Safety and Synergy of Capmatinib Plus Stereotactic Radiotherapy in MET Exon 14-Mutated Non-Small Cell Lung Cancer: A Case Report
Othmane Bensalah, Meryem Naciri, Mohamed Ali Boudraa, Fatimaezzahra Aouzah, Fadila Kouhen

TL;DR
A patient with a rare lung cancer mutation responded well to a combination of a MET inhibitor and targeted radiation therapy, showing safety and effectiveness.
Contribution
This case report demonstrates the safe and synergistic use of capmatinib and SBRT in MET exon 14-mutated NSCLC.
Findings
The combination of capmatinib and SBRT achieved durable tumor regression with no significant toxicity.
The patient showed complete resolution of a brain lesion and control of oligoprogression.
Temporary capmatinib suspension during SBRT improved tolerability and outcomes.
Abstract
MET exon 14 skipping mutations define a rare subset of non-small cell lung cancer (NSCLC). Capmatinib, a selective MET inhibitor, has shown efficacy, but oligometastatic lesions often require local therapy. Data on combining capmatinib with stereotactic body radiotherapy (SBRT) remain limited. A 73-year-old man with well-controlled type 2 diabetes and a history of smoking presented with a right upper lobe mass, mediastinal lymphadenopathy, vertebral metastases, and a small brain lesion. Biopsy confirmed adenocarcinoma (thyroid transcription factor-1 (TTF-1) +, Programmed Death-Ligand 1 (PD-L1) >80%), and next-generation sequencing revealed a MET exon 14 skipping mutation. He received capmatinib (800 mg/day) and denosumab, with SBRT to vertebral metastases and later to the primary lung tumor. Capmatinib was held five days before and resumed five days after each SBRT course. Treatment was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
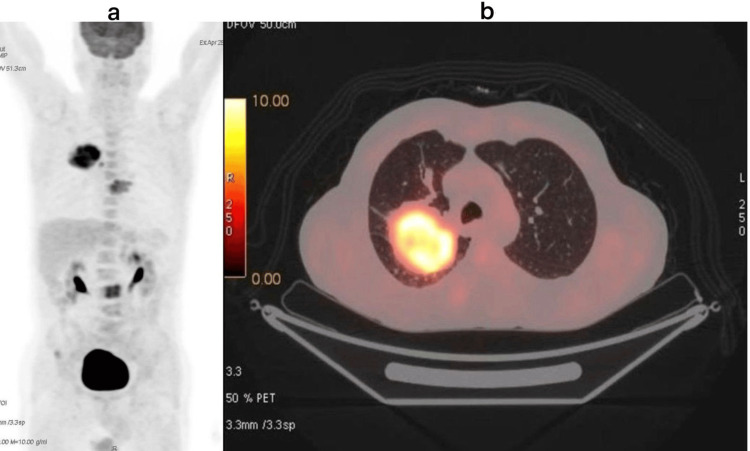 Figure 1
Figure 1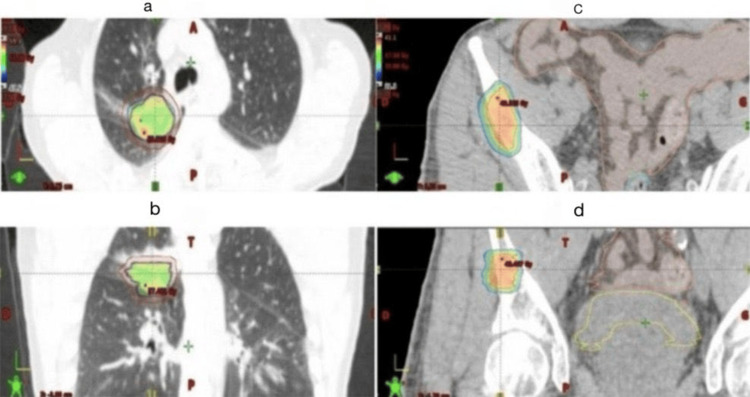 Figure 2
Figure 2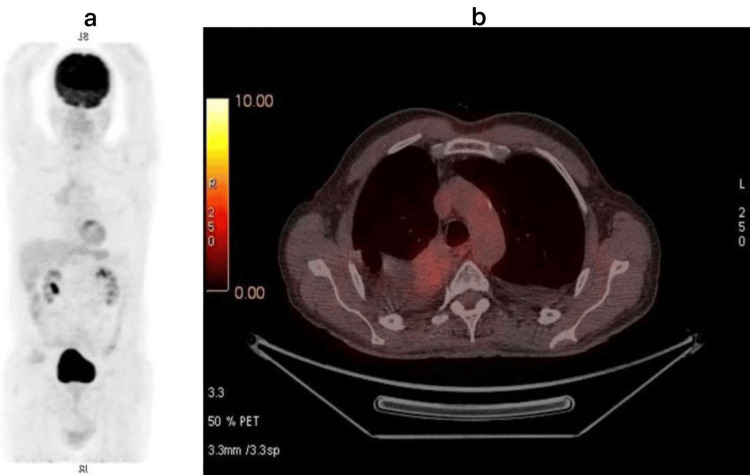 Figure 3
Figure 3| Parameters | Patient Results | Units | Reference Range | |
| Hematology (CBC) | Hemoglobin | 14.1 | g/dL | 13 – 17 (M) |
| Hematocrit | 42 | % | 36 – 46 | |
| Red Blood Cells | 4.7 | T/L | 4.0 – 5.2 | |
| Mean Corpuscular Volume | 89 | fL | 80 – 100 | |
