Association between systemic inflammation and risk of atrial fibrillation in cancer survivors: a population-based cohort study using UK biobank
Quan Yang, Jiazhen Zheng, Chunting Zhao, Min Wu, Run Wang, Mingya Liu, Kai-Hang Yiu

TL;DR
Cancer survivors with higher inflammation levels may be at greater risk of developing atrial fibrillation, especially if they haven't had radiotherapy.
Contribution
This study identifies a potential link between systemic inflammation and atrial fibrillation in cancer survivors using population-based data.
Findings
Elevated C-reactive protein levels are associated with increased atrial fibrillation risk in cancer survivors.
The association weakens after adjusting for lifestyle factors but remains suggestive.
The link is stronger in cancer survivors not receiving radiotherapy.
Abstract
Cancer survivors (CSs) are at increased risk of atrial fibrillation (AF), potentially due to cancer-related inflammation and treatment effects. While inflammation has been implicated in both cancer and AF, the association between C-reactive protein (CRP) and AF risk in CSs remains unclear. We analyzed data from 19,677 UK Biobank participants (mean age 60; 34.2% male) with a prior cancer diagnosis. Incident AF was evaluated using competing-risk Cox proportional hazards models, adjusting for sociodemographic, lifestyle, and clinical factors. Over a median follow-up of 10.4 years, 836 CSs (4.2%) developed AF. Competing risk analysis revealed that the significant association between elevated CRP (> 2 mg/L) and AF risk in CSs, observed in models adjusted for sociodemographic and clinical factors (HR 1.21, 95% CI 1.06–1.37; P = 0.005), progressively attenuated with further adjustment for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
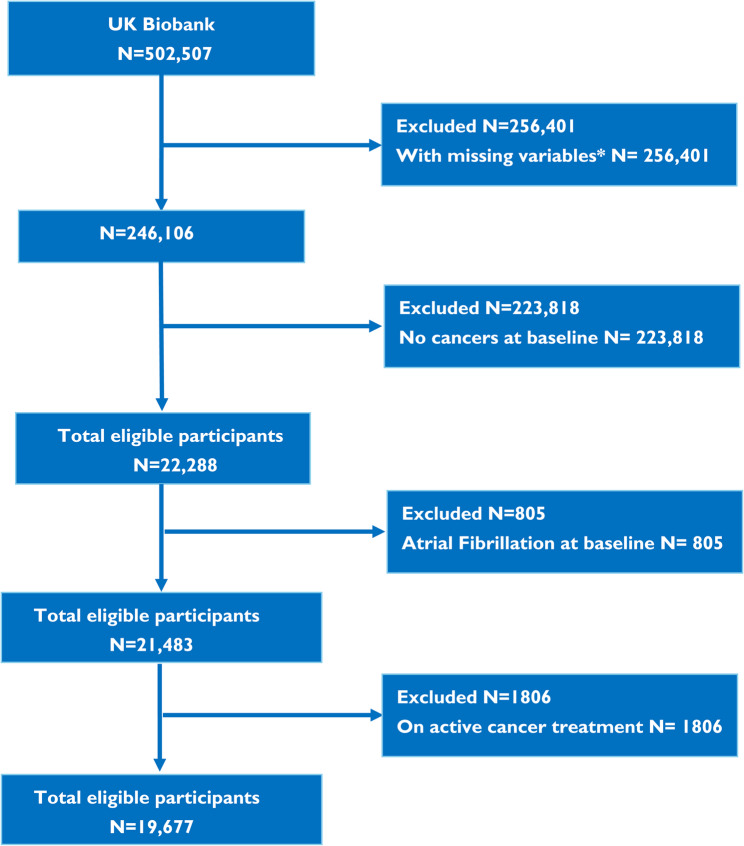 Figure 1
Figure 1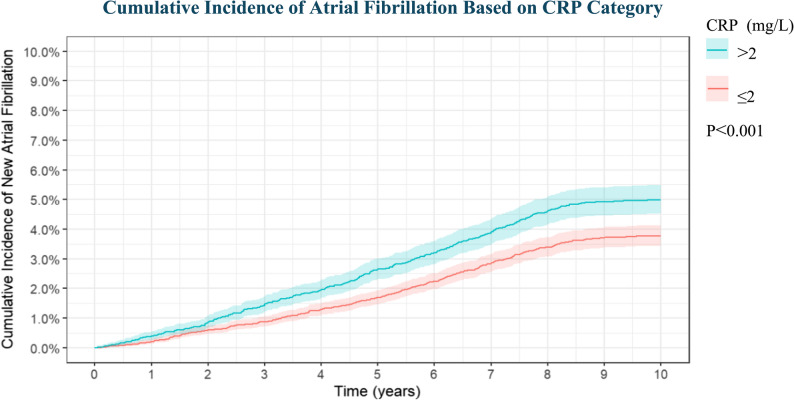 Figure 2
Figure 2- —Shenzhen Clinical Research Center for Rare Diseases
- —https://doi.org/10.13039/501100012151Sanming Project of Medicine in Shenzen Municipality
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Biomarkers in Disease Prognosis · Atrial Fibrillation Management and Outcomes · Adipokines, Inflammation, and Metabolic Diseases
Introduction
The landscape of cancer treatment has evolved, resulting in more individuals surviving cancer diagnoses [1–3]. However, this progress has brought to light the heightened cardiovascular risks faced by cancer survivors(CSs), attributed to cancer-related inflammation and combined treatments [4–6]. Surprisingly, the risk of cardiovascular mortality in these survivors surpasses that of cancer itself [7, 8]. Atrial fibrillation (AF) emerges as a prevalent cardiovascular condition affecting 33 million individuals worldwide, with a prevalence ranging from 2 to 4% and projected to rise in the coming years [9, 10]. Notably, about 20% of cancer patients experience AF as a comorbidity [11], underscoring the substantial disease burden. The field of cardio-oncology aims to prevent and manage cancer therapy-related cardiovascular toxicity(CTR-CVT), emphasizing the integration of cancer care with cardiovascular health outcomes [12]. Nevertheless, the lack of easily identifiable and reproducible biomarkers to identify high-risk populations before AF onset poses a significant challenge [11].
