Role of Polysomnography in Tracheostomy Decannulation in Neuromuscular Disease: A Case Report
Patrícia Pereira, Ana Luísa Vieira, Sónia Tizón

TL;DR
This case report shows how polysomnography can help decide if a patient with neuromuscular disease is ready to have their tracheostomy removed.
Contribution
The paper demonstrates the novel use of polysomnography to assess ventilatory stability in a complex neuromuscular disease case.
Findings
Polysomnography confirmed ventilatory stability in a patient with chronic respiratory insufficiency.
Standard pulmonary function tests were insufficient for this patient's complex condition.
The patient's readiness for decannulation was supported by PSG results despite daytime hypercapnia.
Abstract
Tracheostomy decannulation in patients with neuromuscular disease presents significant challenges due to impaired airway clearance, pharyngolaryngeal hypotonia, and chronic hypoventilation. Polysomnography (PSG) may provide an objective assessment of ventilatory stability and support safe decision-making. We describe a 54-year-old woman with sequelae of Arnold-Chiari malformation type I, syringomyelia, and tetraplegia (AIS D, neurological level C1), who developed chronic respiratory insufficiency requiring tracheostomy. Despite achieving nocturnal normocapnia with non-invasive ventilation, she exhibited persistent daytime hypercapnia and severely impaired cough. A capped tracheostomy PSG performed under nasal-mask non-invasive ventilation demonstrated no worsening of baseline hypoventilation, confirming ventilatory stability and supporting decannulation readiness. Anxiety delayed the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
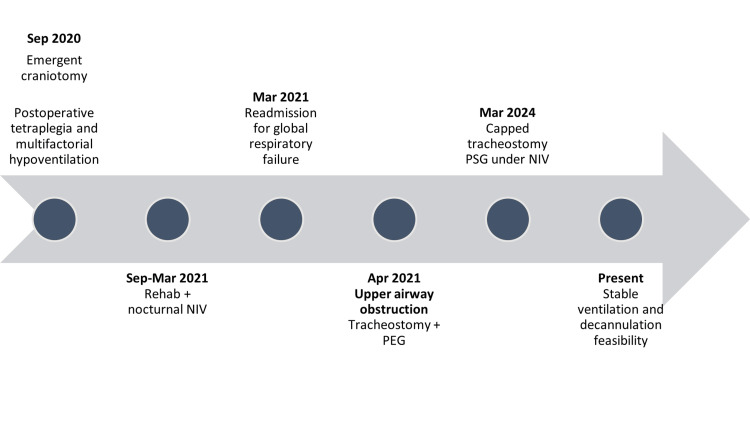 Figure 1
Figure 1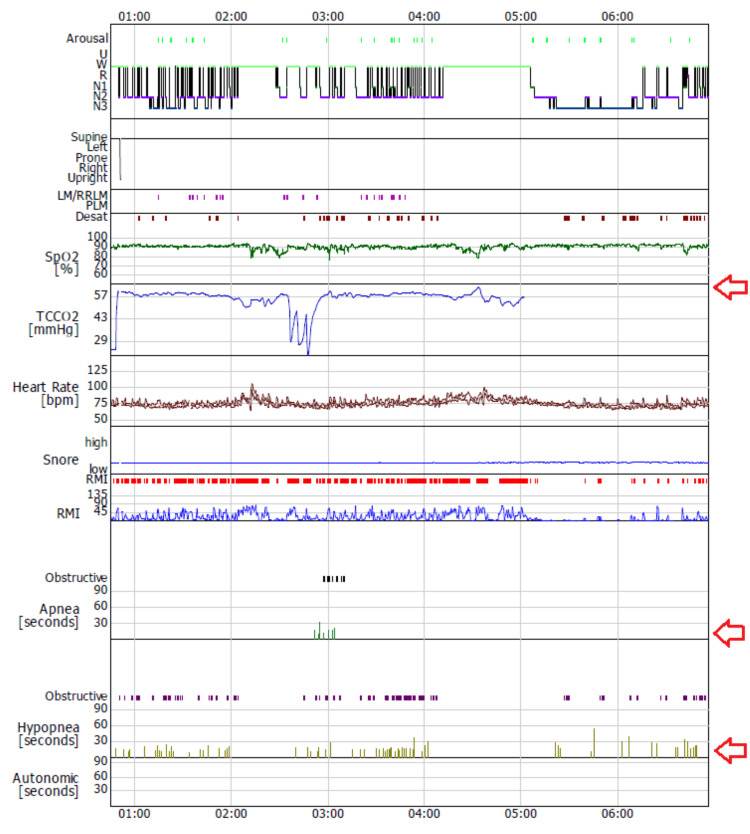 Figure 2
Figure 2| Parameter | Value | Reference values |
| Apnea + Hypopnea Index | 21.6/h | Normal <5 events/hour |
| Apnea Index | 1.9/h | Normal: < 5 events/hour |
| Hypopnea Index | 19.7/h | Normal: < 5 events/hour |
| Oxygen Desaturation Events | 11.2/h | Normal: < 5-10 events/hour |
| Mean SpO₂ | 91.4% | Normal mean sleeping SpO₂: ≥ 94% Mild reductions: 92–94% |
| Saturation <90% | 25.9 min (11.9%) | Normal < 10% |
| Arousal Index | 7.4/h | Normal < 5–10 arousals/hour |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Respiratory Support and Mechanisms · Congenital Diaphragmatic Hernia Studies
Introduction
Neuromuscular diseases frequently impair respiratory muscle strength, reduce lung volumes, and compromise airway clearance. These abnormalities predispose patients to sleep-disordered breathing and chronic hypoventilation, often necessitating tracheostomy for ventilatory support and airway protection [1,2]. Determining readiness for tracheostomy decannulation in this population is complex, particularly when daytime clinical assessment and arterial blood gases fail to predict nocturnal ventilatory stability.
