Acceptability and preferences for dual-active ingredient long-lasting insecticidal nets in rural Tanzania: a mixed-methods study
Eliud Andrea Lukole, Stacie Gobin, Jackie Cook, Jacques Derek Charlwood, Jacklin F. Mosha, Nancy S. Matowo, Elizabeth Mallya, Tatu Aziz, Justina V. Mosha, Jacklin Martin, Mark Rowland, Immo Kleinschmidt, Alphaxard Manjurano, Franklin W. Mosha, Jayne Webster, Natacha Protopopoff

TL;DR
This study explores how people in rural Tanzania accept and prefer different types of insecticide-treated mosquito nets to combat malaria.
Contribution
The study provides community-informed insights into LLIN acceptability and preferences, which can guide future malaria prevention strategies.
Findings
Olyset Plus was slightly favored over Olyset Net in Muleba due to perceived stronger insecticide effects.
In Misungwi, polyester nets were preferred over polyethylene due to better comfort and durability.
Adverse effects like skin irritation were reported more frequently for certain net types.
Abstract
The World Health Organization (WHO) recommends dual-active ingredient long-lasting insecticidal nets (dual-AI LLINs) for protection against malaria in areas with insecticide resistance. The effectiveness of LLINs, however, depends on user compliance, influenced by community perceptions of malaria, prevention methods, and the acceptability of LLINs. Understanding these factors is essential for the success of large-scale implementation. This study was part of the two cluster-randomized controlled trials (RCTs) evaluating the efficacy of dual-AI LLINs on malaria indicators in Muleba and Misungwi districts, Tanzania. Polyethylene and polyester rectangular LLINs were distributed in Muleba (Olyset Plus and Olyset Net) in 2015 and in Misungwi (Olyset Plus, Royal Guard, Interceptor G2, and Interceptor) in 2019. A mixed-methods approach was used to assess users’ acceptability, preferences, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
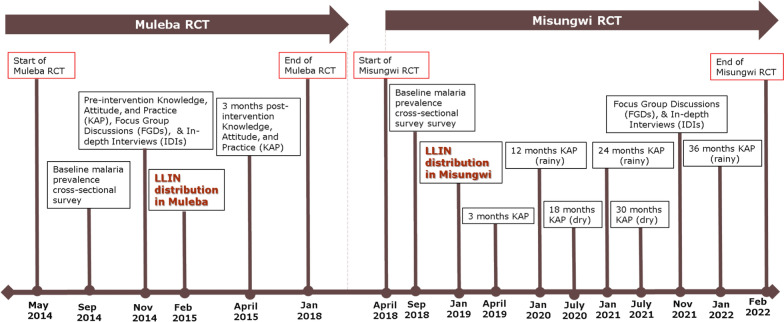 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3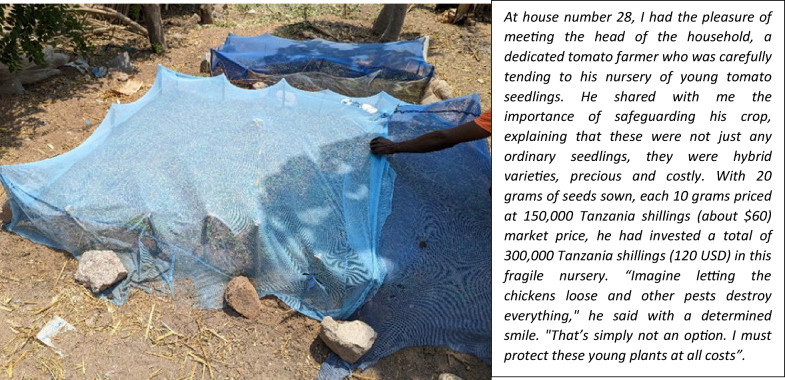 Figure 4
Figure 4- —https://doi.org/10.13039/501100000265Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · ICT in Developing Communities · Mosquito-borne diseases and control
Background
Malaria caused approximately 597,000deaths globally in 2024 [1]. Tanzania is among the four countries with the highest malaria deaths accounting for 4.4% of the global deaths in 2024 [1]. Malaria is highest in the Lake Victoria zone, with the districts of Muleba and Misungwi having an annual incidence rate of 130.9, and 24.3 cases per 1000 population in 2023, respectively [2, 3]. Malaria has a profound economic and social impact, contributing to human suffering and limiting development [4, 5]. Countries with high malaria transmission have been shown to have income levels about one-third lower than those without malaria. Indeed, countries that have eliminated malaria have typically experienced substantially higher economic growth in the following 5 years [6]. LLINs, primarily treated with pyrethroids, have been the cornerstone of malaria prevention for decades [7, 8]. Acceptability of pyrethroid-only long-lasting insecticidal nets (LLIN) has generally been high over the last few decades, with studies suggesting this is due to their perceived effectiveness [9–11]. However, growing resistance to pyrethroid insecticides has reduced the effectiveness of these nets, which may, in turn, impact their acceptability.
In 2017, the World Health Organization (WHO) recommended the deployment of novel LLINs combining a pyrethroid with a synergist piperonyl butoxide (PBO) [12]. In 2023, the WHO further endorsed LLINs with dual active ingredient treated with pyrethroid, with either pyriproxyfen or chlorfenapyr [13] to control malaria-transmitted by insecticide-resistant vectors. In that same year, 360 million pyrethroid-piperonyl butoxide (PBO) LLINs, and 74 million dual active ingredient LLINs were distributed across sub-Saharan Africa (SSA), including Tanzania [1, 14], with the number increasing to 82 million in the second quarter of 2025. Between 2018 and 2025, the proportion of dual-active ingredient long-lasting insecticidal nets (dual-AI LLINs) including PBO LLINs distributed in SSA increased from 3 to 84% of all LLINs distributed [14]. Following the WHO recommendations, the Tanzanian National Malaria Control Programme (NMCP), with the support of the President’s Malaria Initiative (PMI), and Global Fund (GF), has distributed over 2,945,181 PBO LLINs by 2024 [15, 16]. NMCP is also considering the deployment of dual-AI LLIN, such as Interceptor G2, for future LLIN campaigns [16].
Previous studies in Tanzania have examined LLIN user’s attitude [17–20]. Nuisance from mosquito bites was identified as the main factor influencing consistent use. Individuals who used LLINs primarily for malaria protection were more likely to adhere than those who used them mainly to prevent mosquito-biting nuisance especially when mosquito density was low. Hot weather was also to be a major deterrent to LLIN use [21]. While mosquito net manufacturers aim to improve ventilation by enlarging the mesh size, they are constrained by the need to keep the openings small enough to block mosquitoes [22]. Various characteristics of LLINs brands such as durability, texture, mesh size, net size, shape, colour, and insecticidal effectiveness have been found to influence acceptability and usage [9]. The net material also influences user preference and durability. Studies in Kenya [23], India, and Nepal [24] found users preference leaning towards polyester have a softer texture. In contrast polyethylene have a stiffer texture, shrink after washing (making them difficult to tuck under bedding), and have larger mesh sizes which are perceived as allowing mosquito entry. Conversely, a study in Uganda [25] found a slight preference for polyethylene LLINs over polyester. These findings highlight the importance of determining community preferences before procuring LLINs.
