Longitudinal healthcare utilization among traumatic spinal cord injury patients: a 20 year retrospective study using population-based data
Michael Bond, Aidan Beresford, Vanessa K. Noonan, Naama Rotem-Kohavi, Brian K. Kwon, Guiping Liu, Jason M. Sutherland

TL;DR
This study examines healthcare use over 20 years in spinal cord injury patients, finding higher use among older individuals and those with cervical injuries.
Contribution
The study provides a 20-year longitudinal analysis of healthcare utilization patterns in TSCI patients using population-based data.
Findings
Patients had 18.9 primary care visits and 13.9 specialist visits per person year on average.
Cervical injury and urban residence were associated with higher healthcare utilization.
Older patients (65+) used more healthcare resources than younger patients.
Abstract
Patients with traumatic spinal cord injury (TSCI) experience the healthcare system in a heterogeneous fashion after initial injury. This study performs a retrospective analysis of administrative data to identify patterns of longitudinal healthcare utilization among patients with TSCI in British Columbia, Canada, up to 20 years after initial hospitalization. Using population-based administrative databases, adult patients with incident TSCIs were identified between January 2001 and December 2021. Population-based healthcare administrative and demographic data were used to determine physician services (primary care and specialist), hospital admissions (elective surgical, medical, and emergency department), and clinical information. Descriptive summaries measuring healthcare utilization per person year were calculated. Average utilization calculated in person years since the time of injury…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
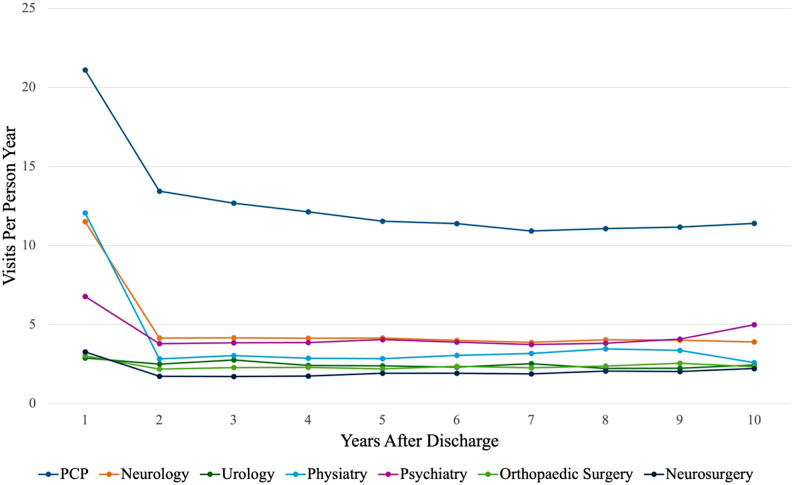 Figure 1
Figure 1- —https://doi.org/10.13039/100009520Praxis Spinal Cord Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Cord Injury Research · Traumatic Brain Injury Research · Cervical and Thoracic Myelopathy
Background
Traumatic spinal cord injury (TSCI) is a significant event that has long-lasting implications for the individual and their use of healthcare services and resources [1]. TSCIs can result in irreversible damage to sensory and motor function and lead to medical complications that impact quality of life [2, 3]. Although TSCIs are rare events, with a global rate of 1 in 23 million [4], the demand for healthcare services among this population is high due to the complex nature of the injury requiring long-term care and support. Higher healthcare utilization can create a significant economic impact on healthcare systems and patients, in addition to the need for comprehensive acute and rehabilitation-based care immediately after initial injury [5–8]. Further, the demographics of TSCI are shifting, and there is an increasing incidence of TSCIs among the elderly population due to low-energy falls [9, 10]. The increased rate of elderly patients suffering TSCI from low-energy falls may cause new system-level challenges, given that elderly TSCI patients are more likely to have multiple medical issues and chronic disease diagnoses prior to their spinal cord injury, requiring more specialized and complex care [11, 12]. There is a paucity of information regarding healthcare utilization among those with TSCI.
