
Figure 4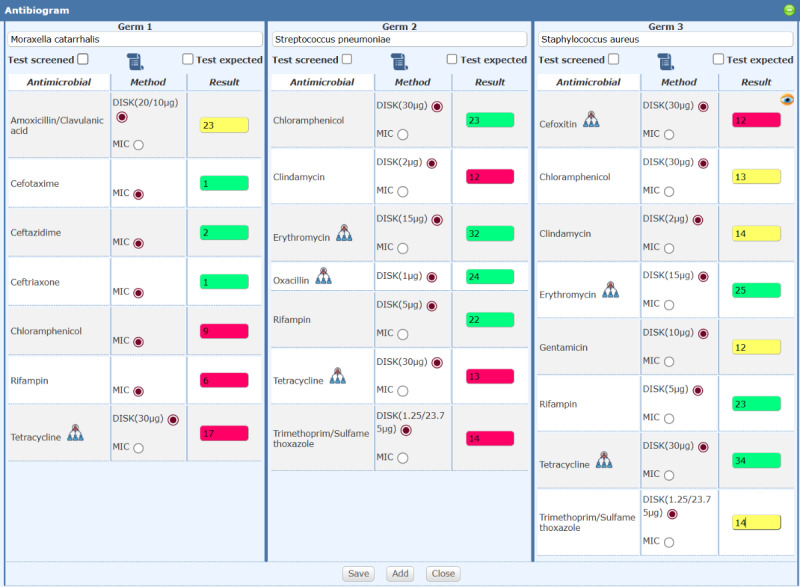 Figure 5
Figure 5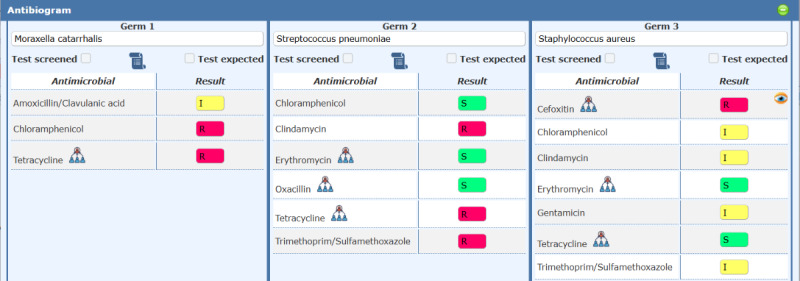 Figure 6
Figure 6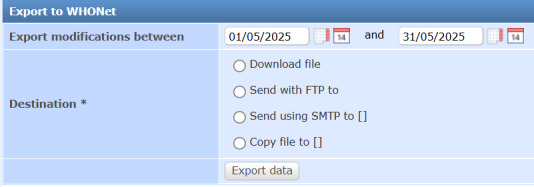 Figure 7
Figure 7| Deficiency | Impact |
|---|---|
| Does not record AST | Hinders traceability of test methods |
| Cannot hide individual antibiotic results | Prevents cascade/selective reporting [ |
| Only Susceptible, Intermediate, or Resistant (S/I/R) interpretations entered | Limits data granularity for analysis |
| Lacks automated interpretation | Manual processes, increasing error risk |
| EUCAST | Limits clinical decision support |
| Inconsistent antibiotic panels | Results in data unsuitable for reliable cumulative antibiogram generation |
| Original results deleted during corrections | Compromises audit trails |
| File content | Purpose | Key fields |
|---|---|---|
| Clinical breakpoints | Stores CLSI/EUCAST | Guideline, test method, pathogen, antimicrobial, breakpoint values |
| Microorganisms | Provides taxonomic and characteristic data for microbial identification | Pathogen identifier, kingdom, genus, species, prevalence, clinical codes (SNOMED |
| Antimicrobials | Details antimicrobial agents with Access, Watch, Reserve (AWaRe) classifications | Antibiotic name, class, potency, administration routes, standardized codes (WHONET |
| Antimicrobial screening rules | Defines screening rules for specific pathogens | Antimicrobial, target pathogen, screening criteria |
| Testable Antimicrobials | Lists antimicrobials with standardized AST | Group, name, abbreviation, AWaRe classification |
| Expected Phenotypes | Incorporates EUCAST Expert Rules for expected phenotypes | Antimicrobial, pathogen, phenotype (susceptible/resistant) |
| Site-Sample Mapping | Maps clinical sites to sample types | Site, specimen type (eg, Respiratory → Sputum) |
| WHONET Specimen Mapping | Standardizes specimen codes for WHONET interoperability | Local codes, WHONET specimen type codes |
| AWaRe Classification | Classifies antibiotics into AWaRe categories | Antibiotic name, AWaRe category |
| LAARC deficiency | Status | Evidence and notes |
|---|---|---|
| Does not record AST method | Fully Resolved | Captures MIC/DD methods in the AST Result Entry Interface (Section 2.4.4) and includes them in WHONET exports (Section 2.4.5). |
| Cannot suppress antibiotic results for cascade reporting | Fully Resolved | AST Result View Form (Section 2.4.6) implements AWaRe-based cascade reporting. |
| Only S/I/R entered, not inhibition zone | Fully Resolved | AST Result Entry Interface (Section 2.4.4) captures inhibition zones/MIC values with automated S/I/R interpretation. |
| Cannot automatically interpret zone sizes | Fully Resolved | Automates S/I/R interpretation using CLSI/EUCAST breakpoints (Section 2.4.4). |
| Expert rules not integrated | Fully Resolved | Integrates EUCAST Expert Rules for phenotypic predictions (Sections 2.3, 2.4.4, 2.4.6). |
| Inconsistent antibiotic panels | Fully Resolved | Achieves 100% panel standardization (Section 3) via metadata-driven panels (Section 2.3) and AWaRe Classification Management Interface (Section 2.4.3). |