A key challenge for malaria control in SSA is not only achieving sufficient LLIN coverage but also addressing the behavioural factors that affect their use. Providing LLINs that are acceptable to users can improve adherence and, ultimately, contribute to the success of malaria control programmes. To address this operational priority, two studies, embedded within cluster–cluster-randomized controlled trials (RCTs), were conducted to assess acceptability and preferences for five types of LLINs with different textiles and insecticidal properties and, to identify barriers to appropriate use.
Methods
Study design
This mixed-method study was part of a two large cluster-randomized controlled trials (RCTs) (Table 1) conducted in Muleba and Misungwi districts. The RCTs aimed to assess the epidemiological and entomological efficacy of different types of dual-AI LLINs against malaria transmitted by resistant mosquitoes [26–28]. In Muleba, the quantitative component of the study included knowledge, attitudes, and practices (KAP) surveys pre- and post-intervention, and a qualitative study pre-intervention (Fig. 1). In Misungwi, KAP questions were included in a survey 3 months post-intervention and in malaria prevalence surveys at 12, 18, 24, 30, and 36 months post-intervention; qualitative data was collected 34 months post-intervention only (Fig. 1). Table 1RCTs in Muleba and Misungwi districtsRCTsMuleba RCT: March 2014–December 2017Misungwi RCT: April 2018–March 2022Study designA four-arm, factorial design, cluster-randomized trial (CRT) with 48 clusters (12 clusters per arm) and village/hamlet as the unit of randomization. Each cluster was comprised of 1–6 hamlets (sub-village) with up to 450 houses per clusterThe four arms/interventions were:1. Olyset Plus (permethrin + piperonyl butoxide (PBO) LLIN)2. Olyset Plus + Indoor Residual Spraying (IRS) with pirimiphos-methyl applied at a dosage of 1–2 g AI/m^2^, provides a residual effect lasting 6–9 months3. Olyset net + IRS4. Olyset net [control/reference arm]: (permethrin only LLIN)A four-arm, superiority design, single-blinded, cluster-randomized trial with 84 clusters (21 clusters per arm) with village/hamlet as the unit of randomization. Each cluster was comprised of 1–8 hamlets (sub-village) of between 150–450 houses in the core area of a clusterThe four arms/interventions were:1. Interceptor G2 (alpha-cypermethrin + chlorfenapyr)2. Royal Guard (alpha-cypermethrin + pyriproxyfen)3. Olyset Plus (permethrin + piperonyl-butoxide (PBO))4. Interceptor [control/reference arm]: (alpha-cypermethrin)LLIN distributionLLINs were distributed from 6th-8th February 2015, and Indoor residual spraying (IRS) took place once in February/March 2015. Approximately 90,000 LLINs were distributed in 30,000 households, with each arm receiving only one type of netLLINs were distributed from 26th-28th January 2019. A total of 147,230 LLINs were distributed in 42,394 households, with each arm receiving only one type of netLLIN fabric, colour, shape, and size of distributed LLINsPolyethylene material, blue in colour, and rectangular in shape (length 180 cm, Height 180 cm, and Width 160 cm)Polyethylene (Olyset Plus and Royal Guard), polyester (Interceptor G2 and Interceptor), all blue, and rectangular (length 180 cm, Height 180 cm, and Width 160 cm)Fig. 1KAP, FGDs, and IDIs data collection timeline
Study sites, and setting
Muleba is the largest district of the Kagera region, located in the northwest of Tanzania on the western shore of Lake Victoria. The population in Muleba is predominantly Wahaya (Haya-speaking), who depend on bananas as their staple food and coffee as a cash crop. The district covers an area of approximately 3500 km^2^ at an altitude ranging from 1100 m to 1600 m above sea level, with a population of 637,659 people (2022 population census) [29]. Misungwi is one of the eight districts of the Mwanza region, located on the southern border of Lake Victoria, north-western Tanzania. The population in Misungwi is predominantly Wasukuma (Sukuma-speaking), who mainly depend on maize, rice, and cassava as staple food and cotton as a cash crop. Misungwi has a population of 467,867 people, with 48% under 15 years of age. The study areas are described in detail elsewhere [26–28]. Both districts experience year-round malaria transmission, which peak in June/July and December/January. Rainfall occurs from September to December (short rainy season) and from March to May (long rainy season). Previous LLIN universal coverage campaigns in the study sites were conducted in 2011 in Muleba and in 2015 in Misungwi, during which Olyset Nets were distributed. Other LLIN brands present in these districts were provided through antenatal clinics and the School Net Programme (SNP). At baseline (before the study LLINs were distributed), malaria prevalence in the Muleba study area was 65% and 28% of the population reported using any LLIN the night before the survey. In Misungwi, malaria prevalence was 44% and 61% of the population reported using an LLIN [26, 27] (Table 2). Over the course of the trials, study LLIN use and malaria prevalence fluctuated in both settings (Table 2). Table 2. Usage of nets and malaria prevalence over the study periodDistrict/yearBaselineYear 1-post interventionYear 2-post interventionYear 3-post interventionMalaria infectionAll LLIN useMalaria infectionStudy LLIN useMalaria infectionStudy LLIN useMalaria infectionStudy LLIN useMuleba65.0%27.5%39.8%77.3%44.3%56.0%64.7%39.0%Misungwi44.2%61%21.9%61%42.140.9%38.5%22.3%
Data collection
The selection of respondents for quantitative and qualitative interviews and FGDs included a mix of random and purposive sampling.
Knowledge, attitudes and practices (KAP)
In Muleba, both baseline and post-intervention KAP surveys were conducted in 16 clusters (4 clusters per study arm) purposively selected based on LLIN usage [high (> 40%) or low (≤ 40%)] and malaria prevalence [high (> 30%) or low (≤ 30%)] (Additional file 1).