Polysomnography (PSG) provides a comprehensive nocturnal assessment of airflow, respiratory effort, oxygen saturation, and carbon dioxide trends. In adults with neuromuscular disease, the purpose of PSG prior to decannulation is not necessarily to eliminate obstructive events, but to confirm that ventilatory support, most commonly non-invasive ventilation (NIV), can maintain adequate gas exchange during sleep under conditions simulating post-decannulation physiology [3,4]. This differs from pediatric decannulation paradigms, in which PSG is often used to identify surgically correctable airway obstruction. Capped-tracheostomy PSG may therefore be particularly valuable when pulmonary function testing is not feasible, or airway anatomy is compromised [5].
We present a case illustrating how PSG informed decannulation decision-making in a patient with complex neuromuscular respiratory insufficiency following Arnold-Chiari malformation type I.
Case presentation
A 54-year-old woman with a history of Arnold-Chiari malformation type I and syringomyelia experienced abrupt neurological deterioration in September 2020. She underwent emergent suboccipital decompressive craniotomy and C1 laminectomy. Postoperatively, she developed tetraplegia (American Spinal Injury Association Impairment Scale (AIS) D, neurological level C1) and multifactorial hypoventilation attributed to impaired central respiratory drive, neuromuscular weakness, and deconditioning.
From September 17, 2020, to March 15, 2021, she required prolonged hospitalization for management of respiratory insufficiency. She was discharged to inpatient rehabilitation with nocturnal bilevel positive airway pressure ventilation (inspiratory positive airway pressure 22 cmH₂O, expiratory positive airway pressure 6 cmH₂O, respiratory rate 16 breaths/min, inspiratory time 1.5 s) and mechanical insufflation-exsufflation (+40/−40 cmH₂O). Her initial tracheostomy was closed prior to discharge.
On March 17, 2021, she was readmitted with acute-on-chronic hypercapnic respiratory failure. After optimization of ventilatory support, she was again discharged on nocturnal NIV. On April 16, 2021, she developed recurrent respiratory failure associated with upper-airway obstruction caused by marked pharyngolaryngeal hypotonia, bilateral vocal cord hypomotility, and epiglottic collapse. A tracheostomy and percutaneous endoscopic gastrostomy were performed on April 28, 2021.
Nasofibrolaryngoscopy (NFL) on May 6, 2021, revealed bilateral vocal cord paralysis in the median position, absent cough reflex, significant salivary stasis, and visible aspiration. Repeat evaluation on May 28, 2021, demonstrated moderate dysphagia (Macedo and Filho grade II) with reduced laryngeal sensitivity but no frank aspiration. The Functional Oral Intake Scale (FOIS) assessment confirmed the need for supplemental enteral feeding.
Recurrent bleeding during cannula changes was attributed to a tracheal lesion near the cuff and treated with cauterization. The tracheostomy was replaced with a fenestrated, cuffed size 6 cannula. Despite achieving nocturnal normocapnia on NIV, the patient exhibited persistent daytime hypercapnia with transcutaneous carbon dioxide (TcCO₂) values around 65 mmHg. Peak cough flow was 0 L/min, indicating severely impaired airway clearance. Pulmonary function testing was not feasible due to interface limitations (Figure 1).
Case presentation timelineRehab: rehabilitation; NIV: non-invasive ventilation; PEG: percutaneous endoscopic gastrostomy; PSG: polysomnographyFigure created by the authors with Microsoft PowerPoint (Microsoft Corp., USA)
Given consideration for decannulation, a capped-tracheostomy PSG was performed to assess nocturnal ventilatory safety (Figure 2, Table 1). The tracheostomy cannula was capped with the cuff completely deflated, allowing airflow through the upper airway and simulating post-decannulation physiology. Non-invasive ventilation was delivered via a nasal mask throughout the study.
Polysomnography (PSG) summary graph The arrows indicate no worsening of baseline hypoventilation and stable transcutaneous CO₂.
PSG demonstrated consolidated sleep with 4.8% stage N1, 35.6% stage N2, 19.5% stage N3, and 0.1% rapid eye movement sleep. The Apnea-Hypopnea Index (AHI) was 21.6 events/h, predominantly obstructive hypopneas (19.7 events/h). Mean oxygen saturation was 91.4%, with a nadir of 77%, an oxygen desaturation index of 11.2 events/h, and time with saturation below 90% corresponding to 11.9% of total sleep time. Importantly, TcCO₂ remained stable throughout the night, with no worsening of baseline hypoventilation.
