Change in maternal income status following stillbirth, neonatal death and severe neonatal morbidity
Jennifer A. Jairam, Hilary K. Brown, Christina Diong, Howard Berger, Jun Guan, Eyal Cohen, Joel G. Ray

TL;DR
This study found that adverse birth outcomes like stillbirth or neonatal death are linked to a higher chance of mothers remaining in or moving to lower-income neighborhoods for subsequent births.
Contribution
The study introduces a novel analysis of how specific adverse birth outcomes affect maternal residential income mobility over time.
Findings
Mothers with non-fatal severe neonatal morbidity were more likely to experience downward income mobility.
Stillbirth and neonatal death were associated with a higher likelihood of remaining in the lowest-income neighborhood.
Adverse birth outcomes were linked to reduced upward income mobility between consecutive births.
Abstract
We evaluated whether stillbirth, neonatal death or severe neonatal morbidity is associated with a mother’s change in residential neighbourhood income between two consecutive births. This population-based cohort included all mothers in Ontario, Canada with two consecutive births at 20–42 weeks’ gestation, 2003–2023. The study exposure at the first birth was: (i) livebirth unaffected by severe neonatal morbidity or neonatal death (referent); (ii) livebirth with severe neonatal morbidity but no neonatal death; (iii) livebirth with neonatal death; and (iv) stillbirth. The study outcome was a mother’s change in residential neighbourhood income quintile (Q) between two consecutive births: (i) downward income mobility, (ii) upward income mobility, or (iii) persistently residing in the lowest income Q1 at each birth. -- each relative to iv) no change in neighbourhood income Q between births…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
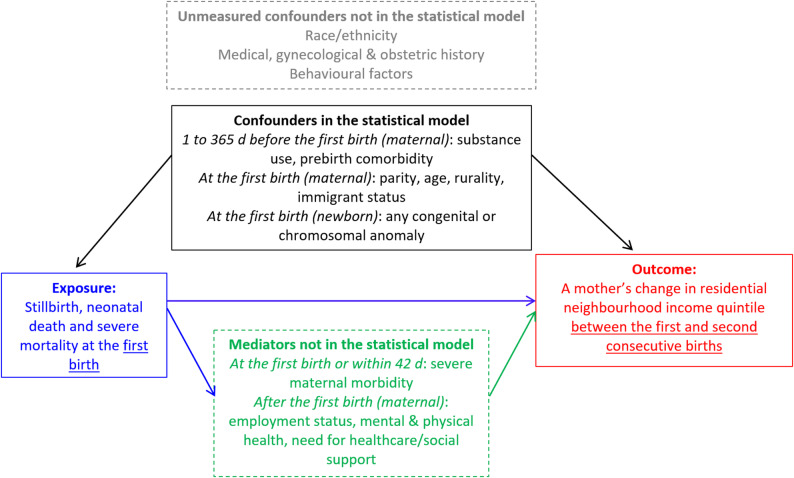 Figure 1
Figure 1- —Keenan Postdoctoral Fellow Scholarship from the St. Michael’s Hospital Foundation
- —Studentship Award from the Edwin S.H. Leong Centre for Healthy Children at the University of Toronto and The Hospital for Sick Children
- —Ontario Academic Health Sciences Centre AFP Innovation Fund
- —https://doi.org/10.13039/501100000024Canadian Institutes of Health Research
- —Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth disparities and outcomes · Global Maternal and Child Health · Family Dynamics and Relationships
Introduction
A birth can create or exacerbate income loss for parents due to child healthcare expenses, [1] workforce absenteeism [2] and the cost of childrearing [3] – together economically termed the ‘child penalty’ [4] – and which can further influence residential affordability. This could be most taxing on women residing in low-income neighbourhoods, with financial instability prior to childbirth [5]. Research indicates that a pregnancy culminating in a stillbirth, neonatal death, or severe neonatal morbidity is associated with maternal postpartum complications, [6] along with profound short- and long-term psychological, social, and economic impacts for both parents [7–9]. Adverse pregnancy events are also more prevalent among those affected by social inequities [7, 10]. Hence, it is plausible that economic challenges may further differ if a woman experiences fetal or neonatal loss, marked by bereavement but no ongoing child-rearing costs thereafter, or has a newborn with transient morbidity followed by a potentially higher economic burden [11] (Fig. 1).