At baseline 40 households with children under 15 were selected per cluster. Data were collected on household demographics, LLIN ownership and usage, malaria knowledge, sources of malaria information, personal agency, perceived norms, perceptions of failed LLINs, and treatment-seeking behaviour. Socio-economic variables were not collected at baseline but were captured during the post-intervention survey. For the post-intervention survey, conducted three months after distribution, 48 households were randomly selected per cluster, including households without children under 15. This survey captured broader experiences with Behaviour Change Communication (BCC)/Information Education Communication (IEC) messages and preventive campaigns. Additional questions addressed exposure to social behaviour change communication (SBCC) materials and household involvement in LLIN and IRS campaigns. Pendragon Forms (Pendragon Corporation Software, Libertyville, USA) on Personal Digital Assistants (PDAs) was used to collect data (Table 3). Table 3. Definition of termsTermDefinitionAdherence to LLINs useThe extent to which individuals or households follow the recommended practices for using LLINs. It specifically involves: consistent use (using the LLIN even during non-peak malaria seasons), proper installation, care and repair and avoiding misuseConsistent LLIN useRegular and sustained use of LLINs by individuals or households for protection against malaria mosquitoes. Specifically, it means that people sleep under the net every night. High adherence ensures consistent use, but consistent use alone does not guarantee adherence if the net is not properly maintained or used effectivelyAcceptabilityThe degree to which a LLINs is considered suitable, desirable, and appropriate by the target population, and whether individuals and communities are willing to use and sustain the proper use of nets
In Misungwi, in each of the 84 clusters, at each survey timepoint (3, 12, 18, 24, 30, and 36 post-intervention), 45 households were randomly selected from a census list, except at 3 months where only 10 households were selected per cluster. KAP questions covered similar topics as in Muleba but were shorter and focused on acceptability of nets, perception on nets, favourable features of nets. In addition, in a subset of LLINs presence of bed bug on net as well as numbers were recorded. Surveys were conducted using Android Tablets with Open Data Kit (ODK) software.
In both settings, respondents were primarily household heads, their spouses, or other adults over 18 years of age. Data collection was conducted by field workers who had completed secondary education and received one week of training covering study design, field procedures, and questionnaires.
In-depth interviews (IDIs) and focus group discussions (FGD)
In each site, participants for IDI and FGD were purposively sampled based on study arm, LLIN usage (high/low), malaria prevalence (high/low), age and sex from baseline survey. In Muleba, participants were selected from 16 clusters (the same clusters involved in-KAP surveys) and in Misungwi from 20 clusters (5 clusters per arm) (Additional file 1).
In both sites, IDIs were conducted with selected district, ward, and village leaders, health facility administrators, Environmental Health Officers (EHOs), community health workers (CHWs) and heads or spouses of households. These interviews explored perceptions of malaria control and prevention interventions, their expected and unexpected effects, and contextual factors affecting the uptake of these interventions. Key informants were contacted directly and invited to choose a convenient time for their interview. The interviews were conducted in locations that ensured privacy and confidentiality for the participants.
FGDs were conducted separately within each demographic group. These groups included married men (26 + years), married women (26 + years), young men (16–25 years), and young women (16–25 years). In Misungwi, an additional group of primary school children (9–15 years) was included. The discussions focused on topics such as knowledge, attitudes, and practices related to malaria prevention and treatment, drivers and barriers to LLIN use, misconceptions about malaria and LLINs, and the acceptability and preferences for LLINs (Table 3).
General procedures for FGDs and IDIs
The FGDs and IDIs were conducted by two teams of researchers in Muleba in November 2014 and three teams in Misungwi in November 2021. All team members were university graduates fluent in local languages. Each team included one experienced researcher and one or two note-takers. Interviews were led by the experienced researchers, while the note-takers, who received two weeks of intensive training, documented and summarized the interviews. This training covered the study design, ethical treatment of participants, use of semi-structured guides, operation of tape recorders, and note-taking techniques. A semi-structured guide was used to initiate the discussions, covering topics such as malaria knowledge, the purpose of using LLINs, rumours or misconceptions about LLINs, factors influencing their use, non-use, and repurposing, as well as participants’ perceptions of LLIN characteristics and other preventive practices. Participants were encouraged to speak freely around the topics and to express their thoughts and feelings. The lead researcher (EL) observations and pictures and geo-locations were also included to authenticate the findings from the IDI and FGDs.
In Misungwi, due to the use of four distinct LLIN brands, participants were shown each brand during discussions to help them accurately identify the one they received and provide informed feedback. The qualitative feedback on the dual-AI LLINs is particularly relevant in the Misungwi study, as data was collected post-intervention. All FGDs and IDIs in both sites were conducted in Kiswahili, Kihaya, and/or Kisukuma.
Data management and analysis
In Muleba, quantitative data were transferred from PDAs to a Microsoft Access database. In Misungwi, data were uploaded from tablets to a server and downloaded as comma-delimited files. All data were then imported into STATA version 15 (Stata Corporation, College Station, Texas, USA). Data from all survey points were combined for analysis at each study site. Quantitative data analysis involved using descriptive statistics means, and proportions.
Interviews and discussions were primarily conducted in the mornings, lasting between 30 and 60 min. Each afternoon, a detailed summary of the main points by theme and study arm was created using the notes taken. In cases of discrepancies, digital recordings were reviewed. In Muleba, recordings of FGDs and IDIs were transcribed verbatim from Kihaya/Kiswahili and then translated into English. In Misungwi, recordings were directly transcribed and translated into English by an experienced translator. A sample of IDIs and FGDs was double-checked by the lead researcher (EL) before analysis.
Data were imported into NVivo version 14.0. For coding, text searching, and data merging. Triangulation of qualitative and quantitative data was also used to validate and interpret emerging patterns. A thematic analysis was applied using a deductive approach, guided by the study’s conceptual framework. Themes and sub-themes were examined considering the frequency, intensity, and diversity of views expressed. This flexible approach allowed for the identification, analysis, and reporting of patterns within the data. Matrices were constructed for each main theme, incorporating relevant data from IDIs and FGDs. These matrices facilitated cross-comparisons across interviews and groups to assess the strength of acceptability. All data were analysed using this method. Relevant quotes were selected to support and illustrate the findings.
To maintain anonymity, FGD participants were assigned random numbers, and IDI participants were coded. Quotes were reported using participant numbers or IDI codes, along with the district and cluster category, whether from areas of low or high malaria prevalence or low or high LLIN use.
Ethics
Muleba trial
The trial was approved by the ethics review committees of the Kilimanjaro Christian Medical University College, the London School of Hygiene & Tropical Medicine, and the Tanzanian Medical Research Coordinating Committee (NIMR/HQ/R.8a/VolIX/1803). A trial steering committee reviewed progress. Written informed consent was provided by adult participants.
Misungwi trial
Ethical approval for the RCT was secured from the institutional review boards of the Tanzanian National Institute for Medical Research (NIMR/HQ/R.8a/Vol.IX/2743), Kilimanjaro Christian Medical University College (2267), London School of Hygiene & Tropical Medicine (14,952; 14,952-1), and the University of Ottawa (H-05–19-4411). Written informed consent was obtained from adult participants. For children, written assent forms were completed by both the children and their parents or guardians prior to the discussions.