| Original results deleted during corrections | Fully Resolved | Tracks corrections via edit history icons in the AST Result View Form (Section 2.4.6), logging edited results with timestamps, reason and user details. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Bacterial Identification and Susceptibility Testing · Electronic Health Records Systems
Introduction
Antimicrobial Resistance (AMR) Surveillance Challenges in Resource-Limited Settings
Antimicrobial Resistance (AMR) is a global health emergency, with the World Health Organization (WHO) estimating 10 million annual deaths by 2050 if unchecked [1]. Effective antimicrobial susceptibility testing (AST) and robust surveillance systems are fundamental to combating AMR. AST guides appropriate therapy at the patient level, while surveillance aggregates resistance data to monitor trends and inform evidence-based treatment guidelines [23]. Resource-limited settings, particularly in Sub-Saharan Africa, face significant barriers to implementing reliable AST and surveillance infrastructure, including inadequate laboratory information systems, inconsistent adoption of standardized guidelines (Clinical and Laboratory Standards Institute [CLSI] and European Committee on Antimicrobial Susceptibility Testing [EUCAST]),[4] limited access to quality-assured testing protocols, and fragmented data management that impairs interoperability with national and global surveillance networks [5-8], undermine antimicrobial stewardship efforts and exacerbate AMR.
Baseline Deficiencies at the University Teaching Hospital of Butare
The University Teaching Hospital of Butare (CHUB), a tertiary referral center in Rwanda, exemplifies these challenges. CHUB’s LIS (Laboratory Information System), built on the OpenClinic GA open-source hospital information system [9], exhibited critical deficiencies in microbiology services. A baseline Laboratory Assessment of Antibiotic Resistance Testing Capacity (LAARC) [10], identified critical deficiencies: 60% capture rate for culture observation, 25% for AST data, 0% standardization of AST panels, and 17% generation of cumulative antibiograms, reflecting systemic issues in resource-limited settings. The assessment revealed several qualitative deficiencies in the LIS that compromised bacteriology services at CHUB (Table 1) [11], which reflect systemic issues, where LIS platforms lack specialized microbiology functionality necessary for standards-compliant AST and surveillance.
Study Rationale and Objectives
Addressing the revealed gaps requires an enhanced LIS that integrates international AST standards, automates result interpretation, standardizes testing panels, and enables seamless data export to surveillance networks. This study aimed to develop such a system at CHUB leveraging the OpenClinic GA platform and integrating CLSI and EUCAST guidelines [23], incorporating metadata from the AMR for R package [13], and from the Information System for Monitoring Antimicrobial Resistance by World Health Organization (WHO) Collaborating Center for Surveillance of Resistance to Antimicrobial Agents (WHONET) [61415], as well as EUCAST Expert Rules and expected phenotypes [16].