Management of TSCI after acute hospitalization involves transition into community-based care, and for many TSCI patients, there is no clear clinical pathway that provides access to out-of-hospital services [13–15]. In many healthcare systems, delivery of healthcare to TSCI patients is provided through a variety of services, settings and providers, causing difficulties with navigating appropriate care [16]. The transition to outpatient care is a particular challenge in Canada due to a lack of rehabilitation services provided through public insurance to assist patients in post-injury rehabilitation, often creating a patchwork of services provided to those with TSCI [17]. Given this, how and where TSCI patients access healthcare services is poorly understood. This lack of insight makes it difficult for clinicians, patients, and policymakers to address gaps in care, anticipate healthcare staffing needs, and develop clinical care pathways that aim to improve the health of TSCI patients across the lifespan.
The objective of this study is to describe patterns of longitudinal healthcare utilization, including primary care physicians (PCP), specialist consultations, emergency department (ED) visits, and all-cause hospital admissions among TSCI patients in the province of British Columbia (B.C.), Canada, using population-based data. A secondary objective is to determine which patient or system-level characteristics are associated with higher rates of utilization. This study’s findings are important to patients, clinicians and policymakers as they will illustrate the constellation of patients’ healthcare utilization following TSCI and identify gaps where access to healthcare services can be improved.
Methods
Study design and population
This study was based on retrospective data from a population-based observational cohort of adults having had a TSCI in the province of B.C. between January 2001 and December 2021. This study utilized population-based hospital and physician-based administrative data routinely collected and maintained for research purposes by Population Data B.C [18]. Population Data B.C. provides research access to linkable, longitudinal, de-identified patient-level datasets for all publicly insured individuals in the province. Data was extracted from several sources, including the Canadian Institute for Health Information Discharge Abstract Database (DAD), B.C. Provincial Vital Statistics, the National Ambulatory Care Reporting System (NACRS), and the Medical Services Plan (MSP) Payment Information File, which includes physician billing data [19–23]. The protocol for linkage has been described elsewhere [24]. Patients not publicly funded through MSP were not included in this study, this included temporary visitors and tourists, and federally funded groups such as those active in the Canadian Armed Forces or incarcerated in a federal penitentiary.
The cohort was created based on identifying hospital discharge records with an International Classification of Diseases 10-CA diagnosis code (see Appendix 1 for list of codes) for TSCI. The cohort included all patients hospitalized for acute cervical, thoracic, lumbar, sacral, or cauda equina TSCIs in B.C. over the study period. The TSCI case definition was validated by mapping ICD-10-CA codes to International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) descriptions of TSCI by level and severity and has been described elsewhere [24]. Patients were excluded if they died during initial hospitalization or were under the age of 18 at the time of injury. All patients were continuously insured throughout the study period through provincially funded and publicly available plans. For cohort members, administrative and clinical data were deterministically linked and anonymous to the study team. This unique linked data has been described elsewhere [24]. Ethics approval for analysis of population-based data was obtained from the University of British Columbia Research Ethics Board (REB#: H22-02696).
Demographic and clinical variables
The demographic and clinical variables were identified from the initial TSCI injury hospitalization, and included age (grouped in categories < 35, 35–64, and ≥ 65 years old), sex (male, female), Charlson Comorbidity Index (CCI), mechanism of injury (falls, transport, other), and level of injury (cervical vs. thoracic/lumbar), presence of traumatic brain injury (TBI), and Injury Severity Score (ISS) [25]. Sociodemographic status was determined using the Quintile of Adjusted Income per person Equivalent (QAIPPE) [26], which is a measure of neighbourhood income adjusted for household size determined by Statistics Canada. Place of residence was determined as rural or urban based on the first 3 characters in their postal code [22].
Outcomes
The main outcome of this study was the rate of utilization of physician-based services, as identified through physician billing data and expressed as visits per person year averaged from the time of injury to the end of the study period in December 2021. Physician-based services included PCP visits and specialist visits (including neurologists, physical medicine and rehabilitation, orthopaedic surgeons, neurosurgeons, urologists, and psychiatrists). Hospital-based care was identified using the DAD, identifying patients admitted to the hospital for acute medical issues, emergency surgeries or having had elective surgical procedures. For all ED visits, physician billing data (MSP) was used to identify the service date of the physician consultation. Physician visits or multiple billings on the same day were counted as a single encounter.