Various studies have demonstrated inflammation as a common thread between cancer and AF, correlating with the development of both conditions [4, 13–16]. The higher prevalence of AF among cancer patients can be attributed to systemic inflammation triggered by malignancy, fostering atrial structural changes that pave the way for AF [14, 15]. This notion finds support in the elevated levels of inflammatory markers observed in cancer patients, including C-reactive protein (CRP), tumor necrosis factor α (TNF-α), and interleukins 2, 6, and 8[14], all linked to increased arrhythmic susceptibility. Despite these insights, no study has specifically examined the association between CRP and new-onset AF in CSs.
Methods
Study population
The research was conducted within the UK Biobank, encompassing over 500,000 individuals aged between 40 and 69 from diverse regions of the UK. Initially, detailed information on participant demographics, lifestyle factors, health history, physical measurements, and blood samples was collected. Health outcomes were linked to Hospital Episode Statistics (HES) and mortality records, categorized according to standardised International Classification of Diseases (ICD) codes.
Among the UK Biobank participants, 41,867 individuals had a prior history of cancer. Those with incomplete data, study withdrawal, concurrent AF at the beginning and who received radiotherapy or chemotherapy after enrolment were excluded, resulting in a final group of 19,677 CSs (Fig. 1). The UK Biobank study received approval from the North West Multicentre Research Ethics Committee. All participants provided informed consent during their initial visit to the assessment center. The UK Biobank project number for this study was 97,089.Fig. 1. Flow diagram of the study population. *Missing variables include age, gender, race, education, body mass index, waist circumference, number of times per week consuming processed meats, number of times per day consuming fruit or vegetables, smoking history, C-reactive protein, antihypertensive medication, diabetes medication and statins
Covariables and outcomes
Extensive review of established evidence was conducted to identify the factors influencing the relationship between CRP and AF in CSs [12, 16]. Various variables were extracted from the baseline assessment data of participants, covering sociodemographic factors such as age, gender, race, and educational attainment (college or university). Lifestyle factors examined included body mass index (BMI), waist circumference, smoking habits, alcohol consumption, dietary preferences, and frequency of moderate-intensity physical activity exceeding 10 min per week. Additionally, clinical aspects like CRP levels, confirmed diabetes mellitus, hypertension, history of coronary artery disease(CAD), heart failure(HF), ischemic stroke, chemotherapy, radiotherapy and the usage of medications for hypertension, diabetes, or statins were also considered.