The enhanced LIS was designed to resolve all LAARC-identified deficiencies, standardize AST processes, enable real-time AMR surveillance, and facilitate data interoperability with the WHO Global Antimicrobial Resistance Surveillance System (GLASS) and national platforms. By building on OpenClinic GA’s established infrastructure, the system provides a scalable, open-source model tailored to resource-limited settings, improving data quality, supporting evidence-based antimicrobial stewardship, and contributing to global AMR monitoring efforts. This approach offers a replicable blueprint for tertiary hospitals and reference laboratories in Sub-Saharan Africa and similar contexts, demonstrating how standards-based digital infrastructure can address critical surveillance gaps with minimal resource requirements and sustainable, locally adaptable solutions.
Methods
Study Design and Setting
This technical implementation study was conducted at CHUB, a key microbiology center in Rwanda, from January 2024 to June 2025. The study focused on upgrading the CHUB LIS, built on the OpenClinic GA open-source hospital information system [9], to address LAARC-identified deficiencies, leveraging metadata from the AMR for the R package and EUCAST Expert Rules.
System Development Approach
An agile methodology facilitated iterative development, incorporating feedback from laboratory staff, clinicians, and public health experts. Requirements targeted improved data capture, AST panel standardization, antibiogram generation, and interoperability with global surveillance systems, extending the capabilities of the OpenClinic GA platform. The agile approach was chosen based on its proven effectiveness in developing health information systems in low-resource settings [1718].
Data Analysis and Metadata Integration
Metadata from the AMR for R package, including microbial taxonomy, antimicrobial profiles, and clinical breakpoints, were analyzed to standardize AST processes. EUCAST Expert Rules and expected phenotypes guided automated interpretations and dynamic testing panel generation. Nine metadata files, all in tab separated values (TSV) format, were integrated, each mapped to specific database tables within the OpenClinic GA system (Table 2).
System Architecture and Functionalities
The LIS was developed by extending the OpenClinic GA open-source web-based hospital information system, incorporating a custom database schema, Java-based APIs, and a web-based interface, optimized for resource-limited settings. The system comprises five key user interfaces, each designed for usability and compliance with CLSI, EUCAST, and WHO GLASS standards (Figure 1).
High-level schematic representation of the enhanced LIS architecture and end-to-end data flow. Circled numbers (①-⑥) denote the six architectural layers of the system. Numbers in parentheses refer to subsections in section 2.4 (system architecture and functionalities) where detailed technical descriptions are provided. AST: antimicrobial susceptibility testing; API: application programming interface; AWaRe: Access, Watch, Reserve; CLSI: Clinical and Laboratory Standards Institute; DD: disk diffusion; EUCAST: European Committee on Antimicrobial Susceptibility Testing; LIS: Laboratory Information System; MIC: Minimum Inhibitory Concentration; TSV: Tab Separated Values; WHONET: World Health Organization Collaborating Center for Surveillance of Resistance to Antimicrobial Agents.
Metadata Import Interface
A web-based tool simplifies the import and update of metadata files within the OpenClinic GA. Users select a file type from a dropdown menu, upload TSV files, and optionally clear existing data. The system validates file headers, provides real-time feedback on errors (eg, invalid format), and deletes temporary files to optimize storage. This interface leverages OpenClinic GA’s robust file-handling capabilities to ensure efficient data management by enabling nontechnical users to update metadata with minimal training (Figure 2).
Screenshot of the metadata import interface, showing the dropdown menu for selecting file types, the file upload button, and the feedback panel for validation status.
Configuration Interface
A web-based tool allows users to configure the AST guideline (EUCAST/CLSI), guideline year, and sector (human or animal) to adapt the system to local needs (Figure 3).
Screenshot of the configuration interface, displaying dropdown menus for selecting AST guideline (CLSI/EUCAST), guideline year, and sector (human/animal), with multilingual support options. AST: antimicrobial susceptibility testing; CLSI: Clinical and Laboratory Standards Institute; EUCAST: European Committee on Antimicrobial Susceptibility Testing.
AWaRe Classification Management Interface
A dedicated tool manages the AWaRe classification of testable antibiotics. It displays a sortable table of antibiotics with their group, name, abbreviation, and AWaRe status or Not Available. Users update classifications via dropdown menus, with changes tracked client-side using JavaScript and submitted asynchronously to the server for database updates (Figure 4).
Screenshot of the AWaRe classification management interface, showing a sortable table of antibiotics with dropdown menus for updating AWaRe status and real-time feedback indicators. AST: antimicrobial susceptibility testing; AWaRe: Access, Watch, Reserve.