Although moderate obstructive events were observed, they were not associated with progressive hypercapnia or sustained oxygen desaturation. Given that the capped tracheostomy itself imposes additional airway resistance, the ability of NIV to maintain stable gas exchange under these conditions suggested that ventilatory performance after decannulation would likely be equal or superior.
Based on these findings, the multidisciplinary team (pulmonology, otolaryngology, and rehabilitation medicine) concluded that decannulation was physiologically feasible. The procedure was temporarily deferred due to patient anxiety rather than medical contraindication. Ongoing follow-up confirmed clinical stability, effective NIV use, tolerance of a speaking valve, and preserved oral intake. She remains under periodic reassessment for future decannulation.
Discussion
Assessing readiness for tracheostomy decannulation in patients with neuromuscular disease is particularly challenging. Weak cough, impaired airway clearance, and sleep-related hypoventilation all contribute to uncertainty in predicting post-decannulation respiratory stability. Daytime blood gases, clinical examination, and endoscopic airway evaluation may not reflect nocturnal respiratory physiology [1,2].
PSG provides an objective assessment of ventilation, oxygenation, and carbon dioxide control during sleep. In contrast to pediatric decannulation protocols, where PSG is often used to identify surgically correctable upper-airway obstruction, adult neuromuscular patients frequently exhibit functional airway compromise that is not amenable to operative intervention [3,6-10]. In these patients, the goal of PSG is not to normalize the AHI, but to determine whether NIV can adequately compensate for respiratory muscle weakness and upper-airway hypotonia.
In this case, PSG performed with the tracheostomy capped and cuff deflated demonstrated stable nocturnal ventilation under NIV, despite the presence of moderate obstructive hypopneas. The absence of nocturnal hypercapnia was the critical finding supporting decannulation readiness. Importantly, the capped tracheostomy represents a physiologically disadvantageous condition due to added airway resistance; therefore, effective ventilation under these circumstances provides additional reassurance regarding post-decannulation safety.
This case underscores the utility of PSG when pulmonary function testing is not feasible and highlights its role in multidisciplinary decision-making. Even when decannulation is delayed by non-medical factors, PSG can distinguish physiological readiness from psychosocial barriers and support clinician confidence in NIV-based decannulation strategies.
Conclusions
PSG can play a decisive role in assessing tracheostomy decannulation readiness in adults with neuromuscular disease and complex respiratory insufficiency. In patients for whom conventional clinical assessments and pulmonary function testing are limited or unreliable, PSG provides an objective evaluation of nocturnal ventilation, airway stability, and gas exchange under conditions that closely approximate the post-decannulation state.
By confirming ventilatory adequacy and carbon dioxide control while the tracheostomy is occluded, PSG complements endoscopic findings and multidisciplinary clinical judgment. Incorporating PSG into the decannulation assessment process may enhance patient safety and support individualized, evidence-based decision-making in high-risk neuromuscular populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Respiratory management of patients with neuromuscular weakness: An American College of Chest Physicians clinical practice guideline and expert panel report Chest Khan A Frazer-Green L Amin R 39441316420233692189410.1016/j.chest.2023.03.011 · doi ↗ · pubmed ↗
- 2Respiratory considerations in patients with neuromuscular disorders Muscle Nerve Patel N Howard IM Baydur A 1221416820233724874510.1002/mus.27845 · doi ↗ · pubmed ↗
- 3Role of polysomnography in the development of an algorithm for planning tracheostomy decannulation Otolaryngol Head Neck Surg Robison JG Thottam PJ Greenberg LL Maguire RC Simons JP Mehta DK 18018415220152538931610.1177/0194599814557467 · doi ↗ · pubmed ↗
- 4Sleep-disordered breathing in neuromuscular disease: diagnostic and therapeutic challenges Chest Aboussouan LS Mireles-Cabodevila E 88089215220172837294910.1016/j.chest.2017.03.023 · doi ↗ · pubmed ↗
- 5Sleep-disordered breathing in neuromuscular disease Am J Respir Crit Care Med Aboussouan LS 97998919120152572373110.1164/rccm.201412-2224 CI · doi ↗ · pubmed ↗
- 6Using polysomnography and airway evaluation to predict successful decannulation in children Otolaryngol Head Neck Surg Gurbani N Promyothin U Rutter M Fenchel MC Szczesniak RD Simakajornboon N 64965515320152612426610.1177/0194599815591531 · doi ↗ · pubmed ↗
- 7Inpatient observation for elective decannulation of pediatric patients with tracheostomy JAMA Otolaryngol Head Neck Surg Prickett KK Sobol SE 12012514120152542943910.1001/jamaoto.2014.3013 · doi ↗ · pubmed ↗
- 8Polysomnography: assessment of decannulation readiness in chronic upper airway obstruction Laryngoscope Wolter NE Anderson J 2574257812420142513041710.1002/lary.24836 · doi ↗ · pubmed ↗