Specific cutoff values were applied for key variables, with age limited to 65 years, BMI capped at 30 kg/m^2^, and waist circumference set at 90 cm. CRP levels were standardized at 2 mg/L, in alignment with insights from prior clinical research and the definition of residual inflammatory risk [17–19].
All-cause mortality and AF-related death outcomes were determined from death registry data, while new-onset AF events were classified according to ICD-10 codes (Table S1). The mean follow-up period for HES and mortality data amounted to 10.4 ± 1.5 years (IQR 9.8–11.3 years). For detailed information on each covariate, measurement techniques, and the programming codes used for covariate computation, please consult Table S1.
Statistical analysis
The data analysis was conducted utilizing appropriate statistical methods. Normally distributed continuous variables were represented as mean ± standard deviation (SD), while non-normally distributed continuous variables were presented as median and interquartile range (IQR). Categorical variables were expressed as counts and percentages. Variances between groups were evaluated using Pearson’s chi-square test. The primary outcome of the study was the occurrence of AF, with non-AF-related death considered as a competing risk.
Participant characteristics were detailed in counts and percentages, with group variations assessed using the Pearson’s chi-square test. Initial univariate analyses were carried out, followed by the plotting of Cumulative Incidence Function (CIF) curves to visualize changes in AF incidence over time. The Fine-Gray test was employed to compare differences between groups. Subsequently, independent risk factors for AF development were explored using competing risk regression with Cox proportional hazards models. Interaction effects on both multiplicative and additive scale were analyzed through the likelihood ratio test and calculations of relative excess risk due to interaction.
A two-sided P-value of 0.05 was applied for determining statistical significance. All statistical computations were executed using R version 4.4.2 and R Studio Version 1.4.1717.
Results
Participant characteristics
The participants’ characteristics are provided in Table 1.
Table 1. Participant characteristicsCRP ≤ 2 mg/LCRP > 2 mg/LP-valueNumber, n (%)11,826(60.1%)7851(39.9%)Socio-demographicsAge, years59.6 ± 7.260.2 ± 6.9< 0.001Gender Female7692(65.0%)5254(66.9%)0.007 Male4134(35.0%)2597(33.1%)Race White11,546(97.6%)7653(97.5%)0.659 Asian78(0.7%)64(0.8%) Black79(0.7%)53(0.7%) Mixed or other123(1.0%)81(1%)College or university degree No7770(65.7%)5925(75.5%)< 0.001 Yes4056(34.3%)1926(24.5%)Lifestyle characteristics BMI26.1 ± 4.029.5 ± 5.4< 0.001 Waist circumference86.4 ± 12.494.7 ± 13.4< 0.001Number of times per week consuming processed meats None1334(11.3%)607(7.7%)< 0.001 1 ~ 310,137(85.7%)6973(88.8%) 4+355(3.0%)271(3.5%)Number of times per day consuming fruit or vegetables None415(3.5%)378(4.8%)< 0.001 1 ~ 25050(42.7%)3484(44.4%) 3 ~ 45083(43.0%)3222(41.0%) 5+1278(10.8%)767(9.8%)Alcohol consumption Daily or almost daily2696(22.8%)1430(18.2%)< 0.001 Three or four times a week2766(23.4%)1472(18.7%) Once or twice a week2968(25.1%)1979(25.2%) One to three times a month1206(10.2%)940(12.0%) Special occasions only1333(11.3%)1236(15.7%) Never857(7.2%)794(10.1%) Smoke7221(61.1%)5129(65.3%)< 0.001Days per week spent doing moderate physical activity > 10 min None1364(11.5%)1344(17.1%)< 0.001 1 ~ 