Fig. 1. Conceptual diagram used in the current study for how stillbirth, neonatal death or severe morbidity occurring at the first birth might be associated with a mother’s subsequent change in residential neighbourhood income quintile between the first and consecutive second births
This study assessed whether a stillbirth, neonatal death or severe neonatal morbidity is associated with a mother’s subsequent change in residential neighbourhood income between two consecutive births.
Methods and data analysis
This population-based cohort study was completed using linked administrative datasets in Ontario, Canada (Table S1), where universal healthcare exists. Included were all mothers with two consecutive births at 20–42 weeks’ gestation, from April 1, 2003, to March 31, 2023 (Table S2). The online Supporting Information contains details of all methods, study variables, and analyses. The STROBE reporting guideline was followed.
The study exposure ─ an adverse perinatal event -- comprised four mutually exclusive groups at the first of two consecutive births in the study period: (i) livebirth unaffected by severe neonatal morbidity or neonatal death (referent); (ii) livebirth with severe neonatal morbidity but no neonatal death; (iii) livebirth with neonatal death; and (iv) stillbirth. Severe neonatal morbidity and neonatal death were assessed from the index birth hospitalization up to 27 days thereafter, with severe morbidity defined using a validated composite measure of serious newborn health issues [12].
The study outcome was a mother’s change in residential neighbourhood income quintile (Q) between two consecutive births, representing four exclusive mobility patterns: (i) downward income mobility, (ii) upward income mobility, or (iii) persistently residing in the lowest income Q1 at each birth -- each relative to (iv) no change in neighbourhood income Q between births (referent). The latter two exposure groups were categorized separately as they likely comprise mothers with different economic circumstances, especially since persistent residence in a lowest income neighbourhood would be indicative of long-term area-level economic instability.
Descriptive statistics (i.e., mean and median values and proportions) were contrasted by the adverse perinatal exposure states at the first birth. Multinomial logistic regression generated odds ratios (aORs) and 95% confidence intervals (CI) for the primary outcome of a mother’s change in neighbourhood income Q between two consecutive births in relation to the study exposure of an adverse perinatal event at the first birth.
Statistical models were adjusted for the following maternal and newborn characteristics: substance use (opioid, cocaine, stimulant, or alcohol use) 1 year before the first birth, number of prebirth comorbidities 1 year before the first birth, maternal age at the first birth, livebirth parity at the first birth, rurality at the first birth, immigrant status, and any newborn congenital or chromosomal anomaly identified within the first birth hospitalization.
Results
Of the 720,119 mothers, whose mean (SD) age was 28.6 (4.8) years at the first recorded birth, 669,232 (92.9%) had a livebirth without severe neonatal morbidity or neonatal death, 44,251 (6.1%) had a livebirth with severe neonatal morbidity but no neonatal death, 1756 (0.24%) had a livebirth with neonatal death, and 4880 (0.68%) had a stillbirth (Table 1).
Table 1. Maternal and fetal/newborn characteristics by pregnancy outcomes at the first birth among 720,119 women who had two consecutive births in Ontario, Canada, 2003 to 2023. Data are presented as a number (%) unless otherwise indicatedCharacteristicLivebirthwithout severe neonatal morbidity or neonatal death(N = 669,232)Livebirth with severe neonatal morbidity without neonatal death^a^(N = 44,251)Livebirthwith neonatal death^b^(N = 1756)Stillbirth^c^(N = 4880) Maternal, 1 to 365 days before the first birth Number of pre-birth comorbidities^d^ * 0–2* 619,320 (92.5)39,848 (90.1)1528 (87.0)4349 (89.1) * ≥ 3* 49,912 (7.5)4403 (10.0)228 (13.0)531 (10.9)Substance use (opioid, cocaine, stimulant or alcohol use)^e^18,352 (2.7)2028 (4.6)87 (5.0)239 (4.9)Maternal,** at the first