Results
A total of 1,397 households were visited during the KAP surveys in Muleba, with 88% (560/640) households interviewed (consented) pre-intervention and 78% (593/768) households consented post-intervention. In Misungwi, the KAP questions were embedded in prevalence surveys and included responses from 13,322 households across six post-intervention surveys. Qualitative data were collected through 44 IDIs (14 conducted in Muleba and 30 in Misungwi), and 36 FGDs, with 17 in Muleba and 19 in Misungwi, as detailed in Table 4. Table 4FGDs, IDIs, and KAP done in Muleba, and MisungwiStudy siteMulebaMisungwiIn-depth interviews (IDIs) groupsNumber of IDIs conductedNumber of people interviewed in IDIsNumber of IDIs conductedNumber of people interviewed in IDIsDistrict health workers2211Environmental health officers (EHO)N/AN/A44In-charges of dispensariesN/AN/A55Villages and ward leaders8855Community health workers (CHW)4466Household heads and spousesN/AN/A99Focus group discussions (FGDs) groupsNumber of FGDs conductedNumber of people in discussionNumber of FGDs conductedNumber of people in discussionMarried men (26 + years)541334Married women (26 + years)545446Young men (16–25 years)430440Young women (16–25 years)327224Primary school boys (9–15 years)N/AN/A224Primary school girls (9–15 years)N/AN/A448
Knowledge, and awareness about malaria
In both districts, the majority of respondents correctly identified mosquito bites as the cause of malaria (92.5% in Muleba, 86.6% in Misungwi) (Additional file 2). However, a small percentage of respondents still hold misconceptions such as attributing malaria to superstitions (11.4%) in Misungwi. This misconception was significantly higher in households where the head of the household (p = 0.0001) or the wife (p = 0.0051) had not attained formal education. No significant differences in misconception were observed by socio-economic status (p = 0.1115).
In Muleba, sun exposure was thought to be associated with malaria, with 7.1% of respondents holding this belief at baseline, increasing to 16.9% post-intervention. This perception remained consistent across sex (p = 0.5097), age group (p = 0.4768), socio-economic status (p = 0.5207), and education level (p = 0.5464). Most respondents were aware that using LLINs helps prevent malaria, with (91% in Muleba) recognizing their importance (Additional file 2). However, the practical application of this knowledge varied, particularly during hot seasons (Box 1).
Box 1: Malaria knowledge, and awareness (quotes) KII 1: Muleba, district levelRespondent (R): Many people do not use LLINs during hot seasons, and it is that time when mosquitoes and malaria are peaking…Sensitization messages need to be intensified for a change of behaviour to use LLINs all the timeFGD 1: Muleba, high malaria clusterP5: Malaria is caused by mosquitoes. Not all mosquitoes cause malaria, the most known to cause malaria are the female anopheles…Mosquito bites all the time, but the ones that transmit malaria bite late at nightIDI 1: Misungwi, high malaria prevalence clusterR: I own a restaurant (many people gather here), I overhear them saying that my child is suffering from malaria, so malaria is high in our community, and the children suffer mostR: We usually use nets during the heavy rain season, but we were advised to use them year-round since mosquitoes are still present. Some people, when summer begins, take down their mosquito nets and store them awayR: I have learned that using mosquito nets helps you a lot not to catch malaria, and if you don’t use it you will suffer from malaria since there are a lot of mosquitoes in here….it also can protect you from snakes, and other dangerous insects like spidersFGD 2: Misungwi, high malaria and high net use clusterP6: The first protection we take is using the best quality mosquito net not like the mosquito nets that we received before which had big holes. Also, the family must drink clean waterFacilitator: How is malaria transmitted from one person to the other?P7: Malaria spread through the air from one person to the other. Yes, when one sneezes while he/she has malaria fever, when that air reaches you it means you will also catch malaria, yes it spreads through the airFGD 3: Misungwi, high net use clusterP2: There is one family in our neighborhood whose child had malaria, and they delayed taking him to the hospital after three days of taking antibiotics he did not recover so they took him to Mitindo Hospital [district hospital] where tests revealed he had chronic malaria. Unfortunately, despite the hospital’s efforts, the child passed away shortly after. So, we can say it is a big problem that’s the reason we are losing many children because of malariaP7: It’s not possible to recognize that I have malaria, but I might have symptoms like fever, headache, joint pains, chills, and tiredness. Another symptom that I never understand is stomach ache because once I go for the test it is confirmed that I have malariaFGD 4: Misungwi, low malaria and low net use clusterP5: What I know is if the mosquito bites a breastfeeding woman if that woman gets malaria, she will be able to infect the child
P = participant in FGD; R = Respondent in IDI
In the qualitative studies (Box 1) despite high awareness about malaria, some respondents, especially in Misungwi, believed that malaria could be spread through the air or from a breastfeeding mother to her child. There was skepticism about whether malaria could be a direct cause of death, with some attributing deaths related to malaria to other causes, including witchcraft.“…At funerals, if the cause of death is stated as malaria, there is often a collective murmur of disbelief, with people questioning, "Has only malaria killed him/her?" They struggle to accept that malaria alone could be the cause of death”. (P9: FGD Misungwi, low malaria, and low net use cluster)
Determinants of LLIN use
During the baseline survey in Muleba, net usage among respondents significantly varied by sex, with more women reporting using nets than men (p = 0.0016), but not by age group (p = 0.2955) nor education status (p = 0.6027). The main reasons given for not using nets at baseline were not having enough nets (56.5%) or available nets being worn out/too torn (29.4%) (Additional file 2). Three months after the net distribution, 94% of people reported using nets (Additional file 2), and this usage did not differ by socio-economic status (p = 0.1966), or sex (p = 0.9990) or education level (p = 0.8045). In the qualitative study, the main determinant of consistent LLIN use included having sufficient LLINs within the household, the perception that LLINs decrease malaria risk, avoiding mosquito bites, and protection from other pests like spiders, snakes, and rodents.*“….Many households lack enough nets, and the ones they have are badly torn. You know, in the last campaign, only two bed nets were provided per household, regardless of the number of sleeping places or people”. (IDI 2, Muleba, low malaria & low net use cluster).“They are using nets to prevent mosquitoes; it has become their habit nowadays. Also, the level of disease has decreased because mosquito nets protect them. Even in my family, there was frequent fever but once we started using mosquito nets fever has decreased” (IDI 3: Misungwi, high malaria cluster)“One day, my wife and I visited a relative in a distant village. At night, they set up a net where we were allocated to sleep. To our surprise, when we woke up in the morning, we saw a tiny snake on the roof of the net. Since then, I always use a net when I sleep, whether there are mosquitoes or not, you never know what might show up.” (P5: FGD 10**: Misungwi, high malaria & high net use cluster)“There are so many mosquitoes in our environment, you cannot sleep without using a mosquito net, and these mosquitoes are very tiny, but their bites are intense, often leading to skin rashes” (P6**: FGD 2: *Misungwi, high malaria & high net use cluster)
Moreover, the primary reason for using LLINs was to avoid mosquito bites and malaria, but a key motivator was also the financial burden of recurrent malaria cases. LLINs are seen as a way to reduce these costs and protect family finances.*“…I’m their sister, and I encourage them to use mosquito nets because whenever they fall sick, they come to me right away asking for money for medication.” (P9: FGD 5**: Misungwi, *low malaria & high net use cluster)