AST Result Entry Interface
Integrated into worklist management, this modal dialog supports manual entry and validation for up to three isolates per specimen, aligning with CLSI/EUCAST recommendations. Key features include: standardized pathogen identification via WHONET/EUCAST/CLSI taxonomy with autocompletion; dynamic antibiotic panels that expand based on whether to include screened antibiotics and/or those with expected phenotypes; real-time color-coded validation (green=Susceptible, yellow=Intermediate, red=Resistant) for inhibition zones or MIC values; icons indicating related antimicrobials and administration-route-dependent interpretations; alerts for invalid inputs, and incomplete method specification (Figure 5).
Screenshot of the AST result entry interface, showing the modal dialog with isolate panels, dynamic antimicrobial table, color-coded result fields, and autocompletion for pathogen identification. MIC: minimum inhibitory concentration.
AST Result View Form
Integrated into laboratory results view, this interface displays finalized AST results for clinicians, infection control staff, and surveillance teams, aligning with CLSI, EUCAST guidelines [1222-24undefinedundefined]. Results appear in modal dialogs grouped by patient and request time, showing up to three isolates with organism names, antimicrobials, S/I/R interpretations, and phenotype indicators. AWaRe–based selective display prioritizes Access antibiotics when susceptible or intermediate, then Watch, then Reserve. Read-only format ensures data integrity; edit history icons track corrections with timestamps and user details. Any pathogen isolated triggers red danger icons in the laboratory results overview that corresponds to automated SMS notifications at result validation sent to the patient informing result availability and to the requesting clinician alerting to urgently review results and take clinical action (Figure 6).
Screenshot of the AST result view form, showing the modal dialog with a grouped results table, color-coded isolate data, AWaRe-filtered antibiotic display, and tooltips for phenotypic comments. AST: antimicrobial susceptibility testing; AWaRe: Access, Watch, Reserve.
WHONET Export Interface
This interface enables seamless export of AST results to WHONET for global AMR surveillance, complying with WHONET’s data formatting requirements. A web form with calendar widgets allows date range selection and export destination choice (download, FTP, SMTP, or directory). The system queries finalized AST records within the selected range, supporting multi-isolate reporting with patient demographics (ID, sex, age, WHO/CLSI age categories), specimen type (WHONET-mapped), pathogen identification, test method, antimicrobial codes, result values, S/I/R interpretations, guideline, sector, and workflow timestamps. Output generates TSV files matching WHONET import specifications, with legacy CSV support (Figure 7) [2526].
Screenshot of the WHONET export interface, displaying the web form with calendar widgets for date range selection, a dropdown for export destination, and feedback on export status. WHONET: World Health Organization Collaborating Center for Surveillance of Resistance to Antimicrobial Agents.
Ease of Integration and Interoperability
The enhanced LIS incorporates interoperability features tailored for resource-limited settings, supporting structured data formats (TSV, CSV, JSON, HL7, FHIR) for direct mapping of organism codes, test results, and interpretations. Plug-and-play API endpoints enable the LIS to integrate with other systems with minimal development effort. Direct export to WHONET, WHO GLASS, and national platforms includes automated local-to-surveillance code mapping.
User Verification, Training and Deployment
Structured user verification and training were conducted before hospital-wide go-live. A dedicated User Acceptance testing was carried out by a team composed of the Laboratory Quality Manager, Microbiology Section Lead, and Information Communication Technology (ICT) staff under the supervision of the Head of Pathology. Nineteen detailed test cases covering system configuration, metadata import, AST result entry (disk diffusion and MIC), dynamic panel generation, EUCAST Expert Rules application, AWaRe–based cascade reporting, audit trails, WHONET export, data integrity, performance, and multilingual support were executed on 10 prospective samples, as per the laboratory standard operating procedure on user verification of LIS. All 19 test cases passed (100 % pass rate). Minor adjustments, mainly related to character encoding compatibility, were applied iteratively.
The six bacteriology laboratory staff received a full day of hands-on training. A 30-minute hospital-wide flash presentation of the new AST reporting features was delivered during clinical grand rounds, and finally, a 5-minute video tutorial covering the entire workflow was produced and disseminated via the hospital’s official WhatsApp groups
The enhanced AST module fully replaced the legacy entry workflow for all new microbiology requests. For backward compatibility and data integrity, the previous (legacy) AST entry and viewing functionality was not removed or disabled. All AST results entered before enhancement remain fully accessible, searchable, and viewable in their original format without any modification or migration issues.