22578(21.8%)1687(21.5%) 3 ~ 77484(66.7%)4820(61.4%)Clinical characteristics C-reactive protein, mg/L0.9(0.5–1.3)3.9(2.7–6.6)<0.001 Hypertension3705(31.3%)3186(40.6%)< 0.001 Diabetes647(5.5%)600(7.6%)< 0.001 Coronary artery disease572(4.8%)379(4.8%)1 Heart failure7(0.1%)16(0.2%)0.007 Ischemic stroke258(2.2%)212(2.7%)0.022 On antihypertensive medication2397 (20.3%)1888(24.0%)< 0.001 On statin2418(20.4%)1505(19.2%)0.029 On diabetes medication378(3.2%)326(4.2%)< 0.001 Chemotherapy1223(10.3%)1109(14.1%)< 0.001 Radiotherapy287(2.4%)229(2.9%)0.039
The group with CRP level > 2 mg/L accounted for 39.9% of the participants. The mean age of this group was 60.2 (± 6.9) years, while the mean age of the CRP ≤ 2 mg/L group was slightly lower at 59.6(± 7.2) years. The proportion of male participants was higher in the CRP ≤ 2 mg/L group, constituting 35.0% of the total participants (n = 4,134). Moreover, the CRP ≤ 2 mg/L group exhibited a higher level of educational accomplishment. The CRP > 2 mg/L group displayed more unhealthy lifestyle traits, including obesity, increased consumption of processed meats, lower intake of fruits and vegetables, lack of physical activity, and a higher prevalence of smoking. Additionally, this group had a higher incidence of comorbidities such as hypertension, diabetes mellitus, HF, and ischemic stroke, with a larger percentage of individuals taking medications for hypertension and diabetes. Moreover, a higher proportion had undergone prior radiotherapy and chemotherapy. Conversely, the CRP ≤ 2 mg/L group had higher rates of alcohol consumption and statin usage.
Over a mean follow-up period of 10.4 ± 1.5 years, 836 cases of AF were documented, resulting in an incidence rate of 4.25 per 100 individuals. Among these cases, 391 (4.98 per 100 individuals) were observed in the CRP > 2 mg/L group, while 445 (3.76 per 100 individuals) occurred in the CRP ≤ 2 mg/L group. The incidence of AF was higher in the CRP > 2 mg/L group compared to the CRP ≤ 2 mg/L group. During follow-up, there were 1,422 all-cause deaths, with AF accounting for only two cases.
Correlates of new-onset AF in CSs
The analysis conducted to identify independent risk factors for AF in CSs utilized multivariable analyses with competing risk regression and Cox proportional hazards model, presented in Tables 2, 3 and 4. The results revealed several factors significantly correlated with the development of AF within this specific population. The multivariable analysis underscored that factors associated with AF in CSs comprised age ≥ 65 years (HR 2.20, 95% CI 1.90–2.55; P < 0.001), male gender (HR 1.73, 95% CI 1.46–2.05; P < 0.001), BMI ≥ 30 kg/m^2^ (HR 1.34, 95% CI 1.14–1.58; P < 0.001) and waist circumference ≥ 90 cm (HR 1.24, 95% CI 1.03–1. 50; P = 0.025), as shown in Tables 2, 3 and 4. Additionally, factors such as a history of CAD (HR 1.74, 95% CI 1.39–2.17; P < 0.001), a history of HF (HR 3.66, 95% CI 1.48–9.02; P = 0.005), use of antihypertensive medication (HR 1.44, 95% CI 1.19–1.75; P < 0.001) and previous chemotherapy (HR 1.24, 95% CI 1.01–1.53; P = 0.043) were also significantly associated with the occurrence of AF in the studied population as indicated in Tables 2, 3 and 4. However, engaging in moderate physical activity exceeding 10 min 1–2 days per week and a higher education level were associated with a reduced incidence of AF, with hazard ratios of 0.78 (95% CI 0.63–0.96; P = 0.019) and 0.84 (95% CI 0.71–0.99; P = 0.035), respectively (Table 4).