Barriers to consistent use of LLINs, acceptability, favourable, and unfavourable characteristics of LLINs
Adverse effects
Itching and facial burning sensations were cited as significant factors contributing to the inconsistent utilization of LLINs, particularly during the initial period of use across all LLIN types. Three months post intervention, during KAP survey, majority of users reported side effect resulting from use of nets and were more pronounced in cluster that received Interceptor (55%) and Royal Guard (48%) and less in Interceptor G2 (11%) and Olyset Plus (11%). However, there was no statistically significant difference in net usage across study arms irrespective of the side effects mentioned (p = 0.169). Contrary to qualitative findings through IDIs and FGDs that was conducted 33 months post-intervention, side effects were overwhelming attached to hindering net usage especially from Interceptor and Royal Guard arms in Misungwi.*“One day I had a guest and I hung a mosquito net [Royal Guard]; he woke up in the middle of the night scratching his face, it felt like it was on fire. The net was itchy, he developed a skin rash, and the irritation lasted for a day before it faded.” (IDI 7, Misungwi, high malaria & high net use cluster).Interviewer: What about you?Participant: “…even myself, I used it when it was still new, it caused itching for three days.” (IDI 7, Misungwi, high malaria & high net use cluster).“…it has too much insecticide that burns the faces and the whole body. The burning sensational can last between half an hour to three hours” (P6: FGD 11: *Misungwi, high malaria & high net use cluster)
Bed bugs infestation
Bed bug infestations in mosquito nets emerged as a common barrier reported in both in-depth interviews and focus group discussions. Respondents commonly reported that bed bugs tend to congregate at the hanging points of the LLINs and descend during the night to feed on sleepers. Consequently, to mitigate the risk of bed bug bites, many participants opted to avoid hanging the nets altogether. The discomfort and intense itching associated with bed bug bites compelled some users to either discard their infested LLINs or subject them to washing with hot water, a practice that likely contributed to net shrinkage [30] and insecticide depletion [31]. While bed bugs are not disease vectors, their bites cause significant discomfort and distress.*“What my colleague mentioned is true, many individuals in our community are reluctant to use mosquito nets due to the fear of bedbug infestations. For them, the discomfort of bedbug bites outweighs the risk of contracting malaria. Consequently, we are requesting that the project consider providing nets that offer protection against both mosquitoes and bedbugs. If such nets were available, no one would hesitate to use them, as it would address both concerns simultaneously, effectively eliminating the incentive to remove the nets”. (P3: FGD 3**: Misungwi, low malaria & high net use cluster)“…In our community, when people first began using mosquito nets, they encountered significant infestations of bedbugs. As a result, many individuals discontinued the use of the nets”. (IDI 5**: *Misungwi, high malaria & high net use cluster)
However, across both the IDIs and FGDs, participants consistently avoided directly admitting to having bed bugs in their own homes, as the presence of bed bugs is culturally stigmatized and often associated with poor hygiene. Acknowledging such an infestation is seen as shameful, leading individuals to speak about the issue in a detached, third-person manner, rather than personalizing their accounts. This tendency to dissociate from the problem underscores the social stigma attached to bed bugs. Despite this reluctance to admit personal experiences, the KAP study revealed that nearly one fifth of the nets had bed bugs, with an average of 14 bed bugs per net (Table 7).*“The belief that mosquito nets are responsible for the emergence of bedbugs has become widespread within the community, leading to numerous complaints. For instance, there was a woman who hung her mosquito nets elsewhere without using them, and when we inquired why, she responded that the nets had caused bedbugs. We took the opportunity to educate her about the environmental factors that contribute to bedbug infestations and provided her with guidance on effective measures to eliminate them. It is important to approach this issue sensitively; directly attributing bedbugs to poor hygiene can be upsetting for community members. Instead, the focus should be on educating them about practical steps to prevent bedbugs from thriving in their homes”. (KII 2**: *Misungwi, district level)
LLIN supply and perceived physical integrity
In Muleba, the pre-intervention quantitative survey revealed that barriers to consistent LLIN use included insufficient supply (56.5%) and LLINs being too torn (29.4%) (Table 5). Table 5. Attitudes towards LLIN characteristics and practices in Muleba and MisungwiIndicatorsMuleba Pre-intervention: (Dec 2014)Misungwi Post-intervention: (2020–2022)Mosquito net colour preference% (n)% (n)Dark colours(blue/green/black/red)61.0 (339)92.8 (2539)Any colour34.2 (190)2.7 (74)Light colours (white/yellow)4.9 (27)4.5 (123)Net shape preference% (n)% (n)Rectangular/square61.4 (344)90.7 (2482)Any shape22.3 (125)2.6 (70)Conical (round)16.3 (91)6.7 (184)How do you decide that the net has failed?% (n)% (n)The bed net has too many holes71.5 (397)88.2 (4165)There are many mosquitoes inside the net7.6 (42)7.7 (361)The bed net is dirty6.7 (37)4.2 (196)The net is too olds14.2 (79)0 (0)What do you do when a net has failed?% (n)% (n)Discard the net49.1 (273)37.7 (1778)Repair and reuse the net31.5 (175)27.4 (1293)Use for alternative purposes19.4 (108)34.9 (1651)What alternative purposes do you use the net for?% (n)% (n)Ropes0 (0)54.5 (1034)Used as bedsheet/mattress47.7 (51)28.6 (543)Cover holes in the wall(s)/curtains/stuff eaves37.4 (40)7.4 (140)Enclosing poultry11.2 (12)6.3 (120)Collecting winged termites14.9 (16)0 (0)How often do you sleep under the net?% (n)% (n)Always ‘right now’47.8 (266)94.0 (548)Never ‘right now’27.1 (151)3.6 (21)Sometimes25.1 (140)2.4 (14)Why do you sometimes or never sleep under the net?% (n)% (n)Not enough nets56.5 (144)20.0 (5)Net worn out/too torn29.4 (75)8.0 (2)Other reasons14.1 (36)72% (18)
Across all IDIs and FGDs, respondents consistently cited excessive damage to the study LLINs as a primary constraint to LLIN use. In Misungwi, where both polyethylene and polyester LLINs were distributed, polyethylene LLINs (specifically Olyset Plus) were most frequently mentioned as being prone to damage.“I noticed that this net [Olyset Plus] tears easily, which is why it’s no longer available in many households. Even a slight squeeze on the bed can cause it to rip. (P1: FGD Misungwi, low net usage cluster)
Perceptions (infertility, impotence and poor sexual drive)
Cultural beliefs also played a role, with some respondents citing that LLINs could cause impotence or infertility.*“You know, some people spread misinformation, claiming in front of others that mosquito nets negatively affect male sexual performance… (laughter)”. (IDI 3**: Misungwi, high malaria village).“…They believe that using mosquito nets can diminish sexual drive in men, and they also claim that women who sleep under them may struggle to conceive”. (IDI 4**: *Misungwi, low malaria & low net usage cluster)
However, other participants in the same focus group discussions dismissed this belief, arguing that a lack of male sexual drive is a personal issue and unrelated to the use of LLINs, seeing it instead as an individual problem.“…(amidst loud group laughter)… There is no such thing; that is a personal problem. If the drive isn’t there, it simply isn’t there. If you’re unwell, that’s your individual issue. The nation will not succumb to malaria because of such a misguided belief” (P4: FGD 6**: Muleba, high malaria & low net usage cluster).“…that is a personal issue. I’ve been using mosquito nets for years, yet my performance [referring to sexual drive] remains strong, and my wife continues to bear children. In fact, we just welcomed a baby girl two months ago (followed by loud and hearty group laughter)” (P2: FGD 3, Misungwi, low malaria & high net use cluster).