| Mean Corpuscular Hemoglobin | 30 | pg | 27 – 32 | |
| Mean Corpuscular Hemoglobin Concentration | 34 | g/dL | 32 – 36 | |
| Total White Blood Cells | 7.0 | G/L | 4 – 10 | |
| Neutrophils | 4.1 | G/L | 1.5 – 7.5 | |
| Lymphocytes | 2.3 | G/L | 1.0 – 4.0 | |
| Monocytes | 0.4 | G/L | 0.1 – 1.0 | |
| Eosinophils | 0.2 | G/L | 0 – 0.5 | |
| Basophils | 0.1 | G/L | 0 – 0.2 | |
| Platelets | 247 | G/L | 150 – 400 | |
| C-Reactive Protein | 13 | mg/L | < 5 | |
| Liver and renal function | Aspartate Transferase (SGOT) | 25 | U/L | < 35 |
| Alanine Aminotransferase (SGPT) | 30 | U/L | < 45 | |
| Total Bilirubin | 10 | µmol/L | < 17 | |
| Conjugated Bilirubin | 3 | µmol/L | < 5 | |
| Urea | 0.36 | g/L | 0.15 – 0.45 | |
| Creatinine | 8.5 | mg/L | 6 – 12 | |
| Electrolytes | Sodium | 140 | mmol/L | 135 – 145 |
| Potassium | 4.1 | mmol/L | 3.5 – 5.0 | |
| Chloride | 103 | mmol/L | 98 – 107 | |
| Bicarbonate | 25 | mmol/L | 22 – 28 | |
| Calcium (total) | 2.35 | mmol/L | 2.15 – 2.50 | |
| Magnesium | 0.85 | mmol/L | 0.75 – 0.95 | |
| Metabolites | Total Protein | 53 | g/L | 65 – 80 |
| Albumin | 37 | g/L | 35 – 50 | |
| Fasting Glucose | 1.10 | g/L | 0.7 – 1.1 | |
| HbA1c (Glycated Hemoglobin) | 9.0 | % | < 5.7 (normal) / < 7 (controlled diabetes) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
Non-small cell lung cancer (NSCLC) remains the leading cause of cancer-related mortality worldwide, accounting for nearly 85% of all lung cancer cases [1]. Despite therapeutic progress, advanced disease continues to be associated with a poor prognosis. Nevertheless, the recognition of an oligometastatic state, defined by a limited number of metastatic sites, has identified a biologically distinct subset of patients who may benefit from aggressive multimodal management combining systemic and local ablative therapies, potentially achieving long-term disease control.
The advent of molecular profiling has revolutionized the management of NSCLC by uncovering actionable oncogenic drivers that guide precision therapies. Among these, MET exon 14 (METex14) skipping mutations lead to dysregulated MET signaling through impaired receptor degradation, driving tumor proliferation and survival [2].
Capmatinib, a highly selective MET inhibitor, has demonstrated robust and durable systemic efficacy in patients with advanced METex14-mutated NSCLC, establishing its role as a key component of targeted therapy [3]. In parallel, stereotactic body radiotherapy (SBRT) has emerged as an effective local treatment for primary and metastatic lesions in oligometastatic NSCLC, providing excellent local control with a favorable toxicity profile [4].
The combination of targeted therapies and SBRT represents a promising therapeutic avenue, potentially leveraging synergistic effects between systemic molecular inhibition and local tumor ablation. However, very few studies have specifically evaluated the safety and efficacy of combining capmatinib with SBRT in MET-driven NSCLC, leaving an important gap in clinical evidence.
Here, we report the case of a patient with oligometastatic NSCLC harboring a METex14 skipping mutation, who achieved a dramatic and durable response following a combined approach using capmatinib and SBRT targeting both the primary tumor and metastatic sites.
Case presentation
A 73-year-old man with a 10-year history of well-controlled type 2 diabetes mellitus and a 25 pack-year smoking history presented with a productive cough and hemoptysis, associated with a 3-kg weight loss and general health deterioration.
Chest computed tomography (CT) revealed a 9 × 7.5 × 5 cm right upper lobe mass, two intertracheobronchial lymph nodes measuring 12 mm, and a lytic lesion of the D7 vertebral body. Bronchoscopy was non-diagnostic, while CT-guided transthoracic biopsy confirmed a moderately differentiated adenocarcinoma, positive for thyroid transcription factor-1 (TTF-1). At presentation, the patient had an Eastern Cooperative Oncology Group (ECOG) performance status of 1 and reported persistent left thoracic pain. Staging with brain MRI demonstrated a small (3 mm) parasagittal enhancing focus. Whole-body fluorine-18 fluorodeoxyglucose positron emission tomography (FDG-PET)/computed tomography (CT) revealed a hypermetabolic right upper lobe lesion (SUV_max_ 13.9), mediastinal lymph node involvement, and bone metastases at T8 and L3 (Figure 1).
Images from the initial FDG-PET/CT showing the primary lung lesion (a: coronal view; b: axial view)FDG: fluorine-18 fluorodeoxyglucose
Spinal MRI confirmed vertebral lesions at D8 and L4, extending to the posterior elements without spinal cord compression, and additional suspicious lesions at C3 and T4.
The diagnosis of oligometastatic lung adenocarcinoma with limited brain and bone involvement was established. Immunohistochemistry showed CK7+, CK20+, TTF-1+, P40-, and programmed death-ligand 1 (PD-L1) >80%. Next-generation sequencing (NGS) confirmed positivity for a METex14 skipping mutation, with no EGFR, RAS, or MEK alterations.
Based on these findings, a multidisciplinary tumor board recommended targeted therapy with capmatinib (800 mg/day) in combination with denosumab (120 mg every three weeks). The patient initially received SBRT to vertebral metastases (30 Gy in three fractions of 10 Gy), resulting in prompt pain relief. As the brain metastasis was asymptomatic, it was not irradiated.
Before initiating capmatinib, the patient underwent a complete baseline biologic and cardiac assessment, including complete blood count (CBC), renal and hepatic function tests (creatinine, electrolytes, aspartate transferase (AST), alanine transaminase (ALT), bilirubin), and fasting blood glucose to ensure safe management of his diabetes (Table 1).
A 12-lead ECG was obtained to evaluate baseline cardiac rhythm and QT interval. During treatment, these parameters were monitored regularly, with CBC, renal and hepatic function, and fasting glucose assessed at least monthly, and ECG repeated if clinically indicated, allowing early detection and management of any hematologic, hepatic, renal, metabolic, or cardiac toxicity.
Three months after treatment initiation, FDG-PET/CT demonstrated a partial metabolic and volumetric regression of the primary lung lesion (SUV_max_ 9.4 vs. 13.9; volume 16 cm³ vs. 50 cm³) and resolution of bone hypermetabolism. Capmatinib was continued with good tolerance.
After 10 months, imaging revealed further regression of the primary tumor and complete resolution of mediastinal uptake, with decreased bone activity. Following multidisciplinary reassessment, SBRT to the primary lung lesion (50 Gy in five fractions of 10 Gy) was delivered (Figure 2). Capmatinib was held five days before and resumed five days after SBRT to minimize potential radiosensitization effects.
Lung SBRT for the primary lesion (a,b) and SBRT of the pelvic metastatic lesion (c,d) SBRT: stereotactic body radiotherapy
Subsequent brain MRI demonstrated complete resolution of the previously enhancing lesion. Follow-up FDG-PET/CT confirmed ongoing metabolic regression of pulmonary and bone lesions, with only mild uptake in a right subpleural nodule interpreted as post-therapeutic. A repeat biopsy revealed macrophagic alveolitis without malignant cells.
Eighteen months after diagnosis, the patient developed isolated oligoprogression in the right iliac crest, which was successfully treated with pelvic SBRT (30 Gy in three fractions of 10 Gy) (Figure 2).
At the most recent follow-up (24 months after diagnosis), the patient remains alive, asymptomatic, and on continuous capmatinib therapy, with no evidence of disease progression, no newly developed hypermetabolic foci on the last FDG-PET/CT imaging (Figure 3), preserved organ function, and excellent tolerance and performance status.
Images from the last FDG-PET/CT showing a complete response (a: coronal view; b: axial view)FDG: fluorine-18 fluorodeoxyglucose
Discussion
METex14 skipping mutations and other activating alterations in the MET kinase domain represent a relatively uncommon molecular subset of NSCLC, accounting for approximately 3-4% of cases [5]. These alterations are usually mutually exclusive with canonical oncogenic drivers such as EGFR, KRAS, ALK, or RET, defining a distinct biological and clinical entity with unique therapeutic implications [6]. In the present case, the absence of concomitant genomic aberrations simplified the molecular landscape but simultaneously limited alternative targeted therapeutic options, making MET inhibition the principal systemic strategy [7]. Capmatinib, a highly selective MET tyrosine kinase inhibitor (TKI), has demonstrated robust efficacy in both treatment-naïve and previously treated NSCLC patients harboring METex14 skipping mutations, with overall response rates ranging from 41% to 68% and durable responses in selected individuals [8]. However, despite these encouraging outcomes, systemic therapy alone may not be sufficient to achieve complete and durable control of oligometastatic disease, due to heterogeneous tumor microenvironments, variable drug penetration, and the emergence of resistant subclones [9].
The integration of local ablative radiotherapy, particularly SBRT, with targeted therapy has been proposed as a rational strategy to consolidate systemic responses and improve long-term outcomes [10]. Preclinical evidence indicates that MET signaling contributes to radioresistance through enhanced DNA repair, activation of prosurvival pathways, and promotion of tumor proliferation [11]. Consequently, MET inhibition may sensitize tumor cells to radiation-induced DNA damage, impair repair mechanisms, and enhance apoptosis [12]. Radiation, in turn, can modulate the tumor microenvironment, promote antigen presentation, and potentially synergize with targeted agents to induce systemic antitumor effects [13]. This bidirectional interaction provides a compelling biological rationale for combining MET inhibition with SBRT in MET-driven NSCLC, particularly in the oligometastatic setting where local tumor control can have an outsized impact on survival and quality of life [14].
Clinical evidence for the combination of capmatinib and SBRT remains scarce, limited to isolated case reports and small retrospective series [15]. These reports suggest that sequential or concurrent administration of SBRT with MET inhibition is feasible, can be well tolerated, and may enhance the durability of response [16]. In the present case, SBRT was initially applied to vertebral metastases and later to the primary lung lesion, with capmatinib held five days before and resumed five days after each course to minimize potential additive toxicity while maintaining radiosensitization effects [17]. This approach allowed for careful hematologic, hepatic, renal, and cardiac monitoring, as well as assessment of glycemic control in our diabetic patient, thereby ensuring safety during treatment. The patient experienced no significant hematologic, hepatic, or pulmonary adverse events, supporting the feasibility of this strategy even in individuals with comorbidities.
The clinical outcome in this patient was remarkable, with rapid and durable regression of both irradiated and non-irradiated lesions, sustained disease control of metastatic sites, and normalization of metabolic activity on follow-up imaging. The observation of tumor regression at non-irradiated sites raises the possibility of systemic immune modulation or abscopal-like effects, suggesting that the combination of targeted therapy and SBRT may confer synergistic antitumor activity beyond the directly irradiated volume [17]. Furthermore, the sequential application of SBRT to metastatic and primary sites in conjunction with continuous capmatinib allowed for durable local control, delayed oligoprogression, and minimal toxicity, highlighting the potential of this dual-modality approach in selected oligometastatic patients [18].
This case underscores several important clinical and scientific points. Comprehensive molecular profiling should be systematically implemented in NSCLC, as identification of actionable mutations such as METex14 skipping can dramatically alter the therapeutic trajectory [19]. In the era of precision oncology, combining molecularly targeted agents with highly focused ablative radiotherapy may represent a promising paradigm for managing oligometastatic disease [20]. Careful attention to treatment sequencing, timing of drug interruption, and systematic monitoring of hematologic, hepatic, renal, cardiac, and metabolic parameters is essential to ensure safety and maximize therapeutic benefit. Prospective studies are urgently needed to define the optimal combination schedule, clarify potential synergistic mechanisms, and establish long-term efficacy and safety of SBRT with MET-targeted therapy.
Conclusions
This case contributes to the growing body of evidence that rational integration of targeted systemic therapy and precision radiotherapy can achieve durable tumor control in MET-driven NSCLC, providing a potential framework for future treatment strategies in this rare but clinically significant molecular subset. By demonstrating the feasibility, safety, and efficacy of combining capmatinib with SBRT, this observation may inform clinical decision-making and stimulate further investigation into multimodal management approaches for oligometastatic NSCLC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lung cancer-epidemiology, pathogenesis, treatment and molecular aspect (review of literature)Int J Mol Sci Smolarz B Łukasiewicz H Samulak D Piekarska E Kołaciński R Romanowicz H 26202510.3390/ijms 26052049 PMC 1190095240076671 · doi ↗ · pubmed ↗
- 2Rare synchronous lung cancers in a nonsmoker with epidermal growth factor receptor and mesenchymal-epithelial transition alterations: a case report Case Rep Oncol Baer X Chevallier M Rey Cobo J Plojoux J De Vito C Addeo A 5495551720243861827710.1159/000538019 PMC 11014720 · doi ↗ · pubmed ↗
- 3Profile of capmatinib for the treatment of metastatic non-small cell lung cancer (NSCLC): patient selection and perspectives Cancer Manag Res Fraser M Seetharamu N Diamond M Lee CS 123312431520233794197110.2147/CMAR.S 386799 PMC 10629434 · doi ↗ · pubmed ↗
- 4Stereotactic radiotherapy for ultra-central lung oligometastases in non-small-cell lung cancer Cancers (Basel) Loi M Franceschini D Dominici L 8851220203226056810.3390/cancers 12040885 PMC 7226119 · doi ↗ · pubmed ↗
- 5Advances in clinical research of MET exon 14 skipping mutations in non-small cell lung cancer J Cancer Res Clin Oncol Wang M Zhang S Yi D 7815120253993729110.1007/s 00432-025-06115-y PMC 11821758 · doi ↗ · pubmed ↗
- 6RET-altered cancers—a tumor-agnostic review of biology, diagnosis and targeted therapy activity Cancers (Basel) Desilets A Repetto M Yang SR Sherman EJ Drilon A 41461520233762717510.3390/cancers 15164146 PMC 10452615 · doi ↗ · pubmed ↗
- 7Aberrant MET receptor tyrosine kinase signaling in glioblastoma: targeted therapy and future directions Cells Al-Ghabkari A Huang B Park M 2181320243833461010.3390/cells 13030218 PMC 10854665 · doi ↗ · pubmed ↗
- 8The biology and treatment of oligometastatic cancer Oncotarget Reyes DK Pienta KJ 84918524620152594069910.18632/oncotarget.3455 PMC 4496163 · doi ↗ · pubmed ↗