Ethical Considerations
The project received ethical approval from the CHUB Research-Ethics Committee (REC/UTHB/91/2023 renew, October 20th, 2024); individual informed consent was waived as the study was a quality-improvement intervention using routine clinical data. Patient confidentiality and data protection fully comply with hospital policy through role-based user authentication, display of patient identifiers and clinical information only to authorized clinical users, secure hosting within the hospital’s firewalled data center with twice daily backups, and complete removal of identifiers from all shared data and aggregate datasets.
Results
The enhanced LIS, built on OpenClinic GA, significantly improved CHUB’s bacteriology services, addressing LAARC-identified deficiencies (Multimedia Appendix 1). The system resolved qualitative gaps identified in the baseline LAARC audit, as detailed below.
Resolution of Qualitative Deficiencies
The enhanced LIS addressed the qualitative deficiencies identified in the LAARC audit (Section 1.4), all fully resolved. The following Table 3 summarizes the resolution status, referencing relevant system functionalities:
Key Functionalities
The system offers comprehensive AST functionality supporting both MIC and DD methods with automated interpretation based on the selected guideline. Results are displayed using color-coded outputs: green for Susceptible, yellow for Intermediate, red for Resistant, and pink for out-of-range values. The system provides real-time notifications for critical isolates to ensure timely clinical intervention.
Dynamic testing panels automatically adjust based on breakpoints, local antimicrobial stock availability, and clinical context, incorporating EUCAST Expert Rules and expected phenotypes. The cascade reporting feature prioritizes WHO AWaRe “Access” antibiotics, thereby reducing inappropriate use of “Watch” and “Reserve” categories.
For surveillance purposes, data export aligns with WHONET variable definitions, enabling seamless integration with WHO GLASS and national surveillance systems through robust interoperability features. The web-based interfaces, including the AST Result View Form, require minimal training and incorporate real-time feedback and tooltips to enhance usability for nontechnical staff.
Discussion
The enhanced LIS, built upon the OpenClinic GA open-source hospital information system, addresses critical gaps in CHUB’s microbiology services, offering a robust, standards-compliant solution for AST and surveillance in resource-limited settings. By integrating CLSI and EUCAST guidelines with metadata from the AMR for R package and EUCAST Expert Rules, the system ensures reliable AST results and real-time surveillance capabilities. The agile development approach, coupled with stakeholder engagement, resulted in a user-friendly system accessible to laboratory staff with minimal technical expertise.
The metadata-driven design, particularly the use of WHO AWaRe classifications and EUCAST Expert Rules, optimizes antimicrobial testing and supports stewardship by prioritizing “Access” antibiotics and flagging critical resistance mechanisms. The WHONET export interface enhances interoperability with global surveillance networks, contributing to AMR monitoring and policy development [1].
Comparison With Existing AMR Surveillance Platforms
The enhanced LIS offers distinct advantages over other popular AMR surveillance platforms by providing comprehensive, integrated laboratory workflow management within a clinical care context. Unlike WHONET, which operates as a standalone desktop on Windows environments and focuses exclusively on bacteriology data [2728], the enhanced LIS is fully web-based, supports comprehensive clinical laboratory operations across all departments (hematology, biochemistry, immunology, microbiology) and accessible from any device with a standard browser, enabling real-time data entry, validation, and clinical decision support at the point of care. Integrated within the electronic medical record system, the enhanced LIS maintains continuity of clinical information flow from specimen registration through result reporting, directly supporting antimicrobial stewardship through features such as AWaRe-based cascade reporting, automated resistance phenotype detection via EUCAST Expert Rules, and critical alerts that prompt immediate clinical review. While District Health Information System (DHIS2) excels at aggregate health program reporting across multiple domains [2930], the enhanced LIS provides specimen-level granularity essential for individual patient management, combining automated CLSI/EUCAST-based AST interpretation and quality-assured data validation within a single platform. This integrated approach ensures data serves dual purposes: immediate clinical utility for patient care and antimicrobial stewardship at the facility level, followed by standardized WHONET-compatible exports for public health surveillance at subnational, national, and global levels [615]. By embedding AMR surveillance capabilities within routine clinical workflows rather than treating surveillance as a separate downstream activity, the enhanced LIS maximizes data quality, clinical relevance, and public health impact while minimizing the burden on laboratory staff.