Statistical analysis
Demographic and clinical information were summarized using means and standard deviations for continuous variables and counts for categorical variables. Health care visits were reported in rates per person year for all participants to capture all observed time for each patient after discharge from acute care. Physician visits per person year in the outpatient setting were calculated for primary care and specialist interactions during the study period. Inpatient hospitalizations, ED visits, and elective surgical procedures were summarized similarly. Comparisons between the rates of visits per person year were performed using level of injury (cervical and thoracic/lumbar injury) and age category (≥ 65 years old and. < 65 years old). Per person year rates and confidence intervals were calculated using Poisson regression. Overdispersion was addressed by applying a scaling parameter to the estimated variance. Statistical significance was set a p < 0.05, and all statistical analysis was performed using SAS v9.4.
To identify clinical and demographic characteristics of patients with TSCI who access healthcare services most frequently, a finite mixture model latent class model was fit using maximum likelihood. In this analysis, the observed variables included were per patient-year visits for primary care, specialists’ services (urology, neurology, orthopedic, neurosurgery, physiatry, and psychiatry) and per-patient-year visits for elective surgeries. Other variables included in the model were patient age (< 65 or ≥ 65 years), sex, CCI, QAIPPE, and place of residence (urban vs. rural). A multi-group latent class analysis used level of injury to identify two distinct groups. Further refinement of the classes selected was accomplished using the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). A step-wise approach was taken to add additional latent classes into the model; based on the fit criteria the 4-class model described variability in the data the best. Latent class analysis was performed using Mplus V8.3 [27]. Nonparametric bootstrap techniques were applied to address non-normality of the data.
Results
Over the course of this 22-year study period, 4132 patients met the cohort’s inclusion criteria. The mean age was 55.1 years (SD 19.64), and 2973 (72.0%) were male. In this cohort, 1661 (40.2%) patients had thoracic/lumbar Injuries, and 2471 (59.8%) had cervical spinal cord injuries. 1762 (42.6%) of patients received their injury from a fall. (See Table 1 for full demographic and clinical details).
Table 1. Summary presentation of the TSCI cohortCharacteristicTotal (N = 4132)Age (SD)55.1 (19.2)Male2973 (72.0%)Charlson Comorbidity Index (SD)0.3 (0.9)QAIPPE 1- Lowest985 (23.8%) 2846 (20.5%) 3801 (19.4%) 4726 (17.6%) 5689 (16.7%) Missing85 (2.1%)Level of Injury Cervical (C1-C8)2471 (59.8%) Thoracic (T1-T12)660 (16.0%) Lumbar (L1-L5)947 (22.9%) Sacral/Cauda Equina (S1-S5)54 (1.3%)Injury Severity Score24.2 (13.6)Traumatic Brain Injury Yes543 (13.1%) No3589 (86.9%)Mechanism of Injury Falls1762 (42.6%) Transport1241 (30.0%) Others1129 (27.4%)Demographic and clinical characteristics and stratified by level of injury (Thoracic / Lumbar Injury vs. Cervical Injury)
The study found that on average, patients with TSCI were seen by a PCP 18.9 (18.0 to 19.9 95% C.I.) visits per patient-year since the time of their injury. All specialist visits averaged 13.9 (13.1 to 14.7 95% C.I.) visits per patient-year, with neurology having had 6.4 (6.0 to 6.7 95% C.I.) visits per patient-year, physiatry 5.3 (4.8 to 5.7 95% C.I.) visits per patient-year, and psychiatry with 3.1 (2.8 to 3.4 95% C.I.) visits per patient-year. Further, it was identified that patients with cervical spinal cord injuries and those 65 and over visited both PCPs and specialists more frequently compared with those under 65 (p < 0.001). Patients with TSCI were admitted to the hospital 1.4 (1.3 to 1.5 95% C.I.) times per patient-year, had 0.6 (0.6 to 0.7 95% C.I.) visits per patient-year to the ED and had 0.3 (0.3 to 0.4 95% C.I.) elective surgical procedures per patient-year. Those with cervical injuries or aged 65 and over were hospitalized most frequently. See Table 2 for further details.