Table 2. Associations between CRP and AF in CSs in model 1VariablessHR95%CIP-valueSocio-demographicsAge < 65, yearsReference ≥65, years2.332.03–2.67< 0.001Gender FemaleReference Male2.191.90–2.51< 0.001Race WhiteReference Asian0.530.17–1.630.27 Black0.510.16–1.610.25 Mixed or other races1.240.66–2.330.50College or university degree NoReference Yes0.770.65–0.900.001C-reactive protein, mg/L ≤2Reference >21.301.14–1.49< 0.001
Table 3. Associations between CRP and AF in CSs in model 2VariablessHR95%CIP-valueSocio-demographicsAge < 65, yearsReference ≥65, years2.131.85–2.46< 0.001Gender FemaleReference Male1.911.66–2.21< 0.001Ethnic WhiteReference Asian0.480.16–1.440.19 Black0.470.15–1.460.19 Mixed or other races1.290.69–2.420.43College or university degree NoReference Yes0.810.69–0.950.011Clinical characteristicsC-reactive protein, mg/L ≤2Reference >21.211.06–1.370.005Diabetes NoReference Yes0.990.69–1.420.97Hypertension NoReference Yes1.241.03–1.480.02Coronary artery disease NoReference Yes1.781.43–2.23< 0.001Heart failure NoReference Yes3.571.42–8.990.007Ischemic stroke NoReference Yes1.290.92–1.800.14On antihypertensive medication NoReference Yes1.441.19–1.75< 0.001On diabetes medication NoReference Yes1.030.66–1.610.89On statin NoReference Yes1.020.86–1.210.80Chemotherapy NoReference Yes1.241.01–1.530.04Radiotherapy NoReference Yes1.050.69–1.580.83
Table 4. Associations between CRP and AF in CSs in model 3VariablessHR95%CIP-valueSocio-demographicsAge < 65, yearsReference ≥65, years2.201.90–2.55< 0.001Gender FemaleReference Male1.731.46–2.05< 0.001Ethnic WhiteReference Asian0.500.17–1.510.22 Black0.460.15–1.430.18 Mixed or other races1.270.67–2.410.47College or university degree NoReference Yes0.840.71–0.990.035Lifestyle characteristicsBMI <30 kg/m^2^Reference ≥30 kg/m^2^1.341.14–1.58< 0.001Waist circumference <90 cmReference ≥90 cm1.241.03–1.500.025Number of times per week consuming processed meats NoneReference 1 ~ 30.910.70–1.180.46 4+0.830.54–1.270.40Number of times per day consuming fruit or vegetables NoneReference 1 ~ 20.830.59–1.150.26 3 ~ 40.810.58–1.120.21 5+0.940.65–1.360.74Alcohol consumption Daily or almost dailyReference Three or four times a week0.930.76–1.150.52 Once or twice a week0.960.78–1.170.66 One to three times a month0.960.74–1.250.77 Special occasions only0.850.66–1.100.21 Never0.980.74–1.300.88Smoke NoReference Yes1.140.98–1.330.1Days per week spent doing moderate physical activity > 10 min NoneReference 1 ~ 20.800.63–1.000.05 3 ~ 70.870.72–1.050.15Clinical characteristicsC-reactive protein, mg/L ≤2Reference >21.140.99–1.310.076Diabetes NoReference Yes0.920.64–1.320.65Hypertension NoReference Yes1.170.97–1.400.10Coronary artery disease NoReference Yes1.741.39–2.17< 0.001Heart failure NoReference Yes3.661.48–9.020.005Ischemic stroke NoReference Yes1.270.91–1.770.16On antihypertensive medication NoReference Yes1.441.19–1.75< 0.001On diabetes medication NoReference Yes0.990.63–1.550.97On statin NoReference Yes1.000.84–1.180.96Chemotherapy NoReference Yes1.241.01–1.530.043Radiotherapy NoReference Yes1.030.68–1.560.88
Given the propensity for hypertensive medications to potentially contribute to the new-onset AF, an in-depth examination into the baseline characteristics of individuals taking such medications was undertaken (Table S2). The findings revealed that these individuals, predominantly older males with lower levels of education, exhibited habits such consuming processed meats, frequent alcohol intake, smoking, physical inactivity and higher level of CRP. Additionally, they presented common comorbidities including obesity, hypertension, diabetes mellitus, CAD, HF and ischemic stroke. Furthermore, they were more inclined to be prescribed diabetes medications and statins, indicating a pattern of interconnected health issues among them.