birthMean (SD), Age, years28.6 (4.8)28.7 (4.9)29.4 (5.4)30.0 (5.4)Neighbourhood income quintile, Q * Q1 (Lowest)* 141,061 (21.1)9252 (20.9)450 (25.6)1276 (26.2) * Q2* 135,799 (20.3)9012 (20.4)415 (23.6)1000 (20.5) * Q3* 140,757 (21.0)9510 (21.5)348 (19.8)1019 (20.9) * Q4* 141,685 (21.2)9461 (21.4)321 (18.3)925 (19.0) Q5 (Highest) 109,930 (16.4)7016 (15.9)222 (12.6)660 (13.5)Parity * 0–1* 624,654 (93.3)41,969 (94.8)1552 (88.4)4260 (87.3) * ≥ 2* 44,578 (6.7)2282 (5.2)204 (11.6)620 (12.7)Rural residence68,070 (10.2)4415 (10.0)180 (10.3)476 (9.8)Non-refugee immigrant159,328 (23.8)9558 (21.6)454 (25.9)1373 (28.1)Fetus or newborn, at the first birthFemale sex328,950 (49.1)18,662 (42.2)785 (44.7)61 (1.2) * Sex missing* 0 (0.0)0 (0.0)0 (0.0)4745 (97.2)Gestational age at birth, mean (SD), weeks39.2 (1.4)37.3 (3.7)29.2 (7.4)30.2 (7.1)Preterm livebirth or stillbirth < 37 weeks’ gestation27,818 (4.2)13,057 (29.5)1254 (71.1)3441 (70.5)Any congenital or chromosomal anomaly17,801 (2.7)6306 (14.3)544 (31.0)Not reportedMedian IQR**,** number of months between the first & second births**,** years**32 (24–47)32 (24–46)20 (14–32)19 (14–30)^a^Arising in the index birth admission or within 27 days thereafter^b^Arising in the index birth admission or within 27 days thereafter^c^A fetal death arising in utero, or a newborn with no signs of life at birth, at ≥ 20 weeks’ gestation^d^Total number of Johns Hopkins Adjusted Clinical Group (ACG)^®^ System Aggregated Diagnosis Groups (ADG) (excluding “pregnancy” diagnosis), 1 to 365 days before the first birth hospitalization^e^Type of substance use, 1 to 365 days before the first birth hospitalization is suppressed due to small cell sizes ≤ 5
Among mothers initially residing in income areas Q2-Q5, relative to those with an unaffected livebirth, there was a higher likelihood of downward income mobility between births if their child was affected by non-fatal severe neonatal morbidity (aOR 1.05, 95% CI 1.02–1.08), with no tendencies for upward income mobility (Table 2). However, significantly lower aORs were observed for experiencing downward or upward income mobility between births if they had a neonatal death or a stillbirth.
Table 2. Odds of a mother exclusively experiencing downward or upward income mobility between two consecutive births, or otherwise persistently residing in neighbourhood income quintile 1 (Q1) between two successive births, each in relation to having a newborn affected by a stillbirth, neonatal death or severe neonatal morbidity at the first recorded birth. Data are limited to women who had two recorded consecutive Singleton hospital births at 20^0/7^ to 42^0/7^ weeks’ gestation in Ontario, Canada, 2003 to 2023Outcome occurring between consecutive birthsDownward income mobilityUpward income mobilityPersistently residing in Q1 Exposure at the first birth
No. (%) with
outcome
Adjusted
odds ratio
(95% CI) ^e, f^
No. (%) with
outcome
Adjusted
odds ratio
(95% CI) ^e, f^
No. (%) with
outcome
Adjusted
odds ratio
(95% CI) ^e, f^
Livebirth without severe neonatal morbidity or neonatal death
(N = 669,232) ^a^ 122,443 (18.3)1 (Reference)168,199 (25.1)1 (Reference)79,465 (11.9)1 (Reference) Livebirth with severe neonatal morbidity without death (N = 44,251)^b^8343 (18.9) 1.05 (1.02 to 1.08) 11,000 (24.9)1.01 (0.99 to 1.04)5241 (11.8) 1.05 (1.01 to 1.08)
Livebirth with neonatal death
(N = 1756) ^c^ 294 (16.7) 0.86 (0.75 to 0.99) 326 (18.6) 0.71 (0.62 to 0.81) 301 (17.1) 1.29 (1.12 to 1.48)
*Stillbirth *
(N = 4880) ^d^ 734 (15.0) 0.77 (0.71 to 0.84) 837 (17.2) 0.64 (0.59 to 0.69) 893 (18.3) 1.35 (1.24 to 1.46) ^a^299,125 (44.7%) of mothers had no income mobility between two consecutive births, except those shown with persistent Q1^b^19,667 (44.4%) of mothers had no income mobility between two consecutive births, except those shown with persistent Q1^c^835 (47.6%) of mothers had no income mobility between two consecutive births, except those shown with persistent Q1^d^2416 (49.5%) of mothers had no income mobility between two consecutive births, except those shown with persistent Q1^e^Multinomial logistic regression, adjusted for substance use within 1 to 365 days before the first birth hospitalization, number of pre-birth comorbidities within 1 to 365 days before the first birth hospitalization (≥ 3 vs. 0–2), age at the first birth hospitalization (15–19, 20–24, 30–34, ≥ 35, vs. 25–29 years), parity (≥ 2 vs. 0–1), residence at the first birth hospitalization (rural vs. urban), immigrant status (non-refugee immigrant vs. non-immigrant), and any newborn congenital or chromosomal anomaly during the first birth hospitalization^f^An adjusted odds ratio < 1 indicates a lower tendency for downward (or upward) income mobility, and an odds ratio > 1 reflects a higher tendency for such movement