Seasonality of net use
Some respondents indicated a belief that the mosquito population had declined, reducing the perceived necessity of using LLINs. This belief is consistent with the common perception that mosquitoes are absent during the dry season.“…For instance, I once visited my uncle and noticed that they weren’t using nets. I asked them, ‘Why aren’t you using nets?’ They responded that there are no mosquitoes anymore. I explained that this isn’t true because mosquitoes come and bite you at midnight while you’re asleep, making it difficult to notice. I then asked whether they had recently been sick with malaria, and he replied, ‘We’re puzzled about why we’re getting malaria when there are no mosquitoes.’ I told them that mosquitoes are indeed present, and therefore, they need to use nets.” (P9: FGD 5: low malaria & high net usage cluster)
Another barrier to LLIN use mentioned in Misungwi was discussed by married women- that husbands returning late from drinking impeded use of the nets.
Acceptability, favourable, and unfavourable characteristics of LLINs
Net acceptability, measured by the proportion of users reporting their LLINs as no longer protective, varied significantly across products at all assessed timepoints (p < 0.0001 for 24, 30, and 36 months). Olyset Plus consistently had the highest dissatisfaction levels (17.8%, 12.4% and 15.2%) followed by Royal Guard (11.7%, 7.5%, and 13.4%), while Interceptor G2 and Interceptor maintained the lowest reports (5.7–9.3%) (Additional file 3).
As shown in Table 5, blue LLINs were the most preferred colour by respondents in both districts. In Muleba the colour preference was 61% for dark colours (blue, green, black and red), 4.9% for light colours (white and yellow) and 34.2% feeling colour indifferent (Table 5). In Muleba, colour preference did not significantly differ by sex (p = 0.9982), or age group (p = 0.6921), but by education status (p = 0.0229). Those with primary or higher education had slightly more preference for light coloured nets (22% vs 16%). In Misungwi 93% of the respondents preferred dark coloured nets. This colour preference did not differ by socio-economic status (p = 0.1360).“I prefer the blue mosquito net because it holds up well against dust. With our red soil and uncemented floors, it’s a relief to have a net that stays clean and doesn’t show dirt easily.”. (P8: FGD 2, Misungwi, high malaria & high net use cluster).
Rectangular LLINs were preferred by 61.4% of respondents in Muleba and 90.7% in Misungwi (Table 5). In Misungwi, where both polyester and polyethylene nets were distributed, the KAP survey participants indicated a strong preference for polyester nets 86% (2338/2736) over polyethylene alternatives 11% (86/2736).
Comparing study nets with the nets they had previously
In both sites, participants were asked to compare the study nets with the nets they had previously. In the quantitative surveys, Muleba (Table 6) and Misungwi (Table 7), no much differences were observed across study net type. However, the qualitative finding in Misungwi revealed that there were differences when people were asked to rate study nets against the nets they owned/used in the past. Interceptor G2 consistently received positive feedback for its physical features and effectiveness in reducing malaria among children.“This mosquito net [Interceptor G2] does not get damaged easily, it last up to four years before showing wear. It’s soft, easy to wash, and effectively prevents mosquito penetration.” (P3: FGD 7, high malaria & high net use cluster).Table 6. Comparing perceptions over Olyset Plus, Olyset nets and IRS in the Muleba district (data from KAP survey collected 3 months after post-intervention)MulebaHow do you compare project LLINs to your previous LLINs?Olyset net: % (n)Olyset plus: % (n)This LLIN is better62.2 (166)72.7 (216)The LLIN is the same as previous nets26.6 (71)17.5 (52)This LLIN is worse3.8 (10)2.7 (8)Don’t know7.5 (20)7.1 (21)Why is this project LLINs better than your previous LLINs?Olyset netOlyset plusThis round the nets have strong insecticide58.1 (97)61.8 (134)This round the nets are larger18.6 (31)16.1 (35)This round premade holes in the net are smaller13.2 (22)14.8 (32)This round the nets are durable9.6 (16)5.5 (12)Other01.8 (3)How long does the insecticide last on LLINs or IRS walls?IRSLLINsOne year or less22.9 (136)19.7 (117)Two years1.7 (10)2.5 (15)Three years1.7 (10)2.2 (13)Four years0.3 (2)0.5 (3)Five years or more5.9 (35)14.3 (85)Don’t know67.5 (400)60.7 (360)Table 7. Comparing study nets in Misungwi district (data from KAP survey)VariablesRoyal guard: % (n)Olyset plus: % (n)Interceptor: % (n)Interceptor G2: % (n)How do you compare project nets to your previously used nets?This net is better59.4 (590)48.4 (366)69.3 (802)66.1 (869)They are similar28.4 (282)38.4 (291)23.6 (273)28.7 (377)This net is worse6.8 (68)7.5 (57)2.2 (25)1.5 (20)Don’t know5.4 (54)5.7 (43)4.9 (57)3.7 (49)Why is this net better?Mosquitoes cannot penetrate80.5 (494)74.8 (294)71.7 (616)69.2 (659)The net is soft7.3 (45)9.2 (36)12.0 (103)10.2 (97)Does not acquire holes easily5.2 (32)4.8 (19)4.9 (42)8.2 (78)It is new1.1 (7)0.8 (3)0 (0)0 (0)Does not itch0.2 (1)0.3 (1)0.6 (5)0.2 (2)Children don’t get malaria1.0 (6)1.8 (7)0.1 (1)0.4 (4)Don’t know/other4.7 (29)8.4 (33)9.5 (82)11.8 (112)Proportion of nets observed with bed bugs: % (n/N)19.4 (87/448)19.0 (58/305)28.7 (218/761)22.2 (157/707)Mean number of bed bugs per LLIN observed by field worker [95% CI]^a^14.2 [12.1–16.3]14.3 [11.7–16.9]14.8 [13.4–16.1]15.4 [13.7–16.9]^a^We capped bed bug counts at 30
Olyset Plus was distributed across both districts, with user perceptions differing by location. Olyset Plus was slightly preferred to Olyset net in Muleba (62.2% vs 72.2%), p = 0.1395, due to its favourable qualities (strong insecticidal properties) (Table 6). In Misungwi, in the qualitative study, participants expressed concerns about its physical integrity, noting that Olyset Plus did not physically last as long as expected.“This net [Olyset plus], is good, but it tears easily.” (P7: FGD Misungwi, low net use cluster)
In Misungwi, both Royal Guard and Interceptor nets were noted to cause adverse effects like skin irritation and facial burning. These negative experiences led to a decrease in LLIN use among some respondents especially in the immediate days after distribution.“Due to the negative impact of the net [in Royal Guard arm], such as causing rashes when first used, people stopped using them entirely” (P11: FGD 7, high malaria & high net use cluster).