Table 2. Rates of primary Care, Specialist, hospital admissions, elective surgeries, and ED visits per patient-year. The Poisson distribution was used to Establish 95% confidence intervalsTotalThoracic / Lumbar InjuryCervical InjuryAge < 65Age ≥ 65RateCIRateCIRateCIRateCIRateCIPrimary Care18.9(18.0 to 19.9)17.1(15.7 to 18.4)20.3(18.9 to 21.6)13.8(13.1 to 14.4)30.1(27.5 to 32.7)Specialist Urology1.4(1.3 to 1.4)1.3(1.1 to 1.4)1.4(1.3 to 1.6)1.1(1.1 to 1.2)1.9(1.7 to 2.2) Neurology6.4(6.0 to 6.7)4.8(4.4 to 5.3)7.4(6.9 to 8.0)5.3(4.9 to 5.7)8.6(7.8 to 9.4) Orthopaedic1.2(1.1 to 1.3)1.1(1.0 to 1.2)1.3(1.1 to 1.5)1.0(0.9 to 1.1)1.8(1.4 to 2.2) Neurosurgery1.5(1.3 to 1.8)1.2(1.0 to 1.3)1.8(1.4 to 2.2)1.0(0.8 to 1.2)2.6(2.0 to 3.2) Physiatry5.3(4.8 to 5.7)3.8(3.2 to 4.3)6.1(5.5 to 6.7)4.7(4.2 to 5.2)6.7(5.8 to 7.7) Psychiatry3.1(2.8 to 3.4)2.6(2.2 to 3.0)3.5(3.0 to 4.0)2.8(2.4 to 3.1)3.9(3.2 to 4.6)Hospital Admissions1.4(1.3 to 1.5)1.2(1.1 to 1.3)1.5(1.4 to 1.7)1.1(1.0 to 1.1)2.1(1.9 to 2.3)Elective Surgeries0.3(0.3 to 0.4)0.4(0.3 to 0.4)0.7(0.6 to 0.7)0.3(0.3 to 0.4)0.5(0.4 to 0.5)Emergency Department0.6(0.6 to 0.7)0.6(0.6 to 0.6)0.3(0.3 to 0.3)0.5(0.5 to 0.6)0.9(0.8 to 1.0)
Figure 1 illustrates the trends in healthcare utilization for physician services in the first 10 years after discharge for TSCI. This figure demonstrates that cohort members had the highest healthcare utilization in the first year following their discharge from acute care. Rates of PCP and specialist visits decreased after the first year and remained stable over time.
Fig. 1. Physician visits over 10 years after discharge from acute care for all TSCI patients
Latent class analysis found four mutually exclusive groups based on healthcare utilization patterns. These four patterns were divided by level of the spinal cord injury (cervical spine vs. thoracic/lumbar injury) and the location of residence (rural vs. urban). Those who had cervical spinal cord injuries and were living in urban centers had the highest rates of healthcare utilization. Those who had thoracic/lumbar injuries and lived in rural locations at the time of their injury had the lowest rates of healthcare utilization. See Table 3 for details.
Table 3. Latent class analysis model and visits estimates with standard errors, including four classes; class 1: Thoracic/Lumbar – Urban, class 2: Thoracic/Lumbar – Rural, class 3: Cervical – Urban, class 4: Cervical – RuralClass OneN = 1355Class TwoN = 266Class ThreeN = 1886Class FourN = 369EstimateStandard ErrorEstimateStandard ErrorEstimateStandard ErrorEstimateStandard ErrorPrimary Care17.640.7213.991.3320.750.4916.411.60Specialist (Total)11.400.676.750.9217.200.4512.031.65 Urology0.670.032.470.427.460.214.920.77 Neurology4.930.320.740.100.790.090.500.13 Orthopaedic0.740.030.810.081.260.091.120.16 Neurosurgery0.850.071.230.344.160.193.120.61 Physiatry2.070.261.050.082.770.191.790.34 Psychiatry2.160.096.760.9217.200.4512.001.65Hospital Admissions1.200.041.150.101.570.071.330.28Emergency Department0.570.060.240.070.610.040.340.07Elective Surgeries0.350.020.360.030.270.010.210.02
Discussion
This study provided an overview of healthcare utilization among TSCI patients. Leveraging the study setting’s single-payer healthcare system, the study provides insights regarding utilization of primary care, specialist consultations, ED visits, and all-cause hospital admissions.
Primary care is an important component in the care of patients outside of the hospital setting and helps patients navigate the health care system to access the care they need. This is especially important for patients who have complex medical requirements, like those with TSCI [28, 29]. This is reflected in the results of this study in that PCP visits were the most frequent type of physician encounter, averaging 18.9 visits per person year after their initial injury. In comparison to the general population, where a recent study by Lavergne et al. (2022) found that PCP visits averaged between 3.6 and 4.7 visits per person per year using similar data. Using the Canadian Community Health Survey, stroke survivors tended to have on average 4.9 visits per year with their PCP [30]. In this study, PCP continue to be a significant contact point for patients during their life course after injury, with much higher rates of visits on average when compared with the general population and similar conditions. This increased utilization of primary care services extended far beyond other injuries, including brain injury and pelvic fracture [31].