Among mothers initially residing in income Q1, the aOR for remaining in income Q1 was 1.05 (95% CI 1.01–1.08) following a livebirth affected by severe neonatal morbidity, 1.29 (95% CI 1.12–1.48) after a neonatal death, and 1.35 (95% CI 1.24–1.46) after a stillbirth – each compared to mothers with an unaffected livebirth (Table 2).
Discussion
Mothers with a newborn affected by severe morbidity were more likely to have a decline in neighbourhood income Q, or to persist in the lowest-income area. Those experiencing a stillbirth or neonatal death were more likely to remain in the same neighbourhood income quintile at a subsequent birth (i.e., having no income mobility across births).
Study limitations include a lack of information on a mother’s individual-level income, profession, race, or details about the non-birthing parent, and other unmeasured confounders included in Fig. 1. Individual income changes may not correspond with neighbourhood income mobility. While the current study accounted for livebirth bias at the first birth, survivorship selection bias was likely introduced by the study design, necessitating having a second birth for cohort entry [13]. Maternal peripartum morbidity was not included as a confounder since it is likely a causal mediator of the relation between the study exposure of an adverse perinatal event at the first birth and the ensuing outcome of a mother’s change in residential neighbourhood income quintile [6, 14].
We propose that the nature of a pregnancy outcome can be a ‘socioeconomic stress test’ for the parent(s). This stress test may be greater if the newborn experiences severe morbidity: it is plausible that the ongoing requirements of parental care for a newborn affected by morbidity can have both physical, mental, and economic ramifications for one or both parents [15, 16]. In contrast, if the fetus or newborn dies, the economic burden on the family may not persist, despite the emotional burden of that loss.
The exception appears to be among those residing in low-income areas, in which a fetal or neonatal morbidity/loss may profoundly affect her socioeconomic trajectory.
Conclusions
Future studies should elucidate the causal pathways between having a pregnancy ending in either a stillbirth, neonatal death, or severe morbidity experience and the various patterns of subsequent neighbourhood income movement. Further research should also investigate whether, following an adverse perinatal event, supports such as financial supplements can help a mother at risk of income decline, especially among those already residing in the lowest income areas preceding an adverse perinatal event.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jairam JA, Vigod S, Siddiqi A, Guan J, Boblitz A, Wang X, O’Campo P, Ray JG. Morbidity and mortality of newborns born to immigrant and nonimmigrant females residing in low-income neighbourhoods. CMAJ. 2023;195(15):E 537–47.10.1503/cmaj.221711 PMC 1011033737068807 · doi ↗ · pubmed ↗
- 2Aoyama K, Park AL, Davidson AJF, Ray JG. Severe maternal morbidity and infant mortality in Canada. Pediatrics 2020;146(3).10.1542/peds.2019-387032817396 · doi ↗ · pubmed ↗
- 3Cimpian DM, Strete GE, Cimpian CI, et al. The Impact of preterm birth on parents’ mental health and the role of family-centred interventions: a narrative review. Child (Basel). 2025;12(10). 10.3390/children 12101311 PMC 1256445841153493 · doi ↗ · pubmed ↗
- 4Nelson CR, Ray JG, Auger N, et al. Neonatal adverse outcomes among hospital livebirths in Canada: a national retrospective study. Neonatology 2024. 10.1159/000540559 PMC 1180951639173602 · doi ↗ · pubmed ↗