Repurposing of LLINs
In both Muleba and Misungwi, participants reported repurposing LLINs for various tasks, including making ropes, protecting crops, and screening windows (Fig. 2). For example, 54.5% of respondents in Misungwi used LLINs as ropes, and 28.6% used them as bed sheets or mattresses (Table 5).Mosquito nets are used to protect seedlings (P3), poultry coops (P4) and making ropes because they do not cut easily (P7) (FGD 2*: **Misungwi, high malaria, and high net use cluster)*Fig. 2. Repurposing of LLINs: Beneficial repurposing (window screening) (A–B), torn into strips for making fishing traps and ropes (C–D), protecting seedling and young plants (E–F), for making poultry coops (G–H), drying cassava (I–J)
It was also observed that local government leaders at the ward and village levels have implemented strict measures to control malaria. These measures include preventing the misuse of nets and ensuring that households maintain cleanliness around their surroundings to eliminate potential mosquito breeding sites.“I was fined for tying six bags of scarlet eggplant ‘nyanya chungu’ with net strings at Buhongwa market [a famous farmers market]” (P7: FGD 7, high malaria & high net use cluster).Interviewer: Who fined you, and how much did you pay?“An environmental health officer came by and questioned who permitted me to use a net for tying my bags. I ended up having to pay two thousand Tanzanian shillings per bag as a fine, so I’ve decided never to use those nets again, except for sleeping under them” (P7: FGD 7, Misungwi, high malaria & high net use cluster)“Last month, we prosecuted some individuals who refused to participate in community cleaning activities and failed to cover ponds around their homes, these actions are crucial for preventing mosquito breeding and controlling malaria” (KII 5, Muleba, ward level).
Lead researcher (Eliud Lukole’s 6.14 kms observational walk)
In November 2021, same time when the qualitative study was conducted in the Misungwi district, the lead researcher (EL) took the opportunity to explore various alternative uses of nets in 43 households in one of the hamlets. As the researcher walked through the area (Additional file 5), he used a handheld GPS to record geolocations and a phone to take photographs of repurposed LLINs, especially those where whole or large sections were utilized. The researcher engaged with residents, asking about the reasons behind each specific use. The majority of these LLINs were employed to cover crops or as barriers around areas where crops were planted or as chicken coops (Fig. 3). At household number 28, the researcher had an extended conversation with a potato farmer who was tending to his tomato nursery (Fig. 4). The collected images were then superimposed onto a map, corresponding to their geolocations, to illustrate the proximity of these households (Additional file 5).Fig. 3. Images of re-purposed nets from Eliud Lukole’s 6.14 km walkFig. 4Tomato nursery at house number 28
Increasing LLIN use: participant recommendations
Participants provided key recommendations for maintaining LLIN use. Regular awareness programmes should be tailored to local languages to reach both literate and illiterate populations, addressing misconceptions and educating on malaria, LLIN benefits, and proper use. Training and incentives for community health workers (CHW) to conduct door-to-door education were also recommended to boost programme coverage, while village meetings were discouraged due to low attendance.“They [CHWs] are volunteers, but their work is challenging, and they need some motivation. Please support them during malaria activities, as they often work in harsh environments. For instance, during a COVID-19 pandemic, the DMO [District medical officer] offered ten thousand shillings to CHWs for vaccinating ten people”. (KII 2, Misungwi, ward level)
Distinct differences between Misungwi and Muleba that might influence potential repurposing of LLINs
Both districts had similar exposure to SBCC messages and comparable knowledge of malaria prevention (Additional file 2). However, Misungwi households had more LLINs at baseline (62.3% access of 1 LLIN per sleeping space used last night, and 61% usage) than Muleba (16.9% access and 27.1% usage) (Additional file 7), and cultural, lifestyle, and SES differences between the districts may have influenced LLIN use and repurposing (Additional file 6).
Discussion
This study evaluated community perceptions of malaria prevention, and the acceptability and preference of dual-AI LLINs compared to standard LLINs (Olyset net and Interceptor) in Muleba and Misungwi districts, Tanzania, where these novel nets were introduced. Acceptability, defined as the extent to which nets are perceived as suitable and effective by users, was high for dual-AI LLINs but varied across net types. Interceptor G2 was the most preferred net in Misungwi due to its perceived physical integrity, soft texture, and superior effectiveness in reducing malaria, particularly among children. By contrast, Olyset Plus, though perceived as effective, was less favoured in Misungwi due to frequent tearing. In Muleba, where only polyethylene nets have been distributed, Olyset Plus was well received for its perceived strong insecticidal properties compared to the standard Olyset net. Side effects were associated with certain brands of nets, with participants reporting skin irritation, burning, and itching linked to Royal Guard and Interceptor. Net preferences were primarily driven by durability, comfort, and efficacy, underscoring the need for user centred designs to optimize acceptability and consistent usage.
Participants frequently reported side effects associated with Royal Guard (48%) and Interceptor (55%), likely due to higher concentrations of alpha-cypermethrin, as reported in other studies [32–34], which is known to cause more side effects than permethrin [33, 35, 36]. A Benin RCTs [37] also reported similar transient adverse events, such as itching and mild skin irritation, associated with alpha-cypermethrin with 63.8% of Interceptor users and 52.5% of Royal Guard users, reporting side effects [27, 37]. These numbers were higher than those reported in Liberia [38], where only 17.5% reported issues with Interceptor LLINs. The quantitative findings in this study showed that while side effects were commonly cited, they did not deter LLIN usage in most households. This may be because side effects are short-lived and typically resolve within a few days of use, as well as the protective benefits of the nets against malaria, which participants emphasized, outweighing any discomfort. However, in a small subset of users, these effects did lead to reduced adherence or even non-use. Given these findings, adverse events associated with LLIN use during distribution campaigns should be monitored. Clear communication about the transient nature of most side effects and strategies to mitigate discomfort (e.g., washing nets before use, as recommended to participants in this study) may further enhance user compliance and satisfaction.
The dissatisfaction reported in among users of Olyset Plus reporting their nets ineffective could be paralleled with the decline in their durability observed in bio efficacy [31], physical integrity [30, 31]. The decline in perceived protection may have contributed to reduced net use over time which was more pronounced in Olyset Plus cluster [30, 39], with only 16% of study nets still in use at 36 months and just 19% of households maintaining sufficient net coverage. This convergence of biological degradation, physical wear, and declining user confidence highlights the critical role of both technical durability and behavioural adherence in sustaining LLIN effectiveness. Products that combine chemical longevity with user acceptability driven by perceived comfort, net shape, colour, and continued protection are more likely to retain high usage over time and achieve durable epidemiological impact.