Association of CRP with new-onset AF in CSs
In our investigation, a univariable competing risks model was utilized to assess to the cumulative incidence of AF in relation to CRP > 2 mg/L. The findings illustrated in Fig. 2 displayed a substantial correlation between elevated CRP levels and an heightened cumulative risk of AF. To delve deeper into the independent relationship between CRP levels and AF, a multivariable competing risk model was constructed. In Model 1 (sociodemographics only), CRP levels > 2 mg/L independently predicted incident AF (HR 1.30, 95% CI 1.14–1.49, P < 0.001) (Table 2). The association remained robust after additional adjustment for clinical covariates in Model 2 (HR 1.21, 95% CI 1.06–1.37; P = 0.005) (Table 3). Further inclusion of lifestyle factors in Model 3 attenuated the effect, yet CRP > 2 mg/L retained a borderline significant trend (HR 1.14, 95% CI 0.99–1.31, P = 0.076) (Table 4).Fig. 2. Cumulative Incidence of Atrial Fibrillation Based on CRP Category. CRP, C-reactive protein. AF, atrial fibrillation. CSs, cancer survivors. P-values were calculated between each exposure group and the cumulative incidence of new-onset atrial fibrillation using the Fine-Gray test, accounting for competing risks of non-AF-related mortality
Among eight common cancer subtypes, we analyzed the relationship between CRP levels and the incidence of new-onset AF. The results showed a trend toward increased AF incidence with elevated CRP levels across most cancer types, with the exception of lymphoma. However, this association did not reach statistical significance (Table S3).
Subgroup analyses
In the subgroup analysis documented in Table 5, a detailed exploration was conducted into the potential interaction between CRP levels > 2 mg/L and the risk of AF in various subgroups of CSs. The findings indicated that that inflammation, signaled by CRP > 2 mg/L, amplified the susceptibility to AF independently of variables such age, gender, BMI, waist circumference, smoking, diabetes or hypertension status, history of CAD and HF, the use of medications for hypertension or statins, or prior chemotherapy—without evidence of effect modification (all P for interaction > 0.05) (Table 5). Essentially, the adverse impacts of inflammation remained uniform across the described subgroups of CSs, demonstrating consistency rather than variation based on these specific attributes. Furthermore, the influence of inflammation on AF was more pronounced in CSs who had not received radiotherapy (P for interaction = 0.032), suggesting that the absence of prior radiation may amplify the arrhythmogenic impact of inflammation.
Table 5. Subgroup analysis of CRP levels and the risk of AF occurrence in CSsStratified variablesHR (95% CI)P valueP for interactionNumberPercentCRP ≤ 2 mg/LCRP > 2 mg/LOverall19,67710011.33(1.16–1.53)< 0.001Age, years0.126 <6513,62569.211.46(1.20–1.78)< 0.001 ≥65605230.811.18(0.98–1.42)0.082Gender0.193 Female12,94665.811.50(1.23–1.84)< 0.001 Male673134.211.25(1.04–1.50)0.017BMI0.742 <3014,80075.211.19(1.00–1.42)0.055 ≥30487724.811.13(0.89–1.44)0.316Waist circumference 0.617 < 90 cm10,12451.511.16(0.90–1.50)0.261 ≥ 90 cm955348.511.07(0.91–1.27)0.404Smoke0.762 No732737.211.36(1.06–1.74)0.014 Yes12,35062.811.30(1.10–1.53)0.002Diabetes0.895 No18,43093.711.31(1.14–1.52)< 0.001 Yes12476.311.35(0.88–2.09)0.17Hypertension0.50 No12,78665.011.31(1.08–1.60)0.007 Yes689135.011.19(0.99–1.44)0.067Coronary artery disease0.314 No18,72695.211.37(1.19–1.59)< 0.001 Yes9514.811.11(0.76–1.63)0.583Heart failure0.389 No19,65499.911.33(1.16–1.53)< 0.001 Yes230.110.62(0.10–3.75)0.607On antihypertensive medication0.069 No15,39278.211.42(1.19–1.69)< 0.001 Yes428521.811.10(0.88–1.36)0.399On statin0.768 No15,75480.111.33(1.13–1.57)0.001 Yes392319.911.39(1.09–1.77)0.008Chemotherapy0.884 No17,34588.111.33(1.15–1.53)< 0.001 Yes233211.911.37(0.93–2.00)0.108Radiotherapy0.03 No19,16197.411.37(1.19–1.57)< 0.001 Yes5162.610.51(0.21–1.23)0.136
Discussion
In our comprehensive study involving 19,677 individuals with a cancer history, we conducted the first extensive systematic investigation into the relationship between CRP levels and the incidence of AF. The results revealed a notable correlation, indicating that CRP > 2 mg/L were associated with increased risk of developing AF in this population. This risk was particularly prominent among individuals who had not received radiotherapy.
Furthermore, our research highlighted the prevalence comorbidities among CSs. Those with CRP > 2 mg/L exhibited a higher likelihood of various conditions such as advanced age, obesity, smoking, lack of exercise, diabetes, hypertension, CAD, and HF, all of which are known to elevate the risk of AF [20]. Additionally, traditional risk factors like advanced age, obesity, smoking, lack of exercise, CAD, and HF were found to significantly increase the risk of AF. Crucially, multivariable adjustment demonstrates that the relationship between systemic inflammation and new-onset AF persists after accounting for these conventional determinants, underscoring inflammation as an important pathophysiological driver in the CSs. Nevertheless, incorporation of lifestyle variables attenuates the magnitude of the CRP–AF association, implying that health-behaviour pathways may partially mediate or confound the inflammatory signal. These findings highlight the need to target both biological and behavioural axes when stratifying and mitigating AF risk in CSs.
An intriguing observation from our study was the link between the use of hypertensive medications and an increased risk of AF. This association may stem from individuals on such medications having a higher predisposition to AF due to multiple risk factors.
Our study unveiled a substantial and independent association between systemic inflammation and an increased risk of AF in CSs, aligning with some, but not all, previous studies in this area.
CRP serves as a straightforward and reliable indicator of systemic inflammation. Our research illustrates that individuals with CRP >2 mg/L were more likely to present with comorbid risk factors for AF such as obesity, hypertension, diabetes mellitus, and HF[20]. Moreover, elevated CRP levels were independently associated with a higher incidence of AF, regardless of these conventional risk factors. Recent large cohort studies have highlighted a strong link between CRP and AF development [21–26], leading to its recognition as a biomarker in predicting AF in the 2024 ESC guidelines [20].
The evolving understanding of the relationship between inflammation and AF risk has spurred investigations into the potential benefits of anti-inflammatory interventions in AF prevention and treatment. Various studies have explored anti-inflammatory therapies targeting AF, with some showing promising outcomes [15, 27–29]. For instance, recent findings demonstrated that steroid therapy reduced the risk of postoperative AF in a canine model [30] and may aid in reducing AF recurrence after catheter ablation in the clinical setting [31]. Although some anti-inflammatory strategies, like colchicine [32, 33] and statins [34, 35], have shown effectiveness in specific contexts, our study revealed that statin administration did not decrease new-onset AF events in CSs. Additionally, recent randomized controlled trials investigating colchicine administration did not show a significant decrease in the incidence of clinically significant AF in patients undergoing major noncardiac thoracic surgery [36]. The variations in trial outcomes could be attributed to several factors including participant demographics, follow-up duration, protocol discontinuation rates, and potential differences in targeted inflammatory pathways. Despite the ongoing exploration of anti-inflammatory interventions for AF management, the latest ESC guidelines do not endorse these strategies as standard practice due to the mixed results observed in clinical trials [19]. This underscores the crucial need for further research to uncover the precise role of inflammation and evaluate the impact of anti-inflammatory interventions on AF outcomes.
In cancer patients, inflammatory markers like CRP, TNF-α, and interleukins are commonly elevated [14], reflecting an inflammatory state [20]. Our study observed that a significant percentage of CSs had CRP >2 mg/L, indicating chronic low-grade inflammation [17, 18 ]. The onset of AF in cancer settings may result from comorbid conditions, direct tumor effects, treatment complications, or shared inflammatory processes [4]. There is a notion that AF could potentially be an inflammatory complication of cancer [37]. Several systematic reviews have also highlighted the link between inflammation and AF development in cancer patients [4, 16, 38, 39], yet no study has specifically examined the correlation between CRP and new-onset AF in CSs. Our findings strongly suggest that low-grade inflammation, as indicated by CRP levels, is a key independent risk factor for AF development in CSs. This emphasizes the potential of utilizing CRP as a biomarker for monitoring CTR-CVT and implementing anti-inflammatory interventions to reduce AF risk in this vulnerable population.