Scalability to Subnational and National AMR Surveillance Networks
The web-based architecture of the enhanced LIS provides inherent scalability for subnational and national AMR surveillance networks through centralized deployment models. The system can be hosted on centralized servers, enabling simultaneous access by multiple testing facilities through standard web browsers without requiring local software installation or high-specification hardware at peripheral sites. This approach ensures real-time data visibility across the network: facility-level users enter AST results through the web interface, while supervisory-level surveillance teams access aggregated data from the same system. From any supervisory level, the WHONET export interface generates standardized data files compliant with WHO GLASS requirements, enabling seamless reporting to global surveillance networks. The centralized model eliminates data fragmentation common in resource-limited settings, reduces infrastructure costs by avoiding multiple server deployments, and ensures metadata consistency (breakpoints, antimicrobial panels, AWaRe classifications) across all participating facilities.
Sustainability Considerations
Long-term sustainability of the enhanced LIS requires attention to three critical areas. First, continuous user training programs must be established to maintain laboratory staff competency in system use, AST interpretation, and data quality assurance. Second, metadata updates require sustainable mechanisms, including periodic review of CLSI/EUCAST guideline updates, AMR for R package datasets, WHONET resources and taxonomies, local antimicrobial availability changes, and emerging resistance patterns, with designated personnel responsible for metadata maintenance and validation. Third, ongoing technical support requires a multifaceted approach: capacity building for local information technology staff to handle routine troubleshooting, system upgrades, and eventually instrument integration; and sustainable funding mechanisms beyond donor-dependent models to ensure long-term system functionality and relevance.
Limitations and Future Directions
This study primarily describes the technical development and the qualitative resolution of LIS deficiencies identified in the baseline LAARC audit. Quantitative evaluation of key performance indicators was intentionally deferred to allow sufficient post-implementation observation time. Additional limitations include dependency on manual metadata updates and import, which may be challenging in resource-limited settings. Ongoing training is required to sustain system adoption and ensure data quality. Future enhancements could include automatic metadata updates, mobile app integration, and machine learning for predictive resistance modeling, which have shown promise in other AMR surveillance systems [233132].
Conclusion
The enhanced LIS, built on OpenClinic GA and leveraging CLSI, EUCAST, and AMR for R metadata, demonstrates the feasibility of implementing standards-based AMR informatics in resource-limited settings. By significantly improving AST reliability, integrating clinical decision support, and enabling seamless integration with global surveillance networks, this model provides a practical roadmap for national digital stewardship programs. The system’s scalability from facility to national levels, combined with its open-source foundation and standards-compliant architecture, offers a replicable blueprint for addressing AMR challenges, supporting both immediate patient care and long-term public health surveillance goals. Widespread adoption of such standards-based digital surveillance systems could significantly contribute to reducing AMR burden through earlier detection of resistance trends and evidence-based policy interventions.
Supplementary material
10.2196/82727Multimedia Appendix 1Demo of new AST (antimicrobial susceptibility testing) reporting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antimicrobial resistance: global report on surveillance World Health Organization 2014 UR Lhttps://iris.who.int/handle/10665/112642 Accessed 04-08-2025
- 2EUCAST: Clinical breakpoints and dosing of antibiotics UR Lhttps://www.eucast.org/clinical_breakpoints Accessed 04-08-2025
- 3EM 100 Connect - CLSI M 100 ED 35:2025 UR Lhttps://em 100.edaptivedocs.net/Get Doc.aspx?doc=CLSI%20M 100%20ED 35:2025&scope=user Accessed 04-08-2025
- 4Clinical & Laboratory Standards Institute: CLSI Guidelines UR Lhttps://clsi.org/Accessed 22-08-2024
- 5Turner P Rupali P Opintan JA et al Laboratory informatics capacity for effective antimicrobial resistance surveillance in resource-limited settings Lancet Infect Dis Jun 2021216 e 170e 174doi 10.1016/S 1473-3099(20)30835-5Medline 33865461 · doi ↗ · pubmed ↗
- 6Global antimicrobial resistance and use surveillance system (GLASS)WHOUR Lhttps://www.who.int/initiatives/glass Accessed 04-08-2025
- 7Tools of the trade: data management software in AMR surveillance Fleming Fund UR Lhttps://www.flemingfund.org/publications/tools-of-the-trade-data-management-software-in-amr-surveillance/Accessed 04-08-2025
- 8Aboushady AT Sujan MJ Pham K et al Key Recommendations for Antimicrobial Resistance Surveillance: Takeaways From the CAPTURA Project Clin Infect Dis Dec 20202377 Suppl 7S 581S 587doi 10.1093/cid/ciad 487Medline 38118016 PMC 10732552 · doi ↗ · pubmed ↗