In this study, LLINs were primarily used when mosquito-biting nuisance was high or malaria was perceived as a significant threat. In villages with high biting nuisance, participants continued to use LLINs even if they do not like certain features such as the fabrics, whereas in low biting nuisance areas these characteristics resulted in inconsistent or non-use. Those findings align with evidence from Solomon Islands where participants in areas with high and perennial mosquito nuisance reported consistent LLIN use despite unfavourable net attributes, whereas those in low or seasonal transmission settings more often cited discomforts as justification for intermittent or non-use [9]. Previous studies have similarly linked high mosquito densities and perceived malaria risk with LLIN compliance [40, 41]. Educational programmes should emphasize that the risk of malaria persists even when mosquito numbers are low and should be consistently use for better impact [42].
Repurposing of LLINs was notably more prevalent in Misungwi compared to Muleba, and this pattern appears closely tied to the baseline net coverage and subsequent net distribution dynamics. At baseline, households in Misungwi had significantly higher LLIN access (65.8% population access) and usage (61%)[27] than those in Muleba (37% access and 27.5% usage) [26]. More so, Misungwi received PBO LLINs earlier through the School Net Programme (SNP), prior to the main study mass campaign, which may have contributed to net saturation and the perception that new nets would continue to be distributed frequently. This oversupply appears to have created reduced perceived value of LLINs, fostering a disposable attitude and leading to increased misused nets being repurposed for non-malaria-related uses [43]. This is further supported by qualitative findings showing that households in Misungwi were more likely to treat nets as replaceable goods due to their abundance and expectation of continued supply. Moreover, this behavioural trend is reflected in net survivorship data: although 92% of households in Misungwi owned at least one study net after 12 months, ownership dropped to 62% by month 36, and actual study net usage declined from 72 to 23% over the same period [39]. In contrast, net survival and use in Muleba where baseline access and use were lower, was relatively better maintained. This suggests that excessive initial coverage, without reinforcing value through social behaviour change communication (SBCC), may paradoxically erode long-term net survival and use.
While knowledge about malaria prevention was high among participants, with over 90% demonstrating a clear understanding of key concepts, the practical application of this knowledge often varied. This highlights the gap between knowledge and behaviour, emphasizing the role of contextual and cultural factors in LLIN use. Evidence suggests that knowledge alone is rarely sufficient to drive or sustain behavioural change [44]; contextual factors such as environmental conditions, cultural norms, and competing priorities significantly influence compliance. For example, despite high levels of knowledge, some participants reported reduced LLIN use during the hot season, citing discomfort as a barrier.
Preferences for LLINs vary greatly across settings, with a strong preference for blue, rectangular LLINs observed in this study, aligning with similar findings from Kenya [23, 24]. The widespread preference for blue nets stems from prolonged distribution via national distribution programmes, which have fostered familiarity and acceptance. Moreover, in dwellings with mud walls and uncemented floors, blue nets are perceived to conceal dirt more effectively, thereby minimizing the frequency of washing. Rectangular nets are considered more practical by many households as they are easier to tuck under mattresses, offer broader surface coverage, and better accommodate multiple sleepers a common scenario in high-density sleeping arrangements. In contrast, regions such as Ethiopia [45, 46] and Senegal [47] exhibit a marked preference for conical LLINs, primarily attributed to their ease of installation and efficient space utilization. This preference underscores the influence of cultural practices, housing structures, and user experience on LLIN adoption, highlighting the need for context-specific design considerations in vector control interventions.
The study identified prevalent misconceptions about malaria transmission, including beliefs linking it to contaminated water, bad air, sun exposure, or superstition. Some participants also perceived LLINs as attracting bed bugs similar to findings in Kenya [23], a concern that warrants targeted education [48, 49]. While LLINs are not designed to target bed bugs, pyrethroid-treated nets have shown some suppressive effects [50]. However, multiple studies have reported varying degrees of pyrethroid resistance in bed bug populations [51–55]. The comparable infestation rates observed across study arms likely reflect the limited efficacy of current LLINs under prevailing bed bug pressure, a situation that warrants targeted entomological investigation to better characterize resistance patterns and inform control strategies.
This study has several limitations. First, its qualitative nature limits the representativeness of findings for the wider population. Nonetheless, the inclusion of quantitative data from two districts helps provide a broader perspective. Second, recall bias regarding previously used nets may have influenced participants’ comparisons. This effect was largely mitigated by the balanced design of the RCTs, which distributed such biases evenly across study arms. Third, the observed variation in the desirability of Olyset Plus between Muleba and Misungwi underscores the need for larger-scale studies. Finally, potential biases in self-reported data on LLIN ownership and usage frequency are acknowledged; however, nets were physically observed and inspected before being recorded.
Conclusion
This study reveals that the acceptability and consistent use of dual-AI LLINs are primarily driven by perceived efficacy, fabric quality, mosquito nuisance, and comfort. Issues like physical integrity, bed bugs, and adverse reactions hinder optimal use. Generating entomological data on non-target pests such as bed bugs could inform net selection and improve uptake. Educational programmes focused on adult men, the primary non-users, could improve net utilization. Since education level shapes colour preferences and malaria misconceptions, integrated campaigns are needed to dispel myths and promote consistent use. Incorporating user perception metrics into LLIN evaluation and procurement strategies will further align interventions with community needs.
Supplementary Information
Additional file 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1MMV. Knowledge sharing for severe malaria: Severe malaria observatory. 2023 [cited 2024 05/01/2024]. Available from: https://www.severemalaria.org/countries/tanzania.
- 2PMI. Tanzania (Mainland) malaria profile. https://mesamalaria.org/wp-content/uploads/2025/04/TANZANIA-MAINLAND-Malaria-Profile-PMI-FY-2024.pdf
- 3Alliance for Malaria Prevention. Net mapping project. The elliance for malaria prevention 2024. https://allianceformalariaprevention.com. Accessed 11 Mar 2024.
- 4Ministry of Finance and Planning, National Bureau of Statistics Tanzania and Presidents’ Office. Administrative units population distribution report. Zanzibar. 2022. https://www.nbs.go.tz/uploads/statistics/documents/sw-1705484561-Administrative_units_Population_Distribution_Report_Tanzania_Mainland_volume 1b.pdf. Access 05 May 2024.
- 5Acosta A, Koenker H, Brown A. Social and behavior change for insecticide-treated nets. Vector Works Project, John Hopkins Bloomberg School of Public Health. Baltimore, 2019. https://continuousdistribution.org/wp-content/uploads/2022/03/pmi-vectorworks-social-and-behavior-change-for-insecticide-treated-nets-2019-toolkit.pdf. Access 09 Jan 2025.
- 6MSF. Public health engineering in precarious situations. Paris, France; 2010. https://medicalguidelines.msf.org/sites/default/files/2022-06/Public_health_engineering_2010.pdf. Accessed 10 Jul 2024.