The specific mechanisms through which inflammation heightens the risk of AF in CSs remain incompletely understood. However, drawing on previous research, several potential mechanisms can be hypothesized.
Cancer patients with chronic low-grade inflammation often present with traditional risk factors for AF such as obesity, hypertension, CAD and HF [39]. Treatments like anticancer drugs, radiation therapy, and surgery can initiate AF through inflammatory pathways [4]. Interestingly, early histologic studies have indicated that even in individuals with “isolated AF,” around two-thirds of patients showcase localized atrial inflammatory infiltrates akin to myocarditis [40]. The inflammatory response mediators have the potential to impact atrial electrophysiology and structural substrates, thereby increasing susceptibility to AF [41]. Inflammation can also modulate calcium homeostasis and connexins, which play a role in AF triggers and the heterogeneous conduction of the atria [41]. Moreover, the relationship between AF and inflammation is bidirectional, as AF itself can exacerbate inflammation, leading to the phenomenon known as ‘AF begets AF’ [41]. Furthermore, inflammation has been linked to expediting the aging process and fostering the clonal expansion of cells in normal tissues, including blood cells [42]. Recent research have unveiled that clonal hematopoiesis of indeterminate potential (CHIP) serves as a risk factor for both cancer [43–45] and AF [45, 46]. Continued investigation is imperative to fully uncover the potential mechanisms through which inflammation heightens the risk of AF in CSs. This deeper comprehension will facilitate the development of targeted interventions to mitigate AF risk in this specific population.
Strengths and limitations
Our research possesses several notable strengths that enhance its effectiveness and reliability. A key advantage lies in the utilization of the extensive and well-established UK Biobank database, providing robust and detailed measurements of various exposure factors. The database’s long-term and rigorous follow-up procedures help mitigate common biases prevalent in observational studies, such as selection, recall, and information bias. Furthermore, our study considered the traditional risk factors for AF in CSs. By incorporating a comprehensive evaluation of common AF risk factors and treatment medications in our analysis, we aimed to address potential confounding variables. Notably, our findings suggest that the detrimental impact of elevated CRP levels on new-onset AF in CSs remains significant independent of baseline traditional risk factors. This indicates the potential universal applicability of CRP as a predictive biomarker for AF across a broader population of CSs.
It is essential to acknowledge the limitations of our study, despite its strengths. One significant limitation was the limited statistical power, which restricts the ability to perform robust analyses—particularly due to small sample sizes within individual cancer subtypes, the presence of variables with only one level, and the absence of detailed radiotherapy and chemotherapy regimens. Additionally, the study focused mainly on Caucasian participants, restricting the generalizability of the results to other racial groups. These limitations should be considered when interpreting our findings, highlighting the necessity for further research to bridge these knowledge gaps and ensure inclusivity across diverse populations.
Conclusion
Our findings suggest that systemic inflammation is associated with an increased risk of AFamong CSs,. particularly in individuals without a history of radiotherapy. Further studies are needed to explore underlying mechanisms and therapeutic implications.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jemal A, Ward EM, Johnson CJ, Cronin KA, Ma J, Ryerson AB, Mariotto A, Lake AJ, Wilson R, Sherman RL, Anderson RN, Henley SJ, Kohler BA, Penberthy L, Feuer EJ, Weir HK. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. JNCI: Journal of the National Cancer Institute. 2017;109(9).10.1093/jnci/djx 030PMC 540914028376154 · doi ↗ · pubmed ↗
- 2Kirchhof P, Lip GY, Van Gelder IC, Bax J, Hylek E, Kaab S, Schotten U, Wegscheider K, Boriani G, Brandes A, Ezekowitz M, Diener H, Haegeli L, Heidbuchel H, Lane D, Mont L, Willems S, Dorian P, Aunes-Jansson M, Blomstrom-Lundqvist C, Borentain M, Breitenstein S, Brueckmann M, Cater N, Clemens A, Dobrev D, Dubner S, Edvardsson NG, Friberg L, Goette A, Gulizia M, Hatala R, Horwood J, Szumowski L, Kappenberger L, Kautzner J, Leute A, Lobban T, Meyer R, Millerhagen J, Morgan J, Muenzel F, Nabauer M, · doi ↗ · pubmed ↗