PCPs can manage the majority of general medical issues; however, when further input is needed for more complex issues, patients in Canada’s gatekeeper model are then referred to community or hospital-based specialty physicians, such as neurologists, urologists, spinal surgeons (orthopaedic or neurosurgical), and physical and rehabilitation medical specialists [28]. This study found that TSCI patients received specialized care most frequently from neurologists, physiatrists, and psychiatrists. Specialist care represented a significant proportion of the TSCI’s clinical activity, with 13.9 visits per person year in the first year post-discharge from acute care. Specialists contribute essential expertise in managing TSCI-related issues and guiding ongoing rehabilitation. Coordinating care between multiple physicians is often challenging and complex due to the varied needs of TSCI patients [32, 33]. Ensuring appropriate communication between the PCP and specialists to ensure optimal care is essential to this relationship. To streamline this process and enhance coordination, there has been a recognition that a multidisciplinary approach to care for patients with TSCI is optimal; however, it is often difficult to achieve in complex health systems [34]. Studies have demonstrated that these models of care, including interactions between multiple specialists, allied health rehabilitation specialists, and PCP, are essential to avoid gaps in care and reduce complications [35]. To help support PCP management of TSCI, specialists should ensure they provide PCPs with detailed guidance and instruction on how to manage more complex issues.
The latent class analysis revealed that patients who had cervical spinal cord injuries had a greater number of encounters with the healthcare system, including PCP, specialist, hospital, and ED visits. This is most certainly the result of the more diffuse perturbations across multiple physiologic systems in those with cervical-level injuries as compared to thoracic-level injuries (tetraplegia versus paraplegia), requiring additional treatments outside of their initial hospital admission [36]. Previous research has shown that patients with cervical spinal cord injuries were more likely to have had higher rates of complications and readmissions to the hospital, which likely would increase healthcare utilization and require more frequent visits to manage these problems [36–39]. In the long term, patients who had cervical injuries resulting in tetraplegia were more likely to have increased healthcare needs, including more intensive physical therapy, assistive devices, and caregiver needs, which led to higher healthcare resource utilization and spending [40].
Important for this study, this paper identified that where a patient resides has significant implications for accessing health care. Rural communities often have reduced access to healthcare providers and specialists, with a significant issue with access to PCP in the Canadian context [41]. Studies have shown that TSCI patients who reside further from spinal cord injury treatment centers were less likely to access specialized outpatient services for spinal cord injury [42]. This lack of access to care has been shown to be associated with being twice as likely to be admitted to the hospital for TSCI-related complications [43]. However, while relocation to an urban area may improve access to specialized care, it has also been associated with higher rates of depression and mental health concerns, likely due to a lack of social support from known environments [44]. Moreover, rural community networks may provide better socio-emotional support for patients with TSCI and have been associated with improved mental and physical health compared to those residing in urban communities [45, 46]. The advent of virtual care has been used to enable interactions with specialists working primarily in urban centres to provide treatment plans for TSCI-related complications and has been met with a positive response from these patients [47]. Further, there has been the implementation of workshops aimed at clinicians who work in rural communities to improve care of those with TSCI, which have demonstrated improved patient outcomes [48].
This study represented a large population-level retrospective study of physician service utilization using healthcare administrative data. The findings were representative of a single-payer healthcare system and utilized validated cohorts with a large sample size. However, there are several limitations to the study design. First, while this study evaluated the number of visits to a physician during the inclusion period, it did not characterize the nature or reason for the consultation. Second, many rehabilitation services delivered in the community and community-based home care may not have been publicly insured and not observable in this study. The services provided were also not evaluated to determine whether the consultations were meeting the patients’ needs or associated with patient outcomes. Next, the cohort was created based on hospital administrative data’s diagnostic codes. These codes are entered through hospital record review, but may contain errors and inaccuracies in reporting. The extent of neurological injury could also not be ascertained using these population-based databases. Finally, this study included data from the COVID-19 pandemic where changes in the delivery of care could have influenced the rates of healthcare utilization. However, studies have demonstrated that although in-person visits dramatically declined during the pandemic, the adoption of virtual care maintained steady rates of utilization for primary care, especially in Canada where the quick adoption of virtual care occurred [49]. This study included both virtual and in-person appointments in its analysis.
Implications for care and policy
This study identified that patients with TSCI are frequent users of healthcare resources, with the most significant being primary care. This study builds upon previous knowledge in that patients who access services more are those who have cervical spinal cord injuries, likely worse neurological function, and those who live within urban centers. Future systems should be put in place to allow for improved access to care for patients with TSCI, with not just a focus on improving visit rates, but more importantly, the quality of care provided. PCPs should be provided with adequate resources and care guidelines for people with TSCI to help manage complex issues and ensure appropriate communication with specialists to ensure continuity of care. The Spinal Cord Injury Research Evidence (SCIRE) Professional group have established several guidelines and provides clinical updates specifically for PCP to help manage TSCI in the community [50]. Ideally, patients should be matched to a PCP with a special interest in TSCI and prior to discharge from hospital.
Priority must be given to the establishment of multidisciplinary teams of PCPs, specialists, and allied health services, which have been shown to improve outcomes and streamline care [34, 51]. Research and quality improvement initiatives should be aimed at improving efficiency and optimizing outcomes in TSCI by collaborating with specialized spinal cord injury centres and fostering relationships that span into community care [52]. Multidisciplinary team management of these patients in the community setting will be instrumental in assessing and providing optimal usage of health care resources, education for PCP, and help to improve communication amongst professionals to improve care. Finally, with the development and implementation of these multidisciplinary teams, research can determine which services are necessary and improve outcomes, reducing unnecessary medical encounters and healthcare spending.
Conclusions
Among patients with TSCI, PCPs were found to be the primary contact with the healthcare system after their initial injury. Latent class analysis determined four distinct typologies of TSCI healthcare utilization, with cervical injury and urban residence being identified as the key components. Further research is needed to determine the differences in patterns of utilization based on extent of neurological injury and to evaluate whether multidisciplinary teams can improve access to care for those with TSCI.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zarmer L, Khan M, Islat G, Alameddin H, Massey M, Chaudhry R. Traumatic spinal cord injury: review of the literature. J Clin Med. 2025;14. 10.3390/jcm 14113649.10.3390/jcm 14113649 PMC 1215525540507410 · doi ↗ · pubmed ↗
- 2Merritt CH, Taylor MA, Yelton CJ, Ray SK. Economic impact of traumatic spinal cord injuries in the United States. Neuroimmunol Neuroinflamm. 2019;2019. 10.20517/2347-8659.2019.15.10.20517/2347-8659.2019.15PMC 805210033869674 · doi ↗ · pubmed ↗
- 3Chamberlain JD, Deriaz O, Hund-Georgiadis M, Meier S, Scheel-Sailer A, Schubert M, et al. Epidemiology and contemporary risk profile of traumatic spinal cord injury in Switzerland. Inj Epidemiol. 2015;2. 10.1186/s 40621-015-0061-4.10.1186/s 40621-015-0061-4PMC 463025926550554 · doi ↗ · pubmed ↗
- 4Wang TY, Park C, Zhang H, Rahimpour S, Murphy KR, Goodwin CR, et al. Management of acute traumatic spinal cord injury: a review of the literature. Front Surg. 2021;8. 10.3389/fsurg.2021.698736.10.3389/fsurg.2021.698736 PMC 871045234966774 · doi ↗ · pubmed ↗
- 5Ark TK, Kesselring S, Hills B, Mc Grail KM, Population Data BC. Supporting population data science in British Columbia. Int J Popul Data Sci. 2020;4. 10.23889/ijpds.v 5i 1.1133.10.23889/ijpds.v 4i 2.1133 PMC 748032532935036 · doi ↗ · pubmed ↗
- 6Canadian Institute for Health Information. Discharge Abstracts Database (Hospital Separations) data set: V 2. Population Data BC. 2019. https://www.popdata.bc.ca/data/health/dad. Accessed 20 Mar 2024.
- 7British Columbia Ministry of Health. Vital Events Deaths. V 2. Population Data BC. 2019. https://www.popdata.bc.ca/data/demographic/vs_deaths. Accessed 20 Mar 2024.
- 8British Columbia Ministry of Health. Medical Services Plan (MSP) Payment Information File. V 2. Population Data BC. 2019. https://www.popdata.bc.ca/node/677. Accessed 20